

Abstract
Objectives
To explore the illicit use of specific prescription stimulants among college students and add to our understanding of reasons (motives) and routes of administration associated with illicit use of these drugs.
Methods
A random sample of 4580 college students self-administered a Web-based survey. The survey contained a variety of items pertaining to the illicit use of prescription stimulants. An extensive list of prescription stimulants was provided, and students were asked to select all the specific prescription stimulants that they had used illicitly. Items were also included to assess the motives and routes of administration associated with illicit use of prescription stimulants.
Results
Lifetime and past-year prevalence rates for illicit use of prescription stimulants were 8.3% (382 students) and 5.9% (269 students), respectively. Approximately three fourths (75.8%) of the 269 past-year illicit users of prescription stimulants reported using an amphetamine-dextroamphetamine combination agent (e.g., Adderall) in the past year, and approximately one fourth (24.5%) reported using methylphenidate (e.g., Ritalin, Concerta, Metadate, Methylin). Past-year illicit use of prescription stimulants was more than 3 times more likely among Caucasians (odds ratio [OR] 3.1, 95% confidence interval [CI] 1.5–6.6) and Hispanics (OR 3.8, 95% CI 1.6–9.3) compared with African-Americans, and more than twice as likely among Caucasians (OR 2.1, 95% CI 1.3–3.4) and Hispanics (OR 2.6, 95% CI 1.4–5.1) compared with Asians. The most commonly reported motives for illicit use were to help with concentration (65.2%), help study (59.8%), and increase alertness (47.5%). Other motives included getting high (31.0%) and experimentation (29.9%). Nearly every illicit user (95.3%) reported oral administration, and 38.1% reported snorting prescription stimulants.
Conclusion
Illicit use of amphetamine-dextroamphetamine is more prevalent than illicit use of methylphenidate formulations among college students.
Keywords: prescription stimulants, illicit use, college students, motives, amphetamines, methylphenidate, route of administration
The illicit use of prescription stimulants by college students has been well documented over the past 5 years.1–5 However, with the exception of methylphenidate formulations, of which Ritalin (Novartis Pharmaceuticals Corp., East Hanover, NJ) has received the most attention in medical literature, little information is available regarding which specific stimulants are used illicitly by college students. We know of only two college-based studies2, 6 that have examined the illicit use of selected prescription stimulants other than methylphenidate. The first study, which used a convenience sample of 150 undergraduate college students, found slightly higher rates of illicit use for methylphenidate only (7.3%) compared with amphetamine-dextroamphetamine only (Adderall; Shire US Inc., Newport, KY) (4.0%).2 Most notably, it was found that using both methylphenidate and Adderall was the most prevalent form of illicit use of prescription stimulants (24.0%). The second study used 26 “purposefully selected” students who were familiar with drug use.6 According to these students’ perceptions, Adderall was used more than other prescription stimulants on their campus due to its availability and lower occurrence of “ups and downs.” Students in this sample were not representative of the entire student body, and self-reported prevalence rates were not provided. To our knowledge, these studies, although limited in their design, are the only published college-based investigations that have specifically examined illicit use of amphetamine-dextroamphetamine combination products.
Limited data exist regarding which specific prescription stimulants are used illicitly among students in other age groups. For example, a 2004 study reported the following past-year prevalence rates of illicit amphetamine use among high school seniors: 2.3% Ritalin, 1.9% methamphetamine, 0.7% Dexedrine, 0.2% Benzedrine, 0.2% Methedrine, 0.1% Preludin, and 0.1% Dexamyl.7 As with studies of the general population,8 that study did not assess illicit use of amphetamine-dextroamphetamine formulations. Because these formulations are among the most commonly prescribed stimulants for treatment of attention-deficit–hyperactivity disorder (ADHD), it is crucial to determine the extent of their illicit use.
Data are also scarce with regard to the prevalence of illicit use of specific prescription stimulants in both high school and college students. In addition, comprehensive surveys of motives for illicit stimulant drug use are needed, particularly in light of a growing body of evidence indicating several possible motives for illicit use of prescription stimulants. In one study, the primary reasons students provided for illicitly using prescription stimulants were to help concentrate, increase alertness, and get high.9 Of note, many students also wrote in “to study” as a motive that was not provided as a fixed item in the survey; this motive needs to be empirically tested. Finally, at least one other study that we are aware of has assessed routes other than oral administration for stimulant drugs among college students.1 According to that study, almost 13% of 283 students sampled had used methylphenidate intranasally.
