

Abstract
Fire-eater's pneumonia is an acute, intense hydrocarbon pneumonitis resulting from aspiration of volatile hydrocarbons such as kerosene, gasoline, or turpentine. The vast majority of patients have resolution of their acute lung injury with supportive care only, avoiding the need for surgical lung reduction procedures. We describe a case of severe hydrocarbon pneumonitis secondary to aspiration of JP-8 jet fuel. The presentation, management, and prognosis of fire-eater's pneumonia are reviewed.
Readers are encouraged to respond to George Lundberg, MD, Editor of MedGenMed, for the editor's eye only or for possible publication via email: glundberg@medscape.net
Introduction
Fire-eater's pneumonia is an acute, intense hydrocarbon pneumonitis resulting from aspiration of volatile hydrocarbons such as kerosene, gasoline, or turpentine. Forty percent to 50% of cases are seen in children younger than 6 years old resulting from unintentional aspiration. The remaining cases are mostly occupational exposures, such as fire-eaters, petrochemical workers, painters, and hazardous waste workers.[1] While the long-term prognosis is uncertain, the vast majority of patients have resolution of their acute lung injury with supportive care only, avoiding the need for surgical lung reduction procedures. We describe a case of severe hydrocarbon pneumonitis as the result of aspiration of JP-8 jet fuel, a kerosene-based compound and the accompanying radiographic changes seen at presentation and following treatment.
Case
A 19-year-old Army corporal was admitted after accidentally aspirating JP-8 jet fuel during siphoning. His pulmonary status rapidly deteriorated requiring intubation with the development of massive necrotic abscesses with air-fluid levels (Figure 1, asterisks) in his right lung. Two thoracotomy tubes were inserted (Figure 1, arrow). He continued to be febrile despite the use of broad-spectrum antibiotics but gradually improved after their discontinuation and was extubated. A bronchoscopy was performed that revealed inflamed, hyperemic mucosa without purulence or evidence of necrosis. Repeat computed tomography scan 3 days before discharge showed remarkable improvement (Figure 2). No surgical interventions were required.
Figure 1.
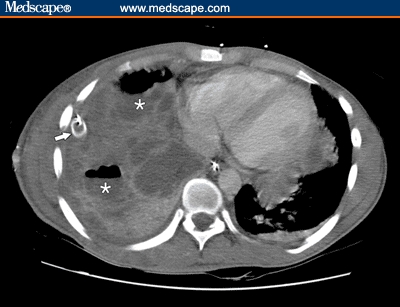
CT of chest with IV contrast shows extensive involvement of right lung parenchyma with thoracotomy tube visible (arrow), abscesses with air-fluid levels (asterisks), and a right-sided loculated pleural effusion.
Figure 2.
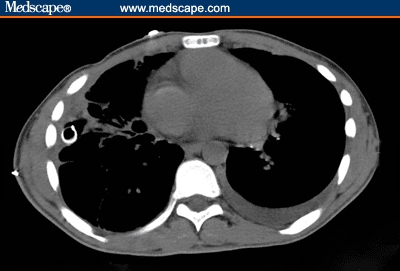
Repeat noncontrast-enhanced CT of the chest done 3 weeks later reveals marked improvement in the right lung with minimal residual scarring.
