

Abstract
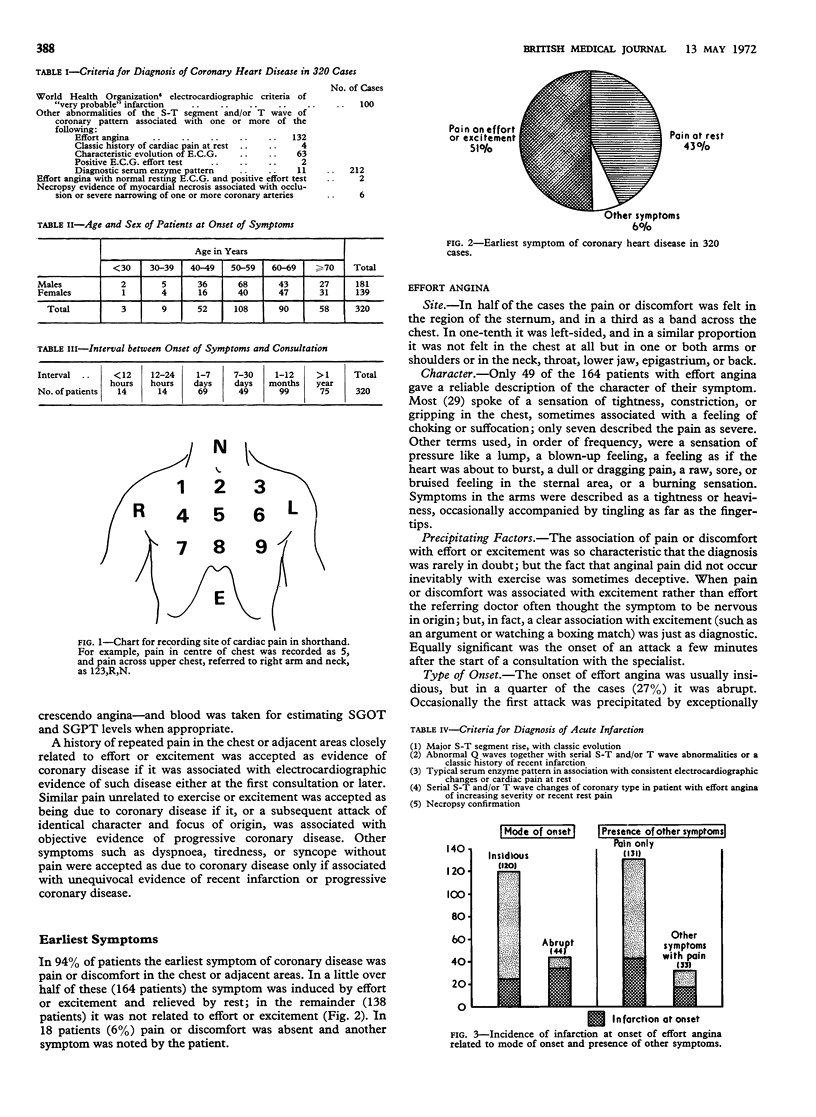
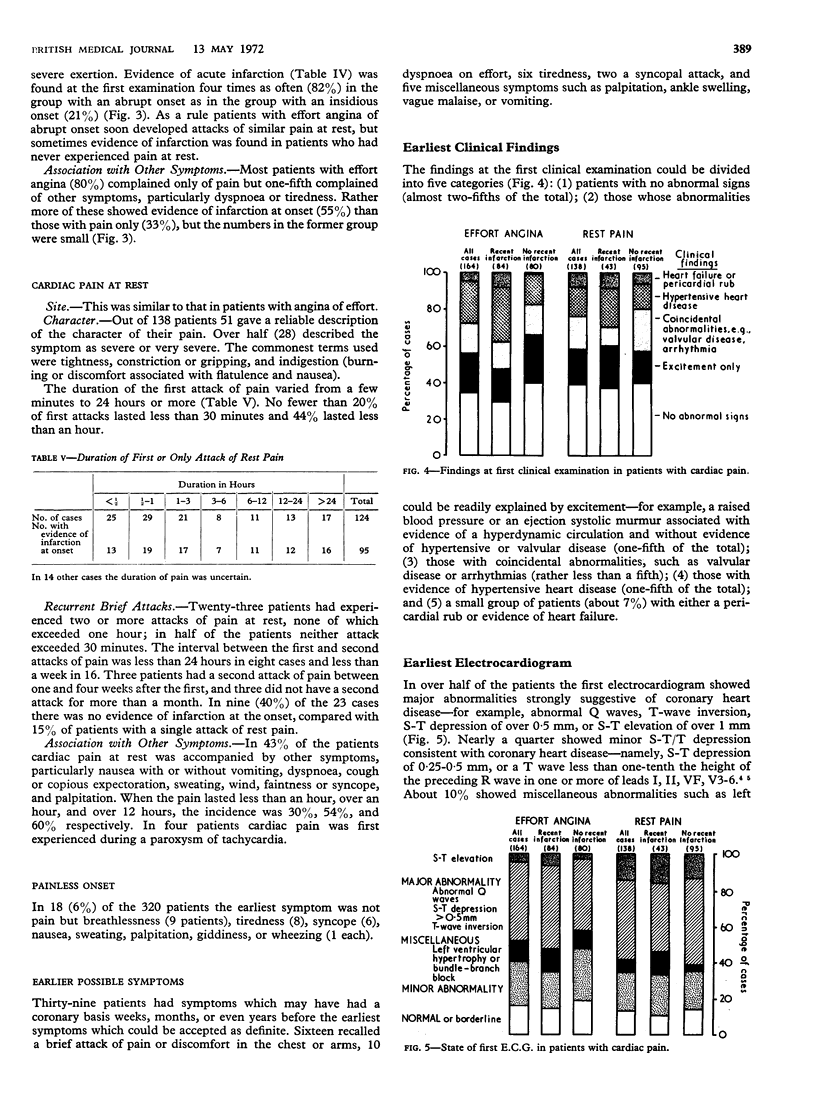
We have reviewed the histories of 320 patients in whom a diagnosis of coronary heart disease was ultimately established and traced the symptoms back to their first appearance. In 51% the first symptom was effort angina. Difficulties in recognition arose when the symptom was localized to an unusual site, when its occurrence was dependent on a combination of exercise with cold or a recent meal, or when it was induced by excitement rather than by effort. In a quarter of the cases the onset of angina was abrupt, and in these there was usually evidence of acute infarction.
In 43% of cases the first symptom was an attack of pain or discomfort in the torso occurring without any discernable precipitating factor. Again, diagnosis was difficult when the pain was in an atypical site and also when it was of brief duration associated with skeletal or abdominal disease which could cause pain at the same site, or if the patient was able to undertake strenuous exertion. In four patients cardiac pain was first experienced during a paroxysm of tachycardia. In 6% of cases the onset was marked by a symptom other than pain—most frequently dyspnoea, tiredness, faintness, or syncope.
