

Abstract
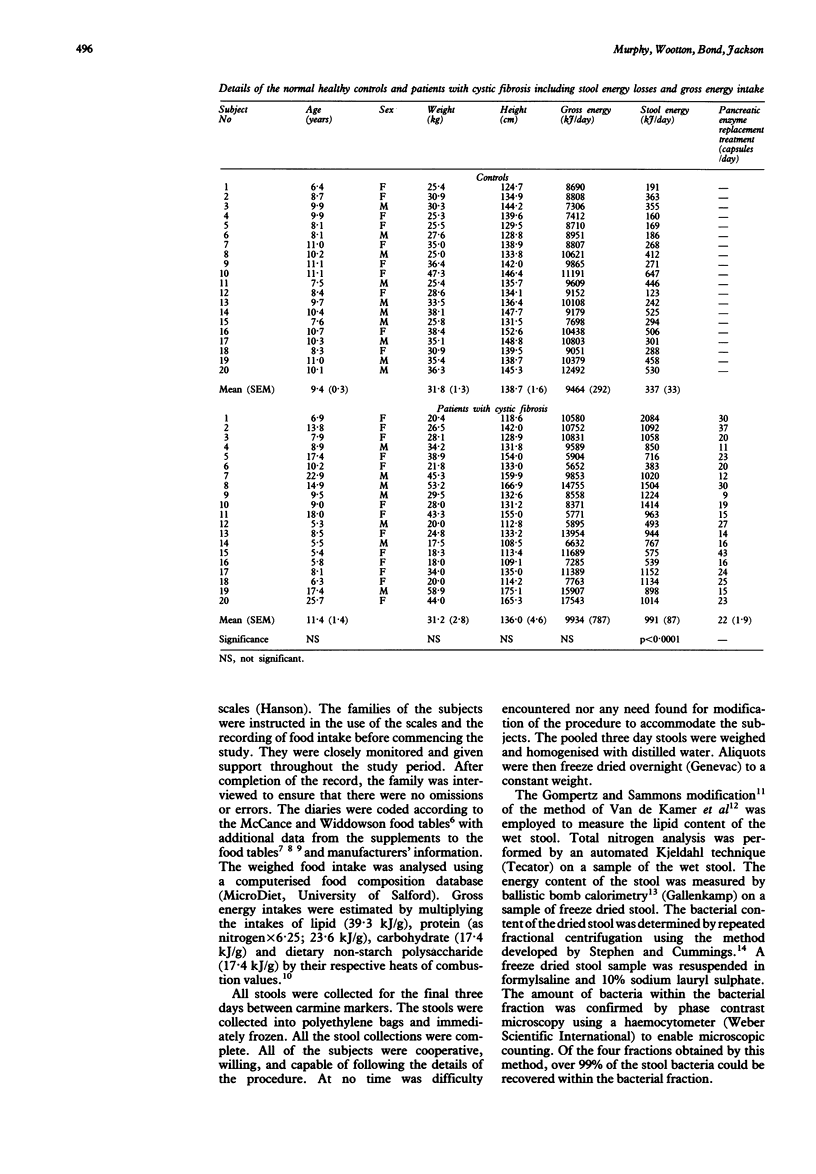
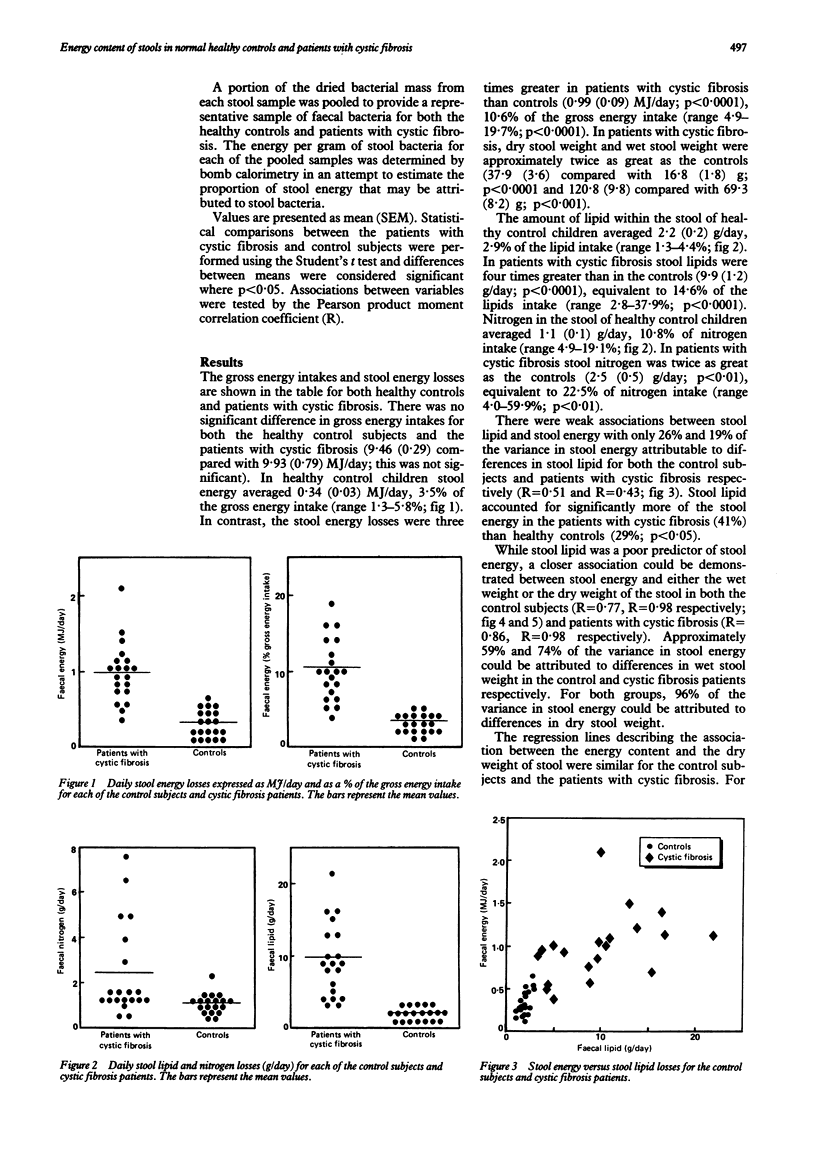
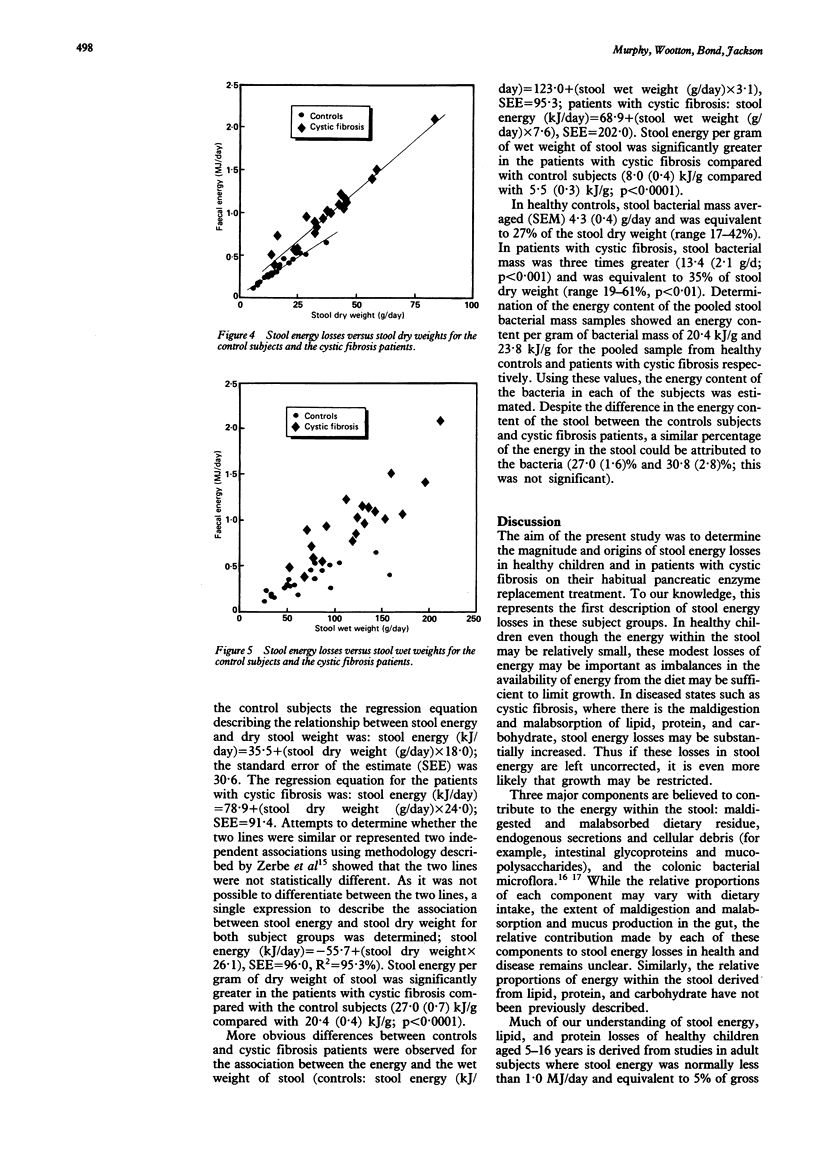
Stool energy losses and the sources of energy within the stool were determined in 20 healthy controls and 20 patients with cystic fibrosis while on their habitual pancreatic enzyme replacement treatment. Stool energy losses were equivalent to 3.5% of gross energy intake in healthy children (range 1.3-5.8%). Despite a comparable gross energy intake, stool energy losses were three times greater in patients with cystic fibrosis than controls averaging 10.6% of gross energy intake (range 4.9-19.7%). Stool lipid could account for only 29% and 41% of the energy within the stool in controls and patients with cystic fibrosis respectively and was poorly related to stool energy. Approximately 30% of the energy within the stool could be attributable to colonic bacteria in both the healthy children and patients with cystic fibrosis. These results suggest that stool energy losses in healthy children are relatively modest but that even when patients with cystic fibrosis are symptomatically well controlled on pancreatic enzyme replacement, raised stool energy losses may continue to contribute towards an energy deficit sufficient to limit growth in cystic fibrosis. As the energy content per gram wet weight remains relatively constant (8 kJ/g), stool energy losses may be estimated from simple measurements of stool wet weight.
