

Abstract
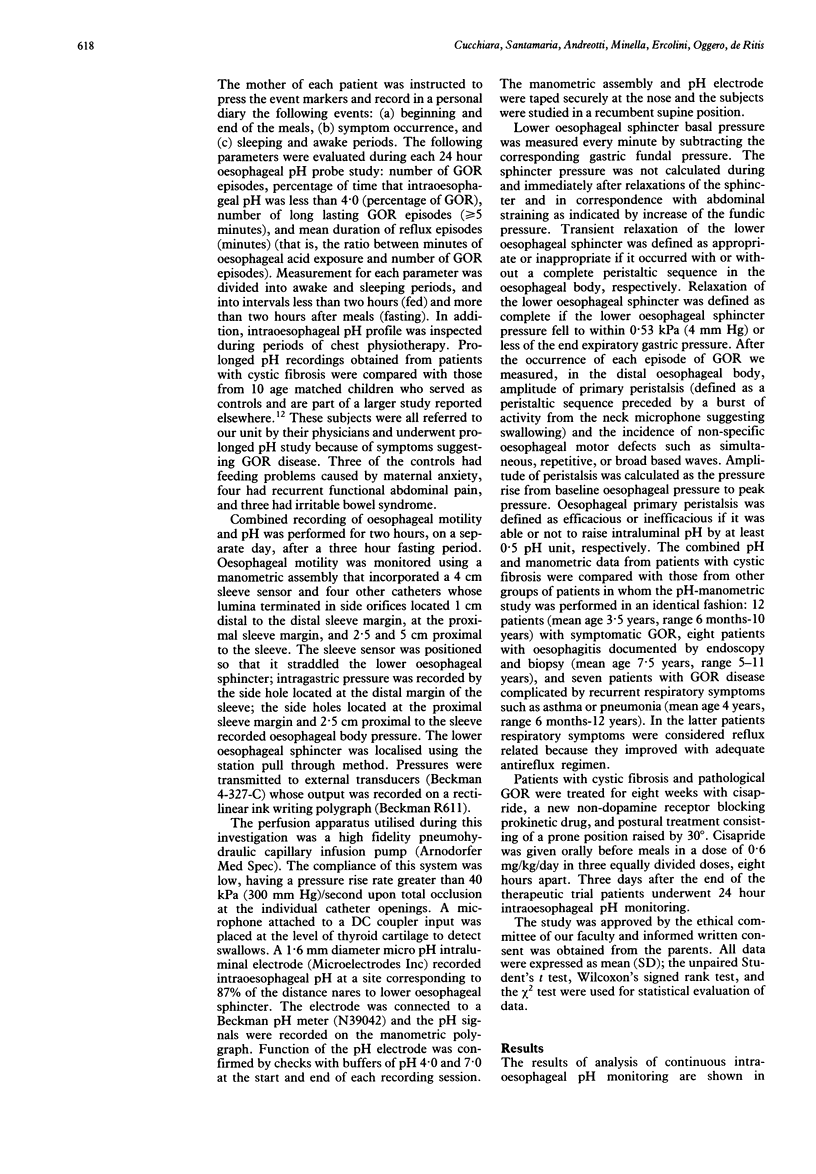
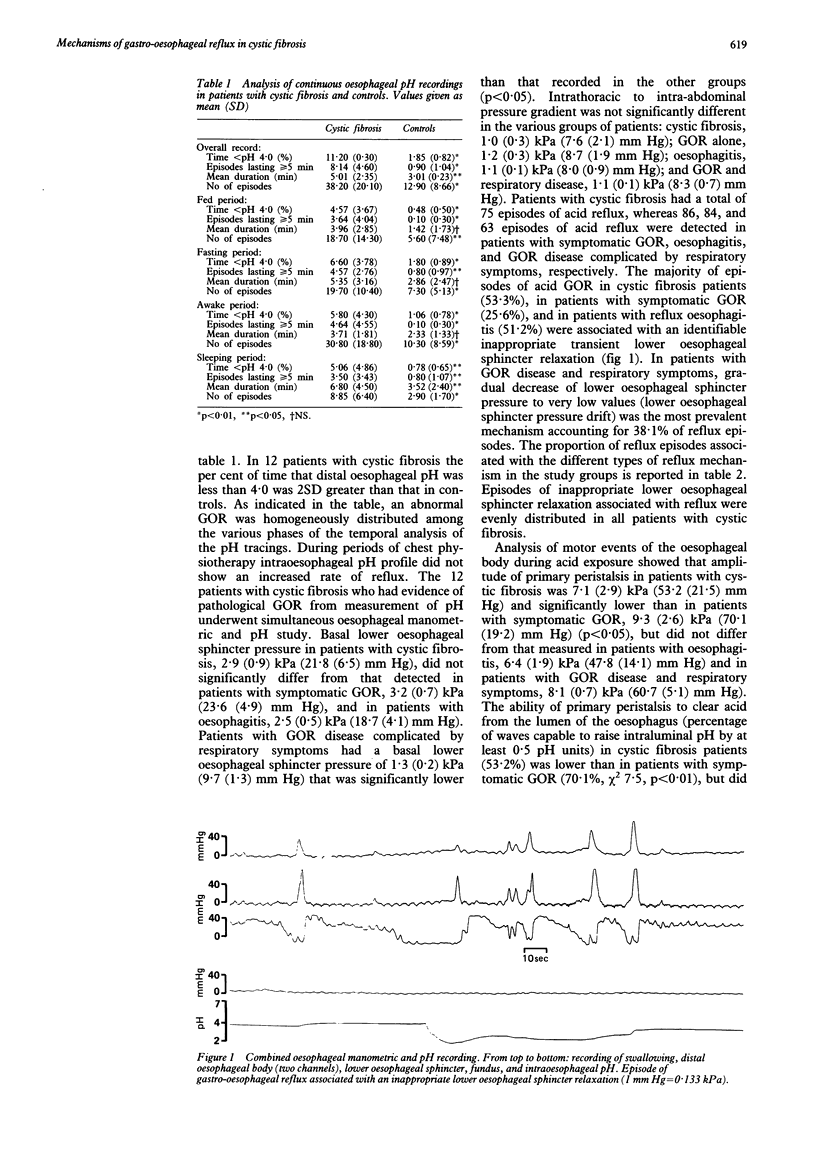
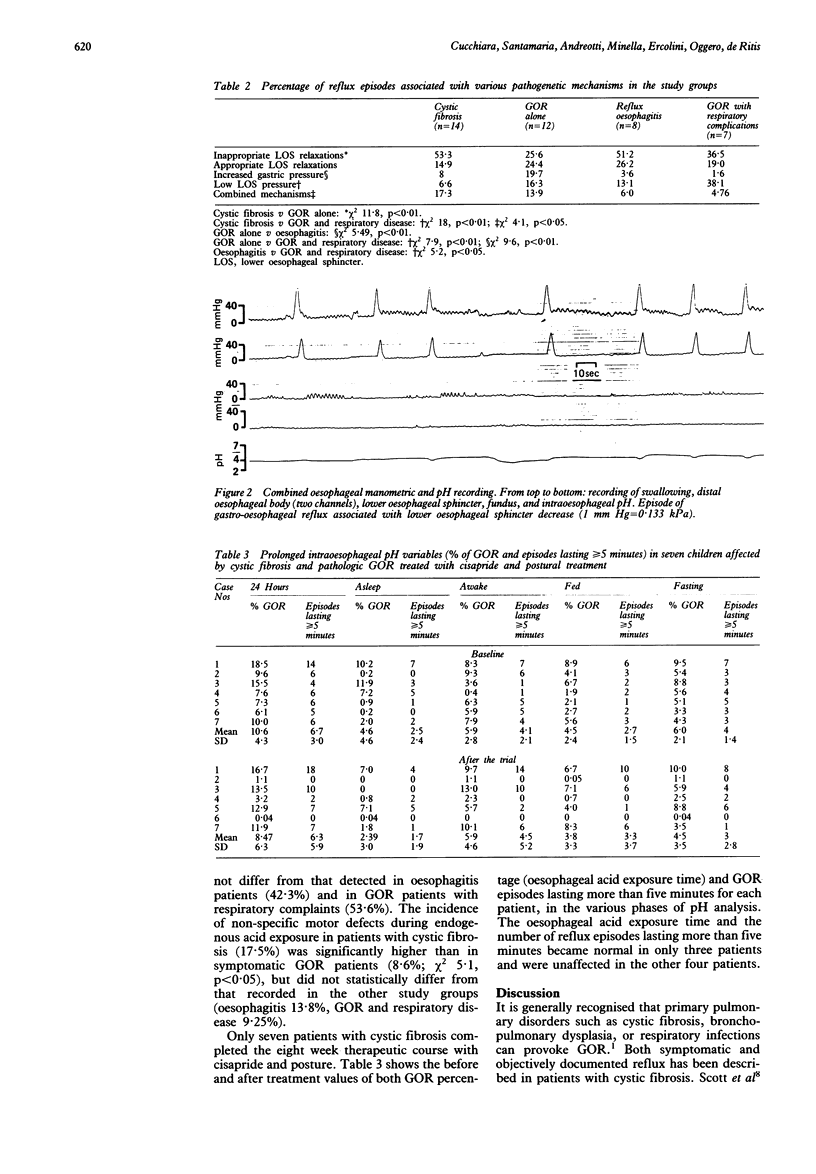
Abnormal degrees of gastro-oesophageal reflux (GOR) were detected by 24 hour intraoesophageal pH measurement in 12 of 14 children (mean age 7.9 years; range 5 months-16 years) affected by cystic fibrosis and complaining of symptoms suggesting GOR. These patients underwent combined recording of distal oesophageal motility and intraluminal pH in order to investigate mechanisms of GOR. Inappropriate lower oesophageal sphincter relaxation was the most common mechanism of reflux in all patients. Other mechanisms (appropriate relaxation or lowered pressure of the lower oesophageal sphincter, increased intragastric pressure) were detected less frequently. Frequency of inappropriate lower oesophageal sphincter relaxations was significantly higher in patients with cystic fibrosis than in other study groups (symptomatic GOR, GOR disease complicated by respiratory complaints). Inappropriate lower oesophageal sphincter relaxations occurred with the same frequency in patients with cystic fibrosis and in a group of children with GOR disease complicated by oesophagitis. Abnormalities of distal oesophageal contractions such as decreased amplitude or uncoordinated waves were also recorded in cystic fibrosis patients. Seven patients with cystic fibrosis completed a therapeutic trial for eight weeks consisting of postural treatment and oral cisapride, a new prokinetic drug. The oesophageal acid exposure improved in only three patients. We conclude that pathologic GOR is commonly associated with cystic fibrosis. The predominant reflux mechanism in these patients is a transient inappropriate lower oesophageal sphincter relaxation rather than a low steady state basal lower oesophageal sphincter pressure.
