

Abstract
Objectives. Research on child labor and its effect on health has been limited. We sought to determine the impact of child labor on children’s health by correlating existing health indicators with the prevalence of child labor in selected developing countries.
Methods. We analyzed the relationship between child labor (defined as the percentage of children aged 10 to14 years who were workers) and selected health indicators in 83 countries using multiple regression to determine the nature and strength of the relation. The regression included control variables such as the percentage of the population below the poverty line and the adult mortality rate.
Results. Child labor was significantly and positively related to adolescent mortality, to a population’s nutrition level, and to the presence of infectious disease.
Conclusions. Longitudinal studies are required to understand the short- and long-term health effects of child labor on the individual child.
Child labor is an important global issue associated with poverty, inadequate educational opportunities, gender inequality, and a range of health risks.1 Child labor is defined by the relevant international conventions (UNICEF’s Convention on the Rights of the Child,2 International Labor Organization [ILO] Convention 138,3 and especially, 1824) not by the activities performed by the child, but by the consequences of such activities (exceptions are the so-called unconditional worst forms of child labor such as prostitution and bondage, as noted in ILO Convention 182). For instance, work affecting a child’s health and schooling should, according to these conventions, be eliminated.5 Identifying the health effects of child labor is essential because it enables policymakers to decide which types of child labor to target for eradication.
The ILO estimates that there are approximately 250 million child laborers worldwide, with at least 120 million of them working under circumstances that have denied them a childhood and in conditions that jeopardize their health and even their lives. Most working children are ages 11 to 14 years old, but as many as 60 million are between the ages of 5 and 11.6 Although the exact numbers are not known, available statistics indicate that approximately 96% of child workers reside in developing countries in Africa, Asia, and Latin America; there are also pockets of child labor in many industrialized countries.5,7,8 In spite of a reported decline in child labor during the period 1995 to 2000,9 child labor remains a major concern.
Most child laborers begin working at a very young age, are malnourished, and work long hours in hazardous occupations; frequently they do not attend school. They receive very low wages or are unpaid, and their income or help is usually essential for family survival. They are mainly employed in the informal sector, with agriculture accounting for more children workers than any other sector. It is estimated that, in developing countries, at least 90% of economically active children in rural areas are employed in agriculture.10 Recent ILO statistics from 20 developing countries categorized the proportion of economically active children aged 5 to 14 years as employed in agriculture, animal husbandry, and related work at 74% (73.3% of boys and 78.8% of girls).11
Short term, the most obvious economic impact of child labor at the family level is an increase in household income. Long term, the underaccumulation of human capital caused by low school attendance and poor health is a serious negative consequence of child labor, representing a missed opportunity to enhance the productivity and future earnings capacity of the next generation.12 Child laborers grow up to be low-wage–earning adults; as a result, their offspring will also be compelled to work to supplement the family’s income. In this way, poverty and child labor is passed from generation to generation.13,14
Although child labor is recognized as a global health problem, research on its health impact on children has been limited and sometimes inconsistent. In 1998, Graitcer and Lerer published the first comprehensive review of the effect of child labor on children’s health by extrapolating data from the Global Burden of Disease Study.15 The occupational mortality rate among children matched the adult occupational mortality rate, such that the occupational mortality rate indicates mortality associated with child labor. In another study, in 2000, Graitcer and Lerer did not find any differences in the health status of working and nonworking Egyptian children in the short run (the children were not followed to adulthood).16 A 2003 report on children’s work in Morocco,17 Yemen,18 and Guatemala,19 and a review developed under the aegis of Understanding Children’s Work Project20 provide an overview of the nature and extent of child labor, its determinants, and its consequences for the health and education of children in these countries. Several case–control and cohort studies have reported on the association of child labor, impaired growth, and malnutrition.21–26
The health effects of child labor on children and the correlation between current health and future health status are difficult to investigate and are compounded by short-term versus long-term health consequences. The situation is further complicated because work can contribute to an improvement in a poor child’s nutritional status (a positive health effect).14 Finally, the anthropometric measurements that traditionally have been used to evaluate children’s health status are of limited value for those who are age 10 years and older.