Development of clinical, prevention, policy, and educational strategies for reducing prescription stimulant abuse requires knowledge of which agents are being abused and insight into motives for drug use and the routes by which these agents are being administered. We sought to address these gaps in knowledge by assessing the prevalence of illicit use of specific prescription stimulants within a large, randomly selected sample of undergraduate college students. We also examined students’ reasons for illicit use of prescription stimulants, using a comprehensive list of motives that evolved from earlier research,9 and explored the routes of illicit drug administration.
Methods
Design
This study was approved by the institutional ethical review board at a large midwestern university and was conducted at that university during a 2-month period in January and February of 2005. A random sample of 5389 full-time undergraduate students was drawn from the total undergraduate population of 20,138 full-time students (10,339 women, 9799 men). In addition, we oversampled 652 Hispanic, 634 African-American, and 244 Asian undergraduate students in order to produce reliable prevalence estimates for these racial and ethnic groups. The entire sample was mailed a prenotification letter with $2 enclosed. This letter described the study and invited students to self-administer a confidential Web survey by using a URL address and a unique password. Nonrespondents were sent up to three reminder e-mails. The survey was maintained on an Internet site with the secure socket layer protocol to ensure privacy and security. By participating in the survey, students became eligible for a sweepstakes that included cash prizes, travel vouchers, field passes to athletic events, and iPods. The final response rate was 66%, which exceeded the average response rate for national college-based studies of alcohol and other drugs.10 Similar Web-based study designs and procedures are described in more detail elsewhere.11
Sample
The final sample consisted of 4580 undergraduate students and closely resembled the demographic characteristics of the overall student population. Fifty percent were women. The sample consisted of 65% Caucasians, 13% Asians, 7% African-Americans, 4% Hispanics, and 11% Native-Americans and other racial categories. The mean ± SD age of students in the sample was 20 ± 2.0 years.
Measures
As shown in Figure 1, computerized skip logic was used to guide students through survey questions pertaining to illicit use of prescription stimulants. Students received follow-up questions only if they acknowledged having illicitly used prescription stimulants during their lifetime. Survey questions about motives for illicit use of prescription stimulants were based on our earlier work9 and were not mutually exclusive (i.e., students could report more than one reason). It should be noted that our survey items included both generic and brand names in order to increase clarity for respondents. However, we use generic names exclusively in our description of our findings.
Figure 1.
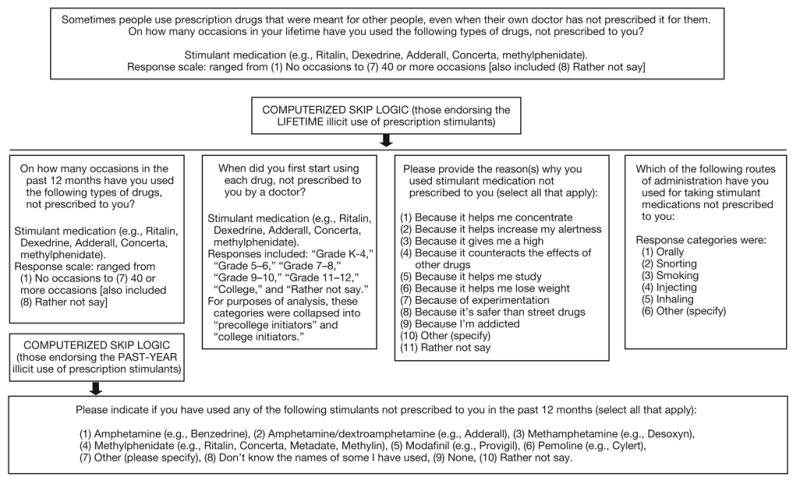
Flow diagram representation of measures and skip logic used during self-administration of the Web-based survey.