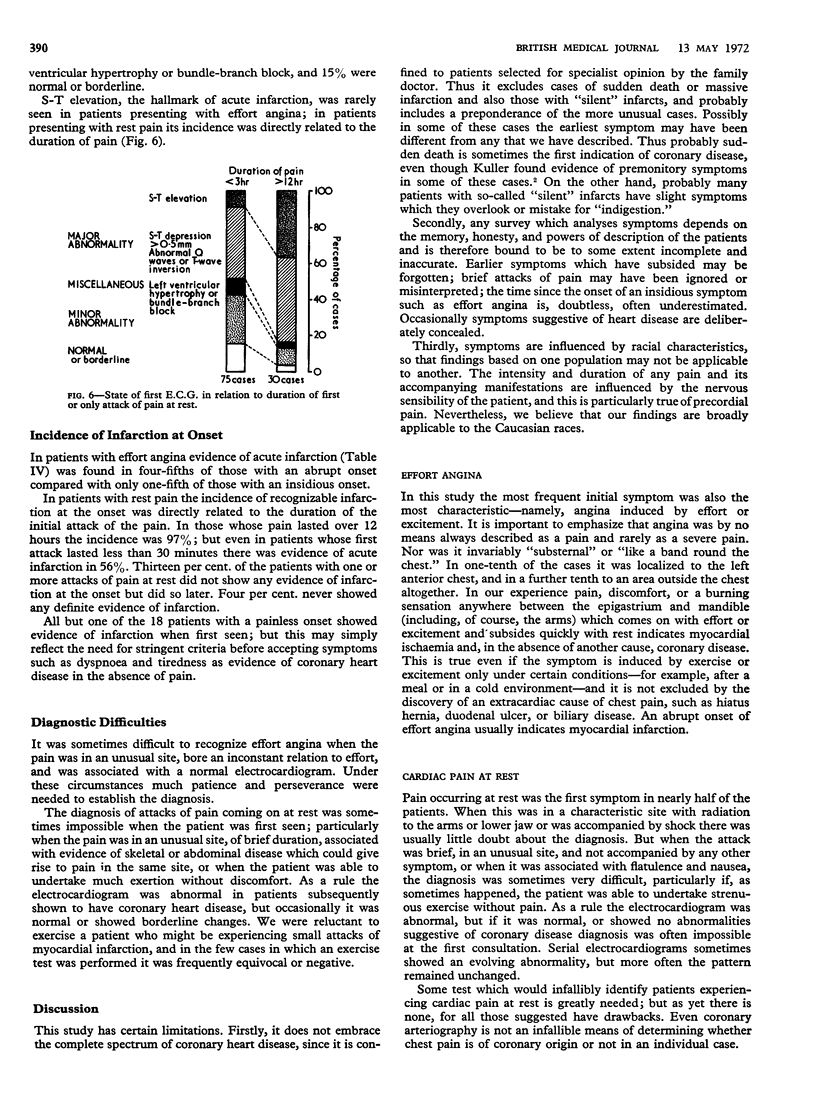
Clinical examination was of no direct value in diagnosis. Its importance lay in disclosing factors which had to be taken into account in interpreting the electrocardiogram. The electrocardiogram was invaluable, though by no means infallible. In over half of the patients the first tracing showed major abnormalities of coronary type, and nearly a quarter more showed minor S-T/T depression consistent with coronary disease. Ten per cent. showed miscellaneous abnormalities, such as left ventricular hypertrophy or bundle-branch block, and 15% no definite abnormality.
There is as yet no completely reliable objective method of diagnosing early coronary heart disease, so that the recognition of symptoms remains of paramount importance.
Full text
PDF
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Kuller L. Sudden death in arteriosclerotic heart disease; the case for preventive medicine. Am J Cardiol. 1969 Nov;24(5):617–628. doi: 10.1016/0002-9149(69)90450-0. [DOI] [PubMed] [Google Scholar]
- Short D. Clinical significance of minor ST-T depression in resting electrocardiogram. Br Heart J. 1972 Apr;34(4):377–382. doi: 10.1136/hrt.34.4.377. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Solomon H. A., Edwards A. L., Killip T. Prodromatan acute myocardial infarction. Circulation. 1969 Oct;40(4):463–471. doi: 10.1161/01.cir.40.4.463. [DOI] [PubMed] [Google Scholar]
- Stowers M., Short D. Warning symptoms before major myocardial infarction. Br Heart J. 1970 Nov;32(6):833–838. doi: 10.1136/hrt.32.6.833. [DOI] [PMC free article] [PubMed] [Google Scholar]