Full text
PDF
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Beverley D. W., Kelleher J., MacDonald A., Littlewood J. M., Robinson T., Walters M. P. Comparison of four pancreatic extracts in cystic fibrosis. Arch Dis Child. 1987 Jun;62(6):564–568. doi: 10.1136/adc.62.6.564. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cummings J. H. Constipation, dietary fibre and the control of large bowel function. Postgrad Med J. 1984 Nov;60(709):811–819. doi: 10.1136/pgmj.60.709.811. [DOI] [PMC free article] [PubMed] [Google Scholar]
- GOMPERTZ S. M., SAMMONS H. G. THE ORIGIN OF FAECAL LIPIDS. THE COMPOSITION OF FAECAL FATSIN HUMAN SUBJECTS. Clin Chim Acta. 1963 Jul;8:591–603. doi: 10.1016/0009-8981(63)90110-4. [DOI] [PubMed] [Google Scholar]
- MILLER D. S., PAYNE P. R. A ballistic bomb calorimeter. Br J Nutr. 1959;13:501–508. doi: 10.1079/bjn19590064. [DOI] [PubMed] [Google Scholar]
- Marr J. W. Individual dietary surveys: purposes and methods. World Rev Nutr Diet. 1971;13:105–164. doi: 10.1159/000391884. [DOI] [PubMed] [Google Scholar]