Statistical Analysis
In the initial analysis, the overall prevalence rates for lifetime and past-year illicit use of prescription stimulant drugs were examined. We also calculated prevalence rates for illicit use of prescription stimulants for subgroups defined by sex, race-ethnicity, and age of onset. Data were weighted to account for the overall student population sampling fractions. We used multiple logistic regression analyses to examine associations between these subgroups and illicit use of prescription stimulants. Prevalence rates of motives for illicit use of prescription stimulants among lifetime users were also calculated, and χ2 analyses were used to test for differences in motives by sex, race-ethnicity, and age of onset. Finally, prevalence rates for routes of administration of prescription stimulants by lifetime users were calculated, and χ2 analyses were performed to test for differences in routes of administration by sex, race-ethnicity, and age of onset. An α level of 0.05 was used for each statistical test.
Results
Prevalence of Illicit Use of Specific Stimulants
Three-hundred eighty-two (8.3%) of the 4580 respondents had used illicit prescription stimulants in their lifetime, and 269 (5.9%) had used illicit prescription stimulants in the past year. As shown in Table 1, approximately three of every four (75.8%) illicit prescription stimulant users reported taking amphetamine-dextroamphetamine in the past year, and approximately one in four (24.5%) reported using methylphenidate products. Less than 3% each was reported for modafinil, amphetamine, methamphetamine, or pemoline. There were no differences in the past-year illicit use of prescription stimulants between men and women. However, there were statistically significant ethnic-racial differences in past-year use: Hispanics 8.5%, Caucasians 7.0%, Asians 3.4%, African-Americans 1.9%, and those categorized as other 3.6% (χ2 39.7, df=4, p<0.001; Figure 2).
Table 1.
Specific Prescription Stimulants Used in the Past Year by 269 Students (weighted dataa) Reporting Illicit Use of Any Prescription Stimulant
| Stimulant | No. (%)b of Users |
|---|---|
| Amphetamine-dextroamphetamine (e.g., Adderall) | 204 (75.8) |
| Methylphenidate (e.g., Ritalin, Concerta, Metadate, Methylin) | 66 (24.5) |
| Modafinil (e.g., Provigil) | 7 (2.6) |
| Amphetamine (e.g., Benzedrine) | 7 (2.4) |
| Methamphetamine (e.g., Desoxyn) | 2 (0.8) |
| Pemoline (e.g., Cylert) | 0 (0.0) |
| Other | 4 (1.6) |
| Don’t know the names of some I have used | 9 (3.2) |
| Rather not say or did not specify | 29 (11.0) |
Data were weighted to account for the overall student populations sampling fractions.
Total exceeds 100% because respondents were instructed to check all categories that applied.
Figure 2.
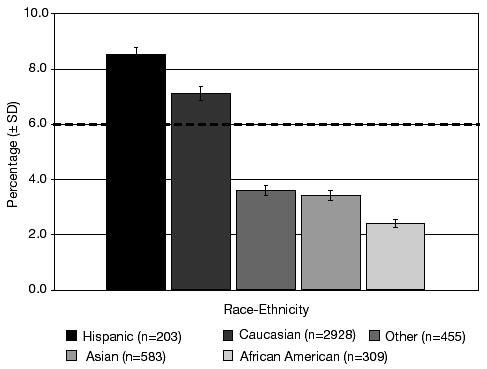
Past-year prevalence of illicit use of prescription stimulants as a function of race-ethnicity (4478 students, weighted data). The dashed line represents overall prevalence rate for past-year illicit use of prescription stimulants.
The effects of race and ethnicity were further examined in a series of multiple logistic regression analyses. Four dummy variables were constructed to represent the information for the five-category race-ethnicity variable. When African-Americans were used as the reference group, the odds of past-year illicit use of prescription stimulants were more than 3 times higher among Caucasians (odds ratio [OR] 3.1, 95% confidence interval [CI] 1.5–6.6) and Hispanics (OR 3.8, 95% CI 1.6–9.3). There were no statistically significant differences between Asians and African-Americans in the odds of past-year illicit use of prescription stimulants. Analyses using Asians as the reference group showed that the odds of past-year illicit use of prescription stimulants were over twice as high among Caucasians (OR 2.1, 95% CI 1.3–3.4) and Hispanics (OR 2.6, 95% CI 1.4–5.1). A final analysis using Caucasians as the reference group showed that there was no statistically significant difference between Caucasians and Hispanics in the odds of past-year illicit use of prescription stimulants.