We provide evidence, garnered from a cross section of countries, on the relation between child labor and children’s health. To our knowledge, this study represents the first use of cross-country data to examine the issue. The benefit of cross-country data is that they allow us to synthesize indicators, creating a set of indicators unavailable in micro- or individual-country data. The drawback to using different data sources is that the statistics may not be comparable. To avoid problems of comparability, we limited ourselves to data that were standardized by the institutions that collected or compiled them. We analyzed the health effects of child labor on children by correlating existing health indicators and the prevalence of child labor in a large group of developing countries (Algeria, Angola, Bangladesh, Belize, Benin, Bolivia, Botswana, Brazil, Burkina Faso, Burundi, Cambodia, Cameroon, Chad, Chile, China, Congo, Colombia, Cote d’Ivoire, Costa Rica, Democratic Republic of Congo, Dominican Republic, Egypt, Ecuador, El Salvador, Eritrea, Gabon, Gambia, Ghana, Guatemala, Guinea, Guinea Bissau, Haiti, Honduras, India, Indonesia, Iran, Iraq, Jamaica, Jordan, Kenya, Laos, Liberia, Libya, Lesotho, Madagascar, Malaysia, Malawi, Mali, Mexico, Mongolia, Mozambique, Morocco, Myanmar, Namibia, Nepal, Nicaragua, Niger, Nigeria, Oman, Pakistan, Panama, Papua New Guinea, Paraguay, Peru, Philippines, Rwanda, Senegal, Sierra Leone, Solomon’s Islands, Sri Lanka, Sudan, Swaziland, Syrian Arab Republic, Uganda, Uruguay, Tanzania, Venezuela, Vietnam, Thailand, Togo, Yemen, Zambia, Zimbabwe).
METHODS
Data and Indicator Sources
We derived our estimates on the prevalence of child labor among children aged 10 to 14 years from only 1 data set: the World Bank’s World Development Indicators.27 This source limits its estimates of working children to the “economically active population,” which means that children who are in non economic activities or are employed in hidden forms of work such as domestic service, prostitution, and armed conflict are not included.
Health indicators, such as health status, and health determinant indicators, which give information about the health of a community or population relative to some criteria or in comparison with other communities or populations, were obtained from the World Development Indicators, the Global Burden of Disease Study,28 and the life tables for 191 countries (our study included only the 83 developing countries).29
The following rates and percentages were obtained from the World Bank database: male and female adult mortality rates, fertility rates, the prevalence of undernourishment (percentage of population), the prevalence of HIV/AIDS among adults (percentage of population), and national poverty levels (percentage of population below the national poverty line, as determined using the World Bank’s country poverty assessments).
The World Bank’s data set came from multitopic welfare surveys, such as the Living Standard Measurement Study (LSMS), which measure and analyze poverty. Dozens of countries have implemented multitopic surveys, and many of them have conducted the same survey repeatedly, allowing for relevant comparisons across time. Multitopic surveys can also be used to measure the effect of public policies and programs on poverty. The LSMS—one of the best known and most useful of these surveys—has a questionnaire designed to study multiple aspects of household welfare and behavior; it also incorporates extensive quality-control features. The main objective of LSMS surveys is to collect household data that can be used to assess household welfare, understand household behavior, and evaluate the effect of various government policies on the quality living conditions of the population. Accordingly, LSMS surveys collect information on employment, household income and expenditures; asset ownership, such as housing or land; health; education; fertility; nutrition; migration; and access to services and social programs. To minimize errors and delays in data processing, LSMS surveys are implemented with distinct procedures that resolve most inconsistencies in the raw data before the data reach the central statistical office.
Data on HIV/AIDS infections, non-HIV infections, and malaria among children aged 5 to 14 years, associated with 4 major risk factors (malnutrition, poor water and lack of sanitation and hygiene, unsafe sex, and dangerous occupation), came from the Global Burden of Disease Study. These indicators are expressed as disability-adjusted life years calculated as the sum of years of life lost because of disability and years of life lived with disability. Mortality rates among children, both boys and girls, aged 10 to 14 years were obtained from these life tables.
