

Abstract
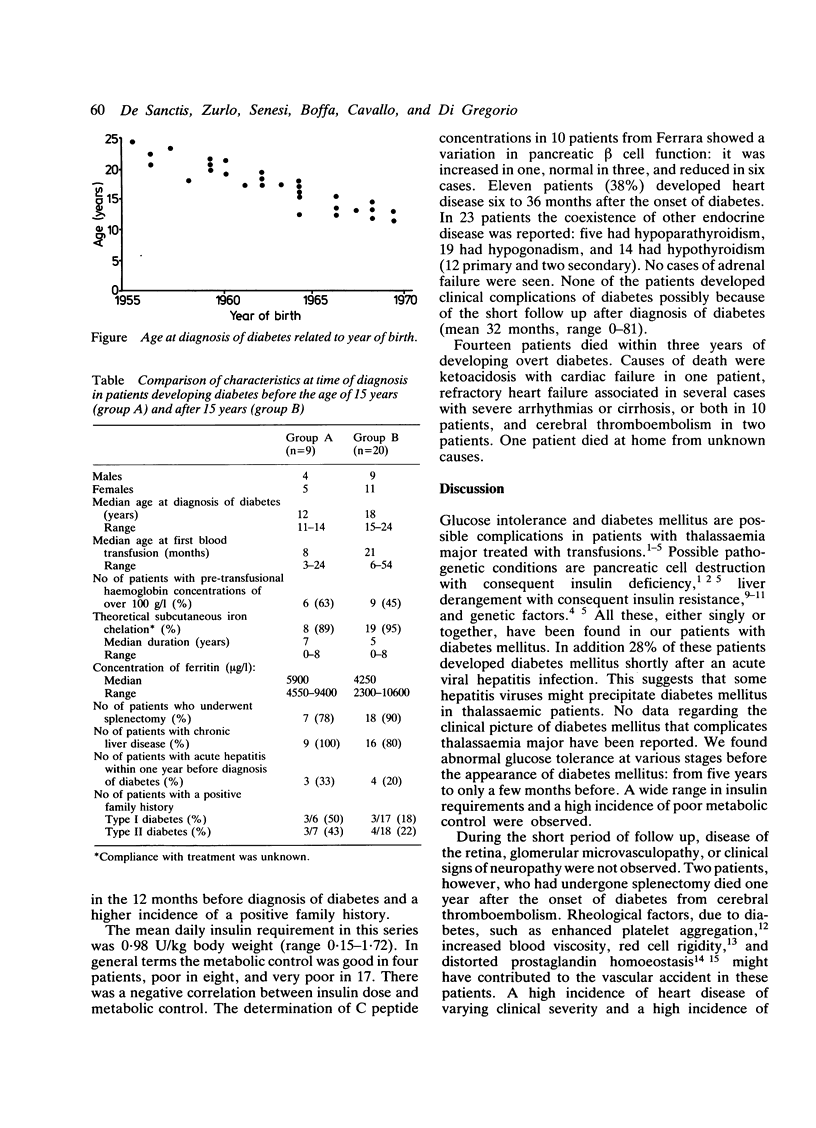
Diabetes mellitus was observed in 29 of 448 patients with thalassaemia major attending seven Italian centres. Twelve patients, at onset of clinical diabetes, presented with an asymptomatic glycosuria, 13 with ketosis, and four with ketoacidosis. All were diagnosed after 1979, at a mean age of 17 years. Mean age at diagnosis of diabetes was lower in patients born in the last two decades. In these patients transfusions were started at a younger age and pre-transfusion haemoglobin concentration, serum ferritin concentration, incidence of liver disease, and the presence of a family history of diabetes were higher than in patients born previously. Although 27 (93%) cases had iron chelating treatment the mean serum ferritin concentration was 5600 micrograms/l; 25 (92%) of these patients had signs of liver impairment. The determination of C peptide in 10 patients showed a wide variation in pancreatic beta cell function, and insulin requirements ranged between 0.15 and 1.72 U/kg body weight. Metabolic control was generally poor. The onset of diabetes mellitus was followed in most patients by the appearance of other endocrine or cardiac complications, or both. Fourteen patients died within three years of presenting with overt diabetes. Haemosiderosis, liver infections, and genetic factors seemed to be crucial in diabetes development. Thalassaemic patients developing clinical diabetes mellitus are at high risk for other complications and should be strictly monitored, especially for thyroid impairment.
