

Abstract
We estimated rates of intimate partner violence and related injuries in a sample of 1371 women aged 18 to 49 years in Yokohama, Japan. By the age of 30 years, 14.3% of women who had ever had a partner had experienced violence from that partner, and 3.3% had suffered injuries related to such violence. By the time women had reached the age of 49 years, these percentages were 19% and 4%, respectively. In addition to the need for increased prevention efforts, our findings indicate the need for an expanded legal definition of intimate partner violence in Japan given that the current definition excludes premarital violence.
Intimate partner violence (IPV) cuts across national, cultural, and socioeconomic boundaries and is a cause of serious social concern as well as health concern worldwide.1,2 In Japan, only recently has IPV been recognized as a grave social issue,3,4 and this overdue recognition largely has been the result of grassroots research and advocacy efforts.5,6 Legal responses in the country remain under-developed; for example, the 2001 Domestic Violence Prevention Act (Law No. 31) does not include partner violence outside marriage as grounds for court-issued protection orders; its 2004 amendment recognizes postdivorce partner violence, but not IPV before marriage, as grounds for protection orders.
We investigated rates of IPV and IPV-related injury among Japanese women of various ages as part of the Multi-Country Study on Women’s Health and Domestic Violence Against Women, coordinated by the World Health Organization (WHO) in 2000–2001.7 The goal of the WHO study was to obtain population-based data on IPV prevalence and women’s health using the same methodologies and instruments across different parts of the world. Participating countries were Bangladesh, Brazil, Ethiopia, Japan, Namibia, Peru, Samoa, Serbia and Montenegro, Thailand, and the United Republic of Tanzania.
METHODS
Our group translated version 9.9 of the WHO Core Questionnaire8 into Japanese and augmented it with questions pertinent to Japanese sociocultural contexts. The study’s stratified cluster sample, which included women aged 18 to 49 years who resided in Yokohama, was designed to be self-weighted (for further details, see the WHO Japan country report9). Of the 2400 women selected to participate, 1371 (57%) completed the interview. This response rate compared favorably with rates from other face-to-face interview studies conducted in Japan; for example, in a previous study, the response rate for the 6 largest cities in Japan, including Yokohama, was 49%.12
Respondents were asked about 6 forms of physical IPV and 3 forms of sexual IPV experienced at the hands of their partners (Table 1 ▶). In addition, they were asked their age at the time of the event and whether or not they had incurred any injuries.
TABLE 1—
Experiences of Physical and Sexual Intimate Partner Violence (IPV) and IPV-Related Injuries Among Women: Yokohama, Japan
| Sample % (95% Confidence Interval) | |
| Physical IPV | |
| Slapped/object thrown at | 9.0 (7.4, 10.6) |
| Pushed or shoved | 8.4 (6.8, 10.2) |
| Hit with fist or with something else that could cause pain/injury | 2.2 (1.4, 3.0) |
| Kicked, dragged, or beaten | 2.6 (1.7, 3.4) |
| Choked or burned deliberately | 0.1 (0.0, 0.3) |
| Threatened or assaulted with gun, knife, or other weapon | 0.6 (0.1, 0.9) |
| Any type of physical IPV | 12.6 (10.9, 14.3) |
| Probability of physical IPV by age 49 y | 16.1 (13.7, 18.8) |
| Sexual IPV | |
| Physically forced to have sexual intercourse without consent | 5.1 (3.6, 6.5) |
| Had sexual intercourse because of fear of what partner might do | 3.3 (2.3, 4.3) |
| Forced to engage in a degrading or humiliating sexual act | 1.4 (0.6, 2.1) |
| Any type of sexual IPV | 6.4 (4.8, 8.0) |
| Probability of sexual IPV by age 49 y | 8.1 (6.3, 10.5) |
| Physical and sexual IPV | |
| Any physical or sexual IPV reported | 15.1 (13.1, 17.0) |
| Probability of physical or sexual IPV by age 49 y | 19.0 (16.4, 22.0) |
| Any IPV | |
| Any IPV-related injury | 3.5 (2.4, 4.5) |
| Probability of IPV-related injury by age 49 y | 4.0 (3.0, 5.4) |
Note. Analyses were based on 1287 women who had been involved in at least 1 heterosexual relationship before the time of the interview.