Most lifetime illicit prescription stimulant users began using in college (65.2%) compared with precollege (34.8%). Logistic regression analysis showed that students who began illicitly using prescription stimulants before college were almost 3 times more likely than students who began using in college to report illicit use of prescription stimulants in the past year (OR 2.8, 95% CI 1.8–4.5).
Motives for Illicit Use
As shown in Table 2, the most commonly reported motives for illicit use of prescription stimulants were to help with concentration (65.2%), help study (59.8%), and increase alertness (47.5%). Other common motives were to get high (31.0%) and to experiment (29.9%).
Table 2.
Motives and Routes of Administration for Illicit Use of Prescription Stimulants Reported by 382 Lifetime Users (weighted dataa)
| Variable | No. (%) of Users |
|---|---|
| Motive | |
| Because it helps me concentrate | 249 (65.2) |
| Because it helps me study | 228 (59.8) |
| Because it helps increase my alertness | 181 (47.5) |
| Because it gives me a high | 118 (31.0) |
| Because of experimentation | 114 (29.9) |
| Because it helps me lose weight | 37 (9.7) |
| Other (specify) | 19 (5.0) |
| Because it counteracts the effects of other drugs | 18 (4.8) |
| Because it is safer than street drugs | 17 (4.5) |
| Because I’m addicted | 4 (1.0) |
| Rather not say | 2 (0.5) |
| Route of Administration | |
| Orally | 363 (95.3) |
| Snorting | 145 (38.1) |
| Smoking | 22 (5.6) |
| Inhaling | 2 (0.6) |
| Injecting | 0 (0.0) |
| Other (specify) | 2 (0.4) |
Data were weighted to account for the overall student populations sampling fractions.
Sex-based differences emerged for several categories of motives. To experiment was reported by 34.6% of men versus 18.2% of women (p<0.05), and to counteract the effect of other drugs was cited by 7.4% of men versus 1.8% of women (p<0.05). In contrast, women were more likely than men to report using prescription stimulants to lose weight (18.2% vs 3.2%, p<0.001), to help study (66.7% vs 54.8%, p<0.05), and to help increase alertness (58.8% vs 38.7%, p<0.001). Finally, there were no sex differences in the most frequently reported motive, which was to help concentrate. Sex-based comparisons for the most commonly reported motives are presented in Figure 3.
Figure 3.
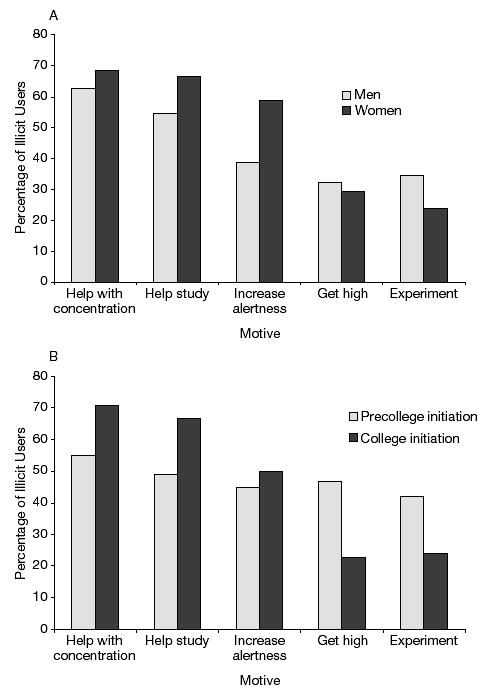
Relationships between the most commonly reported motives for illicit use of prescription stimulants and sex (A) and age of initiation of illicit use of prescription stimulants (B) among 382 students reporting lifetime illicit use of prescription stimulants (weighted data).
Some ethnic-racial differences were also observed with regard to motivation. To get high was not reported by any African-Americans, whereas it was cited by significant percentages of prescription stimulant abusers in other categories: Caucasians 32.4%, Asians 21.9%, Hispanics 21.4%, and others 46.2% (χ2 9.6, df=4, p<0.05). Similar results were found for the motive to experiment; that is, Caucasians, Asians, Hispanics, and others were more likely than African-Americans to report this as a motive (χ2 10.8, df=4, p<0.05). Most African-American illicit prescription stimulant users reported to help concentrate (eight students) and to help study (six students) as their motive for use.
