

Abstract
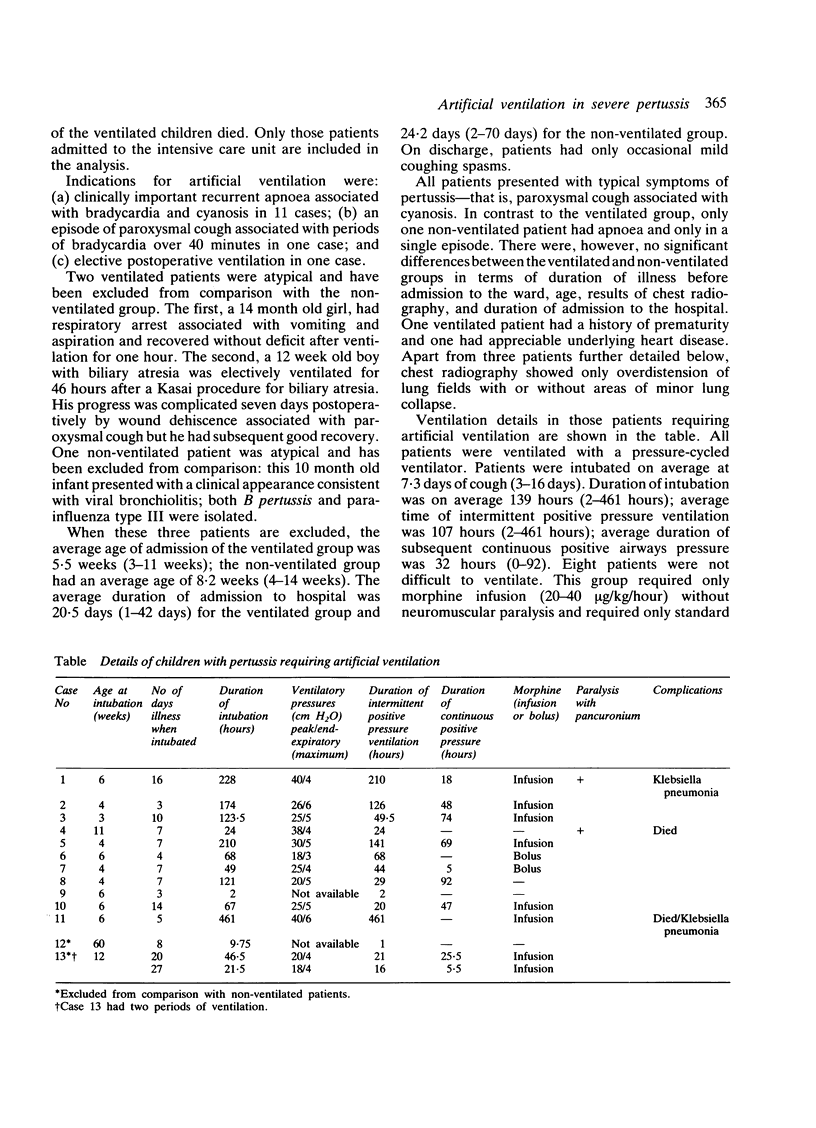
A retrospective review was conducted of all children admitted to our intensive care unit over eight years with a diagnosis of pertussis that had been proved on culture. Altogether 789 children were seen as outpatients and inpatients. Twenty four of these children were admitted to the intensive care unit, 13 of whom required ventilatory support; two of the ventilated patients died. Intubation and ventilation were usually started for appreciable apnoea. Most patients requiring support were less than 3 months of age and required intervention within the first 16 days of cough. For these patients ventilation was neither difficult nor prolonged. Coughing spasms were not a problem and intubation and ventilation appeared to attenuate the progress of the disease. The presence of severe bacterial pneumonia associated with difficult ventilation requiring neuromuscular paralysis indicated a poor prognosis. It is suggested that intubation and ventilation can be safely used in very severe pertussis infection and, because of their greater risk of hypoxic damage and death, it should not be reserved as a last resort in critically ill infants.
Full text
PDF
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Bass J. W. Pertussis: current status of prevention and treatment. Pediatr Infect Dis. 1985 Nov-Dec;4(6):614–619. doi: 10.1097/00006454-198511000-00003. [DOI] [PubMed] [Google Scholar]
- Broomhall J., Herxheimer A. Treatment of whooping cough: the facts. Arch Dis Child. 1984 Feb;59(2):185–187. doi: 10.1136/adc.59.2.185. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Forsyth K., Farmer K., Lennon D. R. High admission rate of infants and young children with whooping cough: clinical aspects and preventive implications. Aust Paediatr J. 1984 May;20(2):101–103. doi: 10.1111/j.1440-1754.1984.tb00053.x. [DOI] [PubMed] [Google Scholar]
- Lewis M., Bush G. H. Ventilatory support for children with whooping cough. Experience with children admitted to a paediatric intensive care unit. Anaesthesia. 1980 Oct;35(10):979–983. doi: 10.1111/j.1365-2044.1980.tb04996.x. [DOI] [PubMed] [Google Scholar]
- Miller C. L., Fletcher W. B. Severity of notified whooping cough. Br Med J. 1976 Jan 17;1(6002):117–119. doi: 10.1136/bmj.1.6002.117. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nkowane B. M., Wassilak S. G., McKee P. A., O'Mara D. J., Dellaportas G., Istre G. R., Orenstein W. A., Bart K. J. Pertussis epidemic in Oklahoma. Difficulties in preventing transmission. Am J Dis Child. 1986 May;140(5):433–437. doi: 10.1001/archpedi.1986.02140190043021. [DOI] [PubMed] [Google Scholar]
- Robinson D. A., Mandal B. K., Ironside A. G., Dunbar E. M. Whooping cough--a study of severity in hospital cases. Arch Dis Child. 1981 Sep;56(9):687–691. doi: 10.1136/adc.56.9.687. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sims D. G., Downham M. A., McQuillin J., Gardner P. S. Respiratory syncytial virus infection in north-east England. Br Med J. 1976 Nov 6;2(6044):1095–1098. doi: 10.1136/bmj.2.6044.1095. [DOI] [PMC free article] [PubMed] [Google Scholar]