We used Stata 8.1 (Stata Corp, College Station, Tex) to conduct the analyses. We used poststratification weights to account for different response rates among subgroups10 determined by age, marital status, and employment status. We used survey methods that adjust variance estimates to account for the stratification and clustering in the sampling design. We estimated cumulative incidence functions and IPV and IPV-related-injury hazards using survival analysis methods. (At age t, the cumulative incidence function represented the probability that IPV or an injury had occurred at or before age t, and the hazard function represented the instantaneous risk of IPV or injury being experienced at age t given no IPV or injury up to that time.)
RESULTS
Of the 1371 respondents (mean age = 35.2 years), 1287 had been involved in at least 1 intimate heterosexual relationship. The distributions of respondents’ characteristics were comparable to those of Yokohama women aged 18 to 49 years as a whole with respect to age, educational level, and marital status (Japanese Institute of Nuclear Safety, unpublished data, 1994).11,12
As shown in Table 1 ▶, 12.6% of women who had ever had a partner reported having experienced physical IPV at some point in their past, 6.4% reported having experienced sexual IPV, and 15.1% reported either physical or sexual IPV or both. Women were most likely to experience their first episode of IPV before the age of 30 years, as evidenced by the steeper slope of the cumulative incidence function during this period (Figure 1 ▶). Approximately 14% of women (95% confidence interval [CI] = 12.3%, 16.5%) were estimated to have experienced IPV by the age of 30 years and 19% (95% CI = 16.4%, 22.0%) by the age of 49 years. The hazard function associated with experiencing IPV for the first time rose consistently from the late adolescent years until the age of 30 years, decreased sharply at the age of 30 years, and leveled off thereafter.
FIGURE 1—
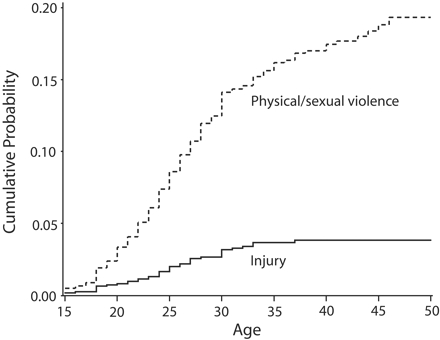
Cumulative probabilities of intimate partner violence (IPV) and IPV-related injuries among women residing in Yokohama, Japan.
Among women who had experienced IPV, almost one fourth (24.4%; 95% CI = 17.6%, 31.2%) had been injured, and more than one third (34.9%; 95% CI = 21.5%, 48.3%) of these injured women had been injured more than twice. Estimated probabilities of women having experienced IPV-related injuries were 3.3% (95% CI = 2.4%, 4.6%) by the time they were aged 30 years and 4.0% (95% CI = 3.0%, 5.4%) by the time they were aged 49 years.
DISCUSSION
We estimated that, by the age of 49 years, 1 in 5 women in Yokohama had experienced IPV, and 4% had sustained IPV-related injuries. Most had experienced IPV or sustained IPV-related injuries early in their adult lives: 14% had experienced IPV and 3% IPV-related injury by age 30 years, the average age at which women in metropolitan areas of Japan marry for the first time.13 The risk of experiencing IPV and IPV-related injury rose steadily until just before the age of 30 years.
The major limitation of this study was the low response rate. Although we used poststratification weights, it is still possible that rates of IPV and IPV-related injuries were higher or lower among respondents than among nonrespondents. In addition, the sample was limited to an urban region of Japan, and we have no way of determining whether our results would be generalizable to rural regions.
Nevertheless, the findings of this study clearly suggest the importance of targeting both married and unmarried young adults and developing policies and prevention and intervention programs designed to address IPV in women aged 18 to 49 years. However, as mentioned, current Japanese law does not include IPV occurring before marriage in its criteria for protection orders, leaving women in such situations with limited recourse. Premarital IPV should be included in Japan’s legal definition of IPV, and intervention programs must target all women at risk regardless of their marital status.