The data, all from the year 2000, were collected from 83 countries in 6 geographic regions, as defined by the Global Burden of Disease Study (sub-Saharan Africa, Latin America and the Caribbean, Asia and Pacific Islands, China, India, and North Africa/Middle East).
Data Analysis
The data on child labor (expressed as a percentage of children aged 10 to14 years who were workers) and health indicators were analyzed by multiple regression to ascertain the effect of child labor on the various health indicators. All data were aggregated at the national level. The strength of the association between the percentage of children who were workers and HIV/AIDS infections, non-HIV infections, and malaria as expressed by disability-adjusted life years were also correlated using SPSS version 10 for Windows (SPSS Inc, Chicago, Ill).
The following were designated as dependent variables: the mortality rate among boys aged 10 to 14 years, the mortality rate among girls aged 10 to 14 years, and the percentage of the population aged 10 to 14 years undernourished.
Mortality rate among children aged 10 to 14 years is an important health indicator, commonly related to accidents. We chose mortality rate among children as a dependent variable because we could test independent variables against it to determine which independent variables most influence mortality in this age range. For each of the first 2 dependent variables, 2 separate regression models were developed, 1 using only the adult mortality rate for women and the other using only the adult male mortality rate. This avoided possible colinearity between these 2 independent variables, a problem that could have occurred had we used a combined version of the adult mortality rate. We chose prevalence of malnutrition in the population as a dependent variable because it reflects the health environment of households and we wished to determine which variables were significantly related to it.
The independent (or predictor) variables used to predict the dependent variables were the following, in various combinations: adult mortality rate for men, adult mortality rate for women, percentage of the population below the poverty line, percentage of adults infected with HIV/AIDS, percentage of the population undernourished, percentage of children aged 10 to14 years who were workers (child labor prevalence).
RESULTS
Figures 1 ▶ and 2 ▶ show the associations between the predictor variables and the dependent variables; Table 1 ▶ presents the multiple regression results. Figures 1 ▶ and 2 ▶ show that child labor appeared to be negatively correlated with the health status of the population, supporting the hypothesis that child labor affects child health.
FIGURE 1—
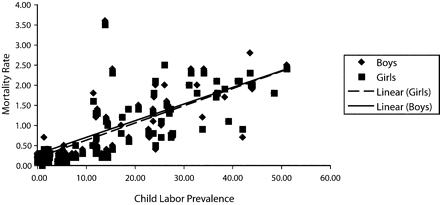
Correlation between mortality among boys and girls aged 10 to 14 years and child labor prevalence (R3 = .78).
FIGURE 2—
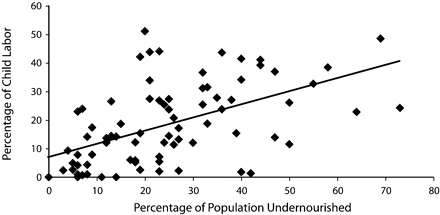
Correlation between the prevalence of child labor and the prevalence of undernourishment in the population (R3 = .47).
TABLE 1—
Multiple Regression Results (Unstandardized Coefficients) for Mortality, Undernourishment, and Labor: Children Aged 10–14 Years, 2000
| Boys | Girls | Undernourished Population | |
| Child labor prevalence | 0.016* | 0.016* | 0.003* |
| Percentage of population below national poverty lines | 0.012* | 0.015* | 0.003* |
| Adult mortality rate | |||
| Men | 0.023* | 0.023* | |
| Women | 0.017* | 0.019* | |
| Percentage of population undernourished | −0.004 | −0.006 | |
| Percentage of HIV/AIDS among adults | NA | NA | 0.01* |
Note. NA = not applicable.
*P ≤ .05.
This association could be caused by other factors affecting the population’s health status that were also correlated with the percentage of children engaged in paid labor. Therefore, we included control variables such as the percentage of the population below the poverty line and the adult mortality rate in the regression. The results of the regression confirmed that several variables played a determining role in the mortality rates of children aged 10 to 14 years and that 2 of these variables also affected the level of undernourishment. The prevalence of child labor was a significant predictor of undernourishment in a population and of the mortality rate for children aged 10 to 14 years (boys and girls), confirming that child labor affects children’s health.