Finally, there were differences in motives based on when students began illicit use of prescription stimulants (Figure 3). Compared with students who started before college, students who started during college were more likely to report the motives of improving concentration (70.7% vs 55%, p<0.01) and helping to study (66.5% vs 48.9%, p=0.001). Conversely, precollege illicit users of prescription stimulants were more likely than their counterparts to report using these agents to get high (46.6% vs 22.8%, p<0.001), to lose weight (15.3% vs 6.5%, p<0.01) and to experiment (42.0% vs 24.0%, p<0.001).
Routes of Administration
As shown in Table 2, nearly every illicit prescription stimulant user (95.3%) reported oral administration, and 38.1% reported snorting these agents. A much smaller proportion of illicit users reported smoking stimulants (5.6%), and less than 1% was reported for other routes of administration, such as inhalation and injection.
We examined associations between sex, race-ethnicity, grade of onset, and the three most frequent routes of administration (oral, intranasal, and smoking). Neither sex nor race-ethnicity was significantly associated with any route of administration. There was also no difference in rates of oral administration between students who started during college versus before college. However, students who began illicitly using prescription stimulants before college were more likely to report snorting prescription stimulants (54.2%) than those who started during college (30.5%) (χ2 20.25, df=1, p<0.01). Further, those who reported precollege onset of illicit prescription stimulant use were more likely to report smoking these agents (11.5%) than those whose onset was during college (2.8%) (χ2 11.52, df=1, p<0.01).
Discussion
Prevalence of Illicit Use of Specific Prescription Stimulants
The lifetime and past-year prevalence rates of illicit use of prescription stimulants found in our study resemble findings from single-institution9 and national studies4, 5 of college students that used similar survey items. To our knowledge, this is the first study to provide evidence that amphetamine-dextroamphetamine is being illicitly used by college students at higher rates than methylphenidate. In fact, amphetamine-dextroamphetamine was reported more frequently than any other stimulants assessed in our study. Two hundred four (75.8%) of the 269 past-year illicit users reported having taken amphetamine-dextroamphetamine, whereas only 66 (24.5%) reported having taken methylphenidate. Forty-eight students (18.0%) reported using both amphetamine-dextroamphetamine and methyl-phenidate.
In the only other study of college students that provided prevalence rates for illicit use of amphetamine-dextroamphetamine, students reported using methylphenidate at higher rates than amphetamine-dextroamphetamine (7.3% vs 4.0%), and the use of both was reported by 24% of respondents, thus exceeding the prevalence of either drug alone.2 The difference in findings may be explained by changing trends in illicit use of specific prescription stimulants or by differences in survey methodology.
The popular press often identifies Adderall as being one of the primary prescription stimulants used illicitly by high school and college students.12–14 Our study is the first to empirically document this claim using random sampling of an undergraduate student population. Furthermore, our findings suggest that other studies may benefit by asking specifically about amphetamine-dextroamphetamine products, as studies that overlook these agents may seriously underestimate the prevalence of prescription stimulant abuse among adolescents and young adults. However, it should be noted that differences in methodology often make it difficult to directly compare studies that assess the illicit use of prescription stimulants.15 Different studies have included various brand names and formulations in their surveys, and whereas some have listed the brand names as individual choices, other studies have grouped multiple brand names together as a single item. For example, many national studies of prescription stimulant abuse have included methylphenidate and/or Ritalin as individual items, but they have not specifically included amphetamine-dextroamphetamine products.4, 8
Several hypotheses have been suggested as to why illicit use of amphetamine-dextroamphetamine appears to be growing relative to other stimulant formulations. These hypotheses generally fall into three categories: availability, pharmacokinetic differences between stimulant drugs, and pharmacologic differences between stimulant drugs. For example, in one of the few other studies to specifically address illicit use of amphetamine-dextroamphetamine, college students reported that they believed Adderall was popular for illicit use because it was easily accessible, caused fewer emotional ups and downs (than alternative agents), and was believed to work better overall.6 Although that study6 did not use a random, representative sample of students or assess medical availability of stimulant drugs, it still provides insight as to why illicit amphetamine-dextroamphetamine use is growing on college campuses.