Discussion
The current case highlights the clinical presentation and course of patients in whom fire-eater's pneumonia develops. Aspiration of volatile hydrocarbons or “fire-eater's pneumonia” is a dramatic hydrocarbon pneumonitis occasionally seen in children and fire-eating performers. The petroleum derivative kerdane, a low viscosity and surface tension substance composed of toluene, xylene, ethylbenzene, propylbenzene, and methylbenzene, is frequently used by fire-eating performers and has been implicated in the majority of such cases.[2] The use of paraffin, or octane, has also been observed.[3] Serious toxicity from hydrocarbon compounds with high viscosity and surface tension such as mineral oil and petrolatum is less likely[1]; however, these compounds have been implicated in exogenous lipoid pneumonia, a chronic lower respiratory tract illness with histologic findings similar to those of fire-eater's pneumonia.[4] Aviation jet fuel and other commercial hydrocarbons such as kerosene, turpentine, and gasoline are composed of a mixture of several varieties of hydrocarbons, most of which are members of the paraffin, naphthene, or aromatic classes. The different types of jet fuels are determined by the varying proportions of compounds from these 3 classes.[5] JP-8 jet fuel, a kerosene-based compound, possesses relatively low viscosity and has the ability to rapidly diffuse throughout the bronchial tree and disrupt the surfactant barrier, causing an inflamed, hyperemic, nonpurulent reaction similar to that observed in our patient. Microscopic features that are similar to lipoid pneumonia include lipid-filled macrophages as the predominant cell type with a paucity of microorganisms.[6]
Despite fever and serum markers of infection, fire-eater's pneumonia is generally a pseudo-infectious lung disease with an intense inflammatory cytokine release. Antibiotics are rarely needed in the treatment of these patients as was found in our patient. The use of corticosteroids remains controversial. Some studies suggest that steroids may improve outcomes in severely affected individuals, yet these data are only based on a limited number of patients.[2,7] The use of gastric decontamination to prevent subsequent pulmonary injury from hydrocarbon ingestion is controversial. It may have potential benefit in large (> 30 cc), intentional ingestion of compounds with systemic toxicity.[1]
While long-term prognosis is uncertain, one study[2] documented normal radiographic features and pulmonary function tests 6 months after the initial injury. As is typical of fire-eater's pneumonia and was demonstrated in our patient, conservative supportive care is frequently a successful strategy of treatment.
The opinions or assertions contained herein are those of the authors and should not be construed as reflecting the views of the Department of the Army or the Department of Defense.
Contributor Information
Matthew Aboudara, Walter Reed Army Medical Center, Washington, DC. Email: Matthew.Aboudara@na.amedd.army.mil.
Joon Yun, Walter Reed Army Medical Center, Washington, DC. Email: jsyun@bethesda.med.navy.mil.
References
- 1.Godfrank, Flomaenbaum, Lewin, et al. Goldfrank's Toxicologic Emergencies. 7th ed. New York: McGraw-Hill; 2002. pp. 1303–1323. [Google Scholar]
- 2.Gentina T, Tillie-Leblond I, Birolleau S, et al. Fire-eater's lung: seventeen cases and a review of the literature. Medicine. 2001;80:291–297. doi: 10.1097/00005792-200109000-00002. [DOI] [PubMed] [Google Scholar]
- 3.Beermann B, Christensson T, Moller P, Stillstrom A. Lipoid pneumonia: an occupational hazard of fire eaters. BMJ. 1984;289:1728–1729. doi: 10.1136/bmj.289.6460.1728. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Crapo J, Glassroth J, Karlinsky J, et al. Baum's Textbook of Pulmonary Diseases. 7th ed. Baltimore: Lippincott Williams and Wilkins; 2004. pp. 412–413. [Google Scholar]
- 5.Chevron USA. Inc. Aviation Turbine Fuel Composition. Aviation Fuels Technical Review. Chapter 4. Available at: http://www.chevron.com/products/prodserv/fuels/bulletin/aviationfuel/4_at_fuel_comp.shtm. Accessed April 26, 2006.
- 6.Burkhardt O, Merker H-J, Shakibaei M, et al. Electron microscopic findings in BAL of a fire-eater after petroleum aspiration. Chest. 2003;124:398–400. doi: 10.1378/chest.124.1.398. [DOI] [PubMed] [Google Scholar]
- 7.Segev D, Szold O, Fireman E, et al. Kerosene-induced severe acute respiratory failure in near drowning: reports on four cases of the literature. Crit Care Med. 1999;27:1437–1440. doi: 10.1097/00003246-199908000-00004. [DOI] [PubMed] [Google Scholar]