We also looked at the association between childhood morbidity, as measured by disability-adjusted life years, and the prevalence of child labor in the 6 regions we studied (Figure 3 ▶). In each of the regions with a high prevalence of child labor, there was a high correlation between child labor and childhood morbidity associated with HIV/AIDS, non-HIV infectious diseases, and malaria.
FIGURE 3—
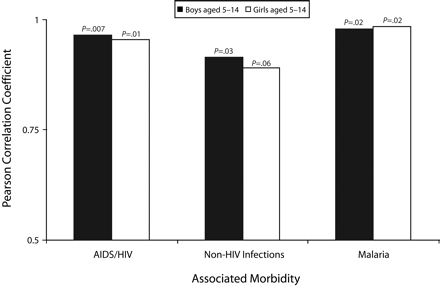
Correlation between child labor, HIV/AIDS, non-HIV infections, and malaria among children and adolescents (aged 5–14 years).
DISCUSSION
Child labor remains one of the most provocative and controversial challenges facing the world at the beginning of the 21st century. Furthermore, child labor’s close links to poverty, lack of education, poor health, and gender inequalities highlight the need for broad-based social and economic progress.
By extrapolating data from the Global Burden of Disease Study, Graitcer and Lerer estimated mortality, morbidity, and disability associated with child labor.15 Despite the limits of the Global Burden of Disease Study—for example, the health statistics were constrained by the age stratification used, and the injury data were not provided by occupation—Graitcer and Lerer were able to estimate work-related injury and mortality. They concluded that in all regions the occupational mortality rate among children matched the adult occupational mortality rate, indicating that children may be working in conditions that are as hazardous as, or even more hazardous than, those of adults. Burn injury estimates from the Global Burden of Disease Study show that work-related burns constituted more than one third of all burn injuries sustained among children aged 5 to 14 years. It is worth noting that this statistic did not take into account burns sustained during housework, the most common of which occur while cooking over an open fire.
Graitcer and Lerer did not find any health problems in working Egyptian children,16 but they argued that a child’s exposure to poor working conditions and health hazards may result in health consequences much later in life. In reports on child labor in Morocco,17 Yemen,18 and Guatemala,19 the researchers of the Understanding Children’s Work project found few or no ill health effects resulting from work and suggested that this might be because the healthiest children are selected for work or because health consequences may not become apparent until a later stage in a child’s life. They also showed that it is not work per se that is damaging to a child’s health, but rather certain kinds of work.
Studies with an ecological design have proven valuable in descriptive and etiological epidemiology, as well as in economics, social planning, and policy evaluation.30 Our study is the first to analyze the health effects of child labor with cross-sectional data, showing that some health indicators are affected by child labor.
In Table 1 ▶, the independent variables account for approximately 77% of the mortality rates for children, both boys and girls, aged 10 to 14 years. This significance (P < .001) suggests that the model is both valid and statistically significant. Child labor, poverty, and adult mortality rates explain, at a significant level, the variance in adolescent mortality among boys and girls aged 10 to 14 years. The percentage of the population that is undernourished does not explain adolescent mortality rates for either boys or girls. For each 1 of the first 2 dependent variables (adolescent mortality rates for boys and girls aged 10 to14 years), we developed 2 regression models, one taking into account only the adult mortality rate for women and the other the combined adult mortality rate for men and women. We did this to avoid any colinearity between these 2 independent variables.
The percentage of the population living below the poverty line was designated an independent variable because of its relevance to policy decisions on education, health, decentralization of resource management, and preventive measures. As predictor variables, child labor and poverty both were significantly correlated with malnutrition (as measured by the percentage of population that was undernourished), whereas the percentage of HIV/AIDS among adults was not significantly related to malnutrition.
Mortality rates for different age groups are important indicators of health status in a country. In the absence of incidence and prevalence rates for disease (morbidity data), they serve to identify vulnerable populations. They are also among the indicators most frequently used to compare levels of socioeconomic development across countries. The finding that child labor prevalence is significantly correlated with adolescent mortality, a population’s nutrition level, and the presence of infectious disease among children suggests that countries with high child labor prevalence have low health status.