Full text
PDF


Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Addison G. M., Beamish M. R., Hales C. N., Hodgkins M., Jacobs A., Llewellin P. An immunoradiometric assay for ferritin in the serum of normal subjects and patients with iron deficiency and iron overload. J Clin Pathol. 1972 Apr;25(4):326–329. doi: 10.1136/jcp.25.4.326. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Costin G., Kogut M. D., Hyman C., Ortega J. A. Carbohydrate metabolism and pancreatic islet-cell function in thalassemia major. Diabetes. 1977 Mar;26(3):230–240. doi: 10.2337/diab.26.3.230. [DOI] [PubMed] [Google Scholar]
- Dandona P., Hussain M. A., Varghese Z., Politis D., Flynn D. M., Hoffbrand A. V. Insulin resistance and iron overload. Ann Clin Biochem. 1983 Mar;20(Pt 2):77–79. doi: 10.1177/000456328302000203. [DOI] [PubMed] [Google Scholar]
- De Sanctis V., D'Ascola G., Wonke B. The development of diabetes mellitus and chronic liver disease in long term chelated beta thalassaemic patients. Postgrad Med J. 1986 Sep;62(731):831–836. doi: 10.1136/pgmj.62.731.831. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Flynn D. M., Fairney A., Jackson D., Clayton B. E. Hormonal changes in thalassaemia major. Arch Dis Child. 1976 Nov;51(11):828–836. doi: 10.1136/adc.51.11.828. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gabutti V., Piga A., Nicola P., Vullo C., Capra L., Di Palma A., Masera G., Terzoli S., Mauri R. Haemoglobin levels and blood requirement in thalassaemia. Arch Dis Child. 1982 Feb;57(2):156–158. doi: 10.1136/adc.57.2.156. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hecht A., Gershberg H. Diabetes mellitus and primary hypothyroidism. Metabolism. 1968 Feb;17(2):108–113. doi: 10.1016/0026-0495(68)90136-4. [DOI] [PubMed] [Google Scholar]
- Hockaday T. D. Direct animal and indirect human evidence of altered platelet function in diabetics. Metabolism. 1979 Apr;28(4 Suppl 1):415–422. doi: 10.1016/0026-0495(79)90048-9. [DOI] [PubMed] [Google Scholar]
- Lassman M. N., Genel M., Wise J. K., Hendler R., Felig P. Carbohydrate homeostasis and pancreatic islet cell funtion in thalassemia. Ann Intern Med. 1974 Jan;80(1):65–69. doi: 10.7326/0003-4819-80-1-65. [DOI] [PubMed] [Google Scholar]
- McIntosh N. Endocrinopathy in thalassaemia major. Arch Dis Child. 1976 Mar;51(3):195–201. doi: 10.1136/adc.51.3.195. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Propper R. D., Button L. N., Nathan D. G. New approaches to the transfusion management of thalassemia. Blood. 1980 Jan;55(1):55–60. [PubMed] [Google Scholar]
- Saudek C. D., Hemm R. M., Peterson C. M. Abnormal glucose tolerance in beta-thalassemia major. Metabolism. 1977 Jan;26(1):43–52. doi: 10.1016/0026-0495(77)90126-3. [DOI] [PubMed] [Google Scholar]
- Schmid-Schönbein H., Volger E. Red-cell aggregation and red-cell deformability in diabetes. Diabetes. 1976;25(2 Suppl):897–902. [PubMed] [Google Scholar]
- Silberbauer K., Schernthaner G., Sinzinger H., Piza-Katzer H., Winter M. Decreased vascular prostacyclin in juvenile-onset diabetes. N Engl J Med. 1979 Feb 15;300(7):366–367. [PubMed] [Google Scholar]
- Zuppinger K., Molinari B., Hirt A., Imbach P., Gugler E., Tönz O., Zurbrügg R. P. Increased risk of diabetes mellitus in beta- thalassemia major due to iron overload. Helv Paediatr Acta. 1979;34(3):197–207. [PubMed] [Google Scholar]