Full text
PDF

Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Allen C. J., Newhouse M. T. Gastroesophageal reflux and chronic respiratory disease. Am Rev Respir Dis. 1984 Apr;129(4):645–647. [PubMed] [Google Scholar]
- Barish C. F., Wu W. C., Castell D. O. Respiratory complications of gastroesophageal reflux. Arch Intern Med. 1985 Oct;145(10):1882–1888. [PubMed] [Google Scholar]
- Bendig D. W., Seilheimer D. K., Wagner M. L., Ferry G. D., Barrison G. M. Complications of gastroesophageal reflux in patients with cystic fibrosis. J Pediatr. 1982 Apr;100(4):536–540. doi: 10.1016/s0022-3476(82)80748-8. [DOI] [PubMed] [Google Scholar]
- Boyle J. T., Altschuler S. M., Nixon T. E., Tuchman D. N., Pack A. I., Cohen S. Role of the diaphragm in the genesis of lower esophageal sphincter pressure in the cat. Gastroenterology. 1985 Mar;88(3):723–730. doi: 10.1016/0016-5085(85)90143-x. [DOI] [PubMed] [Google Scholar]
- Boyle J. T. Gastroesophageal reflux in the pediatric patient. Gastroenterol Clin North Am. 1989 Jun;18(2):315–337. [PubMed] [Google Scholar]
- Chrispin A. R., Norman A. P. The systematic evaluation of the chest radiograph in cystic fibrosis. Pediatr Radiol. 1974;2(2):101–105. doi: 10.1007/BF01314939. [DOI] [PubMed] [Google Scholar]
- Cucchiara S., Staiano A., Gobio Casali L., Boccieri A., Paone F. M. Value of the 24 hour intraoesophageal pH monitoring in children. Gut. 1990 Feb;31(2):129–133. doi: 10.1136/gut.31.2.129. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dent J., Dodds W. J., Hogan W. J., Toouli J. Factors that influence induction of gastroesophageal reflux in normal human subjects. Dig Dis Sci. 1988 Mar;33(3):270–275. doi: 10.1007/BF01535748. [DOI] [PubMed] [Google Scholar]
- Dent J., Holloway R. H., Toouli J., Dodds W. J. Mechanisms of lower oesophageal sphincter incompetence in patients with symptomatic gastrooesophageal reflux. Gut. 1988 Aug;29(8):1020–1028. doi: 10.1136/gut.29.8.1020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gerhardt T., McCarthy J., Bancalari E. Effects of aminophylline on respiratory center and reflex activity in premature infants with apnea. Pediatr Res. 1983 Mar;17(3):188–191. doi: 10.1203/00006450-198303000-00003. [DOI] [PubMed] [Google Scholar]
- Mittal R. K., McCallum R. W. Characteristics and frequency of transient relaxations of the lower esophageal sphincter in patients with reflux esophagitis. Gastroenterology. 1988 Sep;95(3):593–599. doi: 10.1016/s0016-5085(88)80003-9. [DOI] [PubMed] [Google Scholar]
- Nelson H. S. Gastroesophageal reflux and pulmonary disease. J Allergy Clin Immunol. 1984 May;73(5 Pt 1):547–556. doi: 10.1016/0091-6749(84)90509-8. [DOI] [PubMed] [Google Scholar]
- Orenstein S. R., Orenstein D. M. Gastroesophageal reflux and respiratory disease in children. J Pediatr. 1988 Jun;112(6):847–858. doi: 10.1016/s0022-3476(88)80204-x. [DOI] [PubMed] [Google Scholar]
- Reynolds J. C. Prokinetic agents: a key in the future of gastroenterology. Gastroenterol Clin North Am. 1989 Jun;18(2):437–457. [PubMed] [Google Scholar]
- Scott R. B., O'Loughlin E. V., Gall D. G. Gastroesophageal reflux in patients with cystic fibrosis. J Pediatr. 1985 Feb;106(2):223–227. doi: 10.1016/s0022-3476(85)80291-2. [DOI] [PubMed] [Google Scholar]
- Vinocur C. D., Marmon L., Schidlow D. V., Weintraub W. H. Gastroesophageal reflux in the infant with cystic fibrosis. Am J Surg. 1985 Jan;149(1):182–186. doi: 10.1016/s0002-9610(85)80030-1. [DOI] [PubMed] [Google Scholar]