Work can limit a child’s opportunities to obtain an education, especially for girls, whose educational attainment is a recognized determinant of child survival and health.31 Work can expose children to physical and social environments conducive to high-risk sexual behavior. Because child labor is significantly correlated with infectious diseases among children, including HIV/AIDS, interventions that reduce child labor rates could have a direct health benefit.
We have identified a set of health indicators affected by child labor, and our data support the hypothesis that child labor affects children’s health, particularly as measured by adolescent mortality rates. Given the nature of the available data, it is difficult to carry out a proper causality analysis. The methodological weakness of an ecological study is that estimates of effect at the ecological level cannot be extrapolated to individuals. The ecological design did not permit us to obtain direct estimates of the effect of child labor in exposed versus unexposed populations. Therefore, we could not be certain, for instance, that the children experiencing greater morbidity and mortality in a given population were actually child laborers. Other drawbacks to the ecological method are that the method relies on existing data sources, which are often flawed and may involve confounding variables for which control may be difficult.32 Problems with the ecological approach, however, are minimized when measurement, analysis, and interpretation are all at the group level and the data sources are reliable. The ecological design lends itself to the study of structural or sociological effects on human behavior and concomitant disease or injury. The principal characteristic of the ecological design—namely, that it examines differences between groups—makes it well suited to evaluating social and health policies, such as those related to injury prevention.33
Although our findings indicate that child labor may be affecting the health of children, more data are needed to develop a better understanding of the short- and long-term health problems associated with child labor. Most important, longitudinal studies are required to understand the short- and long-term health effects of child labor on the individual child.
Acknowledgments
This work was supported by the Understanding Children’s Work (Inter-Agency Research Cooperation Project), University of Rome, Italy.
Human Participant Protection No protocol approval was needed for this study.
Peer Reviewed
Contributors P. Roggero originated the study and supervised all aspects of its implementation. V. Mangiaterra assisted with the study and supervised research input. F. Bustreo contributed ideas and reviewed drafts of the article. F. Rosati synthesized analyses and interpreted findings. All authors reviewed the drafts of the article.
References
- 1.Parker D. Health effect on child labor. Lancet. 1997;350:1395–1396. [DOI] [PubMed] [Google Scholar]
- 2.UNICEF guide to the convention on the rights of the Child. Available at: http://www.unicef.org/crc/crc.htm. Accessed December 28, 2006.
- 3.International Labour Organization. ILO Convention 138: Minimum age Convention, 1973. Available at: http://www.ilo.org/public/english/standards/ipec/publ/law/ilc/c1381973. Accessed December 28, 2006.
- 4.International Labour Organization. ILO Convention 182: Worst forms of Child labor, 1999. Available at: http://www.ilo.org/public/english/standards/relm/ilc/ilc87/com-chic.htm. Accessed December 28, 2006.
- 5.US National Research Council. Committee on the Health and Safety Implications of Child Labor. Protecting Youth at Work: Health, Safety, and Development of Working Children and Adolescents in the United States. Washington, DC: National Academy Press; 1998. [PubMed]
- 6.UNICEF. The State of the World’s Children 1997. Oxford, UK: Oxford University Press, 1997.
- 7.Parker D. Child labor: the impact of economic exploitation on the health and welfare of children. Minn Med. 1997;80:10–13, 52–55. [PubMed] [Google Scholar]
- 8.Eliminating the Worst Forms of Child Labour. A Practical Guide to ILO Convention No. 182. Handbook for Parliamentarians no. 3. Geneva, Switzerland: International Labor Organization and Inter-Parliamentary Union; 2002.
- 9.International Labor Organization. Child Labor: Targeting the Intolerable. Conference Report VI (1). Geneva, Switzerland: 1998.
- 10.Forastieri V. Children at Work: Health and Safety Risks. Geneva, Switzerland: International Labor Organization; 1997.
- 11.Kebebew Ashagrie. Statistics on Working Children and Hazardous Child Labour in Brief. Rev ed. Geneva, Switzerland: International Labor Organization; 1998.