Pharmacokinetic differences among various formulations support students’ perceptions of experiencing less ups and downs with certain agents compared with others. For example, Adderall XR is an extended-release formulation with a duration of action of approximately 10–12 hours. This is significantly longer than the duration of action of most methylphenidate formulations, with the exception of Concerta (methylphenidate; McNeil Consumer & Specialty Pharmaceuticals, Fort Washington, PA). Immediate-release methylphenidate lasts at most for 6 hours; this short duration of action may contribute to perceived emotional fluctuations. In fact, among children with ADHD, this short duration of action and resultant multiple daily dosing has led to the so-called roller coaster response.16
The mechanism of action of amphetamine-dextroamphetamine may also be a factor in its increasing popularity among illicit prescription stimulant users. Like methylphenidate, amphetamines increase dopamine levels in the brain by blocking the dopamine transporter. However, amphetamines also cause presynaptic release of dopamine. Thus, amphetamine-dextroamphetamine may generate higher dopamine levels in the brain than occur after taking methylphenidate products.17 Furthermore, amphetamine-dextroamphetamine increases levels of norepinephrine, which has been associated with improved cognitive functioning.18 Some researchers have speculated that these differences in mechanism (i.e., higher dopamine levels and the addition of noradrenergic effects) may explain why patients with ADHD respond differently to different stimulant drugs.19 College students may also experience subjectively better responses to certain stimulants when illicitly using them to enhance their academic performance.
To our knowledge, no study has specifically assessed the relationship between availability of specific prescription stimulants and their illicit use. However, as Adderall XR is the most commonly prescribed brand-name prescription stimulant in the United States,19 it is possible that increased availability has resulted in increased illicit use. This hypothesis is purely speculative until it can be adequately tested using valid data on medical availability.
The findings that African-Americans were less likely than Hispanics and Caucasians to report illicit prescription stimulant use accord with results from a national college-based study5 and a national study of 8th, 10th, and 12th graders.20 Both studies found that African-American youths were less likely than other students to report illicit use of methylphenidate. It appears that African-American students of various ages report less illicit use of prescription stimulants. In fact, according to a national survey of high school seniors, African-American students reported less substance use overall than most other racial-ethnic categories.21 It is unclear why African-American students are reporting less drug use, including illicit use of prescription stimulants. African-Americans have more conservative norms and attitudes toward the use of alcohol.22 Thus, it is possible that these attitudes are also held by African-American students with regard to illicit use of prescription stimulants.
Motives for Illicit Use
This study builds on our earlier findings that college students are illicitly using prescription stimulants for a variety of reasons.9 In particular, students report motivation to enhance their academic performance, with most illicit users of prescription stimulants reporting improved concentration and help with studying as their motives for illicit use. Attention to motives for substance abuse is important because users’ motives are often linked to other behaviors associated with drug use. For example, research on motivations for alcohol use has shown that mood regulation is an important reason for drinking alcohol.23 Our findings highlight the importance of the academic environment (e.g., level of competitiveness) as a factor that may increase motivations for illicit stimulant use. They also illustrate the heterogeneous nature of motivations for stimulant abuse.5
Our study revealed several sex-based differences in motives for illicit stimulant use. These findings conflict with our own previous findings9 as well as those of other researchers.2,24 Of particular interest is evidence that academic-related motivations for illicit prescription stimulant use (i.e., to help study or help increase alertness) are more salient for women than for men. To our knowledge, this is the first study to report sex-based differences in motivations for illicit stimulant use. Discrepancies between our results and findings from earlier studies may be related to differences in survey methodology. For example, three items for which we found sex-based differences in this study (to help study, experiment, and lose weight) were not included in our previous survey as fixed items.9 However, two other motives for which we found sex-based differences in this study (increase alertness, counteracts the effects of other drugs) were included in our previous survey, which did not show sex-based differences. It may be that sex-based differences in motives for illicit prescription stimulant use are increasing over time, but this hypothesis can be tested only with longitudinal data.