- Mischler E. H., Parrell S., Farrell P. M., Odell G. B. Comparison of effectiveness of pancreatic enzyme preparations in cystic fibrosis. Am J Dis Child. 1982 Dec;136(12):1060–1063. doi: 10.1001/archpedi.1982.03970480026006. [DOI] [PubMed] [Google Scholar]
- Shmerling D. H., Forrer J. C., Prader A. Fecal fat and nitrogen in healthy children and in children with malabsorption or maldigestion. Pediatrics. 1970 Nov;46(5):690–695. [PubMed] [Google Scholar]
- Southgate D. A., Durnin J. V. Calorie conversion factors. An experimental reassessment of the factors used in the calculation of the energy value of human diets. Br J Nutr. 1970 Jun;24(2):517–535. doi: 10.1079/bjn19700050. [DOI] [PubMed] [Google Scholar]
- Stead R. J., Skypala I., Hodson M. E., Batten J. C. Enteric coated microspheres of pancreatin in the treatment of cystic fibrosis: comparison with a standard enteric coated preparation. Thorax. 1987 Jul;42(7):533–537. doi: 10.1136/thx.42.7.533. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stephen A. M., Cummings J. H. The microbial contribution to human faecal mass. J Med Microbiol. 1980 Feb;13(1):45–56. doi: 10.1099/00222615-13-1-45. [DOI] [PubMed] [Google Scholar]
- Zerbe G. O., Archer P. G., Banchero N., Lechner A. J. On comparing regression lines with unequal slopes. Am J Physiol. 1982 Mar;242(3):R178–R180. doi: 10.1152/ajpregu.1982.242.3.R178. [DOI] [PubMed] [Google Scholar]