- 12.Heady C. The effect of child labor on learning achievement. World Dev. 2003;31:385–398. [Google Scholar]
- 13.Galli R. The Economic Impact of Child Labour. Geneva, Switzerland: International Labor Organization; 2001.
- 14.Harper C, Marcus R, Moore K. Enduring poverty and the conditions of childhood: life course and inter-generational poverty transmissions. World Dev 2003; 31:535–554. [Google Scholar]
- 15.Graitcer PL, Lerer LB. Child Labor and health: quantifying the global health impacts of child labors. Washington, DC: World Bank; 1998.
- 16.Graitcer PL, Lerer LB. The Impact of Child Labor on Health: Report of a Field Investigation in Egypt. Washington DC: World Bank; 2000.
- 17.Understanding children’s work in Morocco. Report prepared for the Understanding Children’s Work Project, a joint research initiative of the International Labor Organization, UNICEF, and the World Bank. 2003. Available at: http://www.ucw-project.org/pdf/publications/report_morocco_draft.pdf. Accessed December 28, 2006.
- 18.Understanding children’s work in Yemen. Report prepared for the Understanding Children’s Work Project, a joint research initiative of the International Labor Organization, UNICEF, and the World Bank. 2003. Available at: http://www.ucw-project.org/pdf/publications/report_yemen_draft.pdf. Accessed December 28, 2006.
- 19.Understanding children’s work in Guatemala. Report prepared for the Understanding Children’s Work Project, a joint research initiative of the International Labor Organization, UNICEF, and the World Bank. 2003. Available at: http://www.oit.org.pe/ipec/documentos/gua-national_report.pdf. Accessed January 5, 2006.
- 20.Susser M. The logic of the ecological: II. The logic of the design. Am J Public Health. 1994;84:830–835. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.O’Donnell O, Rosati CF, Van Doorslaer E. Child Labour and Health: Evidence and Research Issues. Florence, Italy: Innocenti Research Centre; 2002.
- 22.Shah PM. The health care of working children. Child Abuse Negl. 1984;8:541–544. [DOI] [PubMed] [Google Scholar]
- 23.Singh M, Kaura VD, Khan SA. Working Children in Bombay—A Study. New Delhi, India: National Institute of Public Cooperation and Child Development; 1980.
- 24.Gross R, Landfried B, Herman S. Height and weight as a reflection of the nutritional situation of school-aged children working and living in the street of Jakarta. Soc Sci Med. 1996;43:453–458. [DOI] [PubMed] [Google Scholar]
- 25.Ambadekar NN, Wahab SN, Zodpey SP, et al. Effect of child labor on growth of children. Public Health. 1999;113:303–306. [DOI] [PubMed] [Google Scholar]
- 26.Hawamdeh H, Spencer N. Effect of work related variables on growth among working boys in Jordan. J Epidemiol Community Health. 2003;57:154–158. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.World Bank. World Development Indicators. Washington, DC: World Bank; 2003.
- 28.Murray CJL, Lopez AD, eds. The Global Burden of Disease: A Comprehensive Assessment of Mortality and Disability From Diseases, Injuries and Risks Factors in 1990 and Projected to 2020. Cambridge, Mass: Harvard School of Public Health; 1996.
- 29.The World Health Report: Reducing Risks, Promoting Healthy Life. Geneva, Switzerland: World Health Organization; 2002.
- 30.Lopez AD, Salomon J, Ahmad O, Murray CJL. Life Tables for 191 Countries: Data, Methods and Results. Global Program on Evidence discussion no. 9. Geneva, Switzerland: World Health Organization; 2000.
- 31.Raju T. Child labor, adult illiteracy and employment rates in India. Indian J Pediatr. 1989;56:193–200. [DOI] [PubMed] [Google Scholar]
- 32.Walter SD. The ecologic method in the study of environmental health. I. Overview of the method. Environ Health Perspect 1991;94:61–5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Rothman KJ. Methodologic frontiers in environmental epidemiology. Environ Health Perspect Suppl. 1993;101(suppl 4):19–21. [DOI] [PMC free article] [PubMed] [Google Scholar]