Our study is also the first we are aware of to document ethnic-racial differences in students’ motives for illicit prescription stimulant use. In particular, African-Americans who reported the illicit use of prescription stimulants were less likely to cite getting high or experimentation as motives than stimulant users in other ethnic groups. This finding may be related to the lower prevalence rates of illicit use of prescription stimulants among African-Americans as compared with other student populations. These findings need to be validated by other studies before firm conclusions can be made.
Finally, it is interesting that the motives to help study and to improve concentration were reported more frequently by students who began illicit use of prescription stimulants in college rather than before college. This finding suggests that some students are seeking academic performance enhancement through the help of prescription stimulants once they arrive at college. It may be that some students are more vulnerable than others to the pressures of college life and are more likely to use stimulants and other substances to cope with this pressure. Clearly, more work is needed to explore the implications of age of onset for illicit prescription stimulant use, especially with regard to the effects of stimulant use on academic performance.
Routes of Administration
Whereas most illicit prescription stimulant users reported oral administration, it is notable that 38% of illicit users reported snorting prescription stimulants. One other study assessed this behavior among college students and found that almost 13% of the students used methylphenidate intranasally.1 Clearly, this form of drug use needs to be addressed through education and prevention, as the pharmacokinetics of prescription drugs can be dramatically altered when they are taken by routes other than the ones for which they are intended. For example, the effects and hence the abuse liability of methylphenidate are increased when it is taken by routes that cause rapid increases in serum concentrations (e.g., injection, insufflation).25 Hence, college students who use prescription stimulants by alternate routes of administration, such as intranasal, may be increasing their vulnerability for dependence on these drugs, even if they started for apparently innocuous purposes (e.g., to enhance studying).
Information about routes of illicit drug administration is crucial to the development of clinical, prevention, policy, and educational efforts for reducing these behaviors and the negative consequences that may result. The United States Food and Drug Administration (FDA) has shown recent attention to the cardiovascular risks associated with prescription amphetamine-dextroamphetamine products. In fact, the FDA has developed a Web site (http://www.fda.gov/cder/drug/infopage/adderall/default.htm) that both patients and clinicians can access to learn more about the health risks associated with Adderall and Adderall XR. Whereas most individuals exposed to prescription stimulants are unlikely to experience serious adverse events, students who illicitly use prescription stimulants without appropriate medical advice may be putting themselves at risk, particularly if they use an alternative route of administration. Given the widespread illicit use of prescription stimulants reported on U.S. college campuses, students, clinicians, and others who interact with students must be educated about the potential adverse events associated with these potent psychostimulants.
Limitations
Several limitations should be considered before assessing the implications of our findings. Our sample consisted of students from a single university, which may limit the generalizability of our results. Although the prevalence rates of illicit use of prescription stimulants in this single-institution study were comparable to those found in national surveys of college students,4, 5 similar investigations need to be conducted in diverse samples, including young adults who are not attending college, to assess the generality of the findings.
Although we achieved an adequate response rate, nonresponse may have introduced bias in our study. However, concerns regarding non-response were reduced because the demographic characteristics of the sample closely resembled those of the overall student population. In addition, we assessed the potential impact of nonresponse by administering a brief telephone survey to 159 nonrespondents and found no significant differences in alcohol and other drug use between respondents and nonrespondents.
This study did not include an individual survey item for dextroamphetamine (e.g., Dexedrine; GlaxoSmithKline, Research Triangle Park, NC). However, in a national survey of high school seniors that includes a survey item for Dexedrine, the annual prevalence rate of illicit use of Dexedrine has not risen above 1% since 1985.7 Furthermore, a recent report using data from IMS Health’s NPA Plus (1992–2002) demonstrates that the use of dextroamphetamine represents a small percentage of the overall number of filled stimulant prescriptions.26 Therefore, it seems unlikely that the omission of dextroamphetamine products in our survey would have had a large impact on our findings. Also, our study did not distinguish between various formulations of each stimulant (e.g., Adderall vs Adderall XR), which may have important clinical and/or research implications. Finally, this study did not contain diagnostic information such as ADHD, which would help us determine which students may be self-medicating due to untreated ADHD.