Acknowledgments
This study was funded in part by grants from the World Health Organization (grant W6/181/21); the Toyota Foundation (grant 9882-064); the Japan Ministry of Health and Welfare (grant H10-kodomo-015); the University of Michigan’s Center for Japanese Studies, Institute for Research on Women and Gender, and School of Social Work; the Japan National Institute of Population and Social Security Research; and the National Sciences and Engineering Research Council of Canada (NSERC Discovery grant 261497-03).
We would like to thank the study participants, who willingly shared their experiences of intimate partner violence and health conditions. Special thanks also go to the Japan project team members (Hiroko Aikyama, Tamie Kaino, Fumi Hayashi, and Tomoko Yunomae).
Human Participant Protection This study was approved by the institutional review boards of the University of Michigan and the World Health Organization. Participants provided informed consent.
Peer Reviewed
Contributors M. Yoshihama and S. Kamano developed and implemented the study. J. Horrocks assisted with analyses. All of the authors contributed to conceptualization of the article’s focus, interpretation of findings, and the writing of the article.
References
- 1.World Health Organization. Fact sheet: intimate partner violence. 2002. Available at: http://www.who.int/violence_injury_prevention/violence/global_campaign/en/ipvfacts.pdf. Accessed October 26, 2006.
- 2.Campbell JC. Health consequences of intimate partner violence. Lancet. 2002;359:1331–1336. [DOI] [PubMed] [Google Scholar]
- 3.Yoshihama M. Policies and services addressing domestic violence in Japan: from non-interference to incremental changes. Womens Stud Int Forum. 2002; 25:541–553. [Google Scholar]
- 4.Yoshihama M. The definitional process of domestic violence in Japan: generating official response through action-oriented research and international advocacy. Violence Against Women. 2002;7:339–366. [Google Scholar]
- 5.Yoshihama M. Domestic violence in Japan: research, program development and emerging movements. In: Roberts A, ed. Battered Women and Their Families: Intervention Strategies and Treatment Programs. 2nd ed. New York, NY: Springer Publishing Co; 1998: 405–447.
- 6.Hattori N, Kaino T, Tsunoda Y, et al. Otto kara tsuma eno boryoku: koninkankei no naigaide [A study on husbands’ (boyfriends’) violence in Japan: preliminary findings]. Joseigaku Kenkyu. 1995;3:122–139. [Google Scholar]
- 7.WHO Multi-Country Study on Women’s Health and Domestic Violence Against Women: Summary Report of Initial Results on Prevalence, Health Outcomes and Women’s Responses. Geneva, Switzerland: World Health Organization; 2005.
- 8.WHO Multi-Country Study on Women’s Health and Domestic Violence: Core Questionnaire and WHO Instrument—Version 9. Geneva, Switzerland: World Health Organization; 2000.
- 9.WHO Multi-Country Study on Women’s Health and Domestic Violence Against Women—Japan Country Report. Tokyo, Japan: Japan Project Team, WHO Multi-Country Study on Women’s Health and Domestic Violence Against Women; 2005.
- 10.Sarndal CE, Lundstrom S. Estimation in Surveys With Nonresponse. New York, NY: John Wiley & Sons Inc; 2005.
- 11.Heisei 14 Nen Shugyo Kozo Kihon Chosa [The Employment Status Survey of 1997]. Tokyo, Japan: Somucho Tokeikyoku; 1998.
- 12.Kokuminsei No Kenkyu Dai 10 Ji Zenkoku Chosa—1998 Nen Zenkoku Chosa [A study of the Japanese national character: the Tenth Nationwide Survey]. Tokyo, Japan: Tokei Suri Kenkyujo; 1999.
- 13.Kokuritsu Shakaihosho Jinko Mondai Kenkyujo. Jinko Tokei Shiryoshu [Latest demographic statistics]. Tokyo, Japan: Tokei Insatsu Kogyo; 2003.