Future Directions for Research
Studies to investigate the impact of psycho-stimulants on academic performance are needed; in particular, studies to explore any differences in academic performance based on specific stimulants with varying mechanisms of action will contribute to our knowledge regarding the illicit use of prescription stimulants. More work is clearly needed to assess ethnic-racial differences in the prevalence of illicit use of prescription stimulants in diverse populations, including nonacademic environments, in addition to validating our findings among other samples of college students. Future work should examine whether intranasal administration increases a student’s vulnerability for abuse and/or dependence. This should include an assessment of age of initiation of illicit prescription stimulant use as this was shown to have an impact on the route of administration; precollege illicit users were more likely to report intranasal administration or smoking as a route of administration for prescription stimulants. It is unknown why precollege illicit stimulant users report higher rates of nonoral administration compared with college initiators, but it may be associated with differences in motives for use between the two groups. This also must be further elucidated through research efforts.
The impact of pharmaceutical delivery systems on the abuse potential of prescription psycho-stimulants would clearly provide valuable information on this potential approach to decreasing the illicit use of these drugs. For example, one study found that a once-daily osmotic controlled-release formulation of methylphenidate had less abuse potential than immediate-release methylphenidate.27 However, the impact of such delivery systems on long-term development of substance abuse and dependence are unknown.
Conclusion
Amphetamine-dextroamphetamine was clearly the most prevalent stimulant drug used illicitly by college students, at rates 3 times higher than that of methylphenidate formulations (e.g., Ritalin, Concerta, Metadate, Methylin). Thus, studies that rely solely on methylphenidate as an indicator for illicit use of prescription stimulants may underestimate the prevalence of this form of drug abuse.
Hispanic and Caucasian students had higher rates of illicit prescription stimulant use than Asians and African-Americans, but no sex-based differences in use were apparent. College students are illicitly using prescription stimulants for a variety of reasons, with academic performance ranking among the top. In fact, the three most commonly reported motives for illicit use of prescription stimulants seemed related to a desire for enhanced academic performance. Motives linked to academic performance were higher in women than in men and in students who began illicit use of prescription stimulants in college versus before college. Our findings of high rates of intranasal use of prescription stimulants highlight the need for education and prevention efforts aimed at reducing this dangerous behavior.
Clinicians who prescribe stimulant drugs to their patients carry the responsibility of weighing the benefits and risks of these agents. Prescription stimulants are highly effective for treating ADHD and other conditions. However, if they are used without appropriate therapeutic monitoring and management, dangerous health consequences can occur.
Acknowledgments
We would like to thank Dr. Margaret E. Gnegy for her consultation regarding the basic pharmacology of the psychostimulants.
Footnotes
Presented as a poster at the annual meeting of the American College of Clinical Pharmacy, San Francisco, California, October 23–26, 2005.
Supported by a research grant (R03 DA 018239) from the National Institute on Drug Abuse, National Institutes of Health, Bethesda, Maryland.
References
- 1.Babcock Q, Byrne T. Student perceptions of methylphenidate abuse at a public liberal arts college . J Am Coll Health. 2000;49:143–5. doi: 10.1080/07448480009596296. [DOI] [PubMed] [Google Scholar]
- 2.Low KG, Gendaszek AE. Illicit use of psychostimulants among college students: a preliminary study . Psychol Health Med. 2002;7:283–7. [Google Scholar]
- 3.Teter CJ, McCabe SE, Boyd CJ, Guthrie SK. Illicit methylphenidate use in an undergraduate student sample: prevalence and risk factors . Pharmacotherapy. 2003;23:609–17. doi: 10.1592/phco.23.5.609.34187. [DOI] [PubMed] [Google Scholar]
- 4.Johnston LD, O’Malley PM, Bachman JG, Schulenberg JE. Monitoring the future: national survey results on drug use, 1975–2003. Volume II: college students and adults ages 19–45. Bethesda, MD: National Institute on Drug Abuse; 2004. NIH publication no. 04-5508. [Google Scholar]
- 5.McCabe SE, Knight JR, Teter CJ, Wechsler H. Nonmedical use of prescription stimulants among college students: prevalence and correlates from a national survey . Addiction. 2005;100:96–106. doi: 10.1111/j.1360-0443.2005.00944.x. [DOI] [PubMed] [Google Scholar]
- 6.University of Maryland Center for Substance Abuse Research. Maryland drug early warning system. New student drug research (SDR) survey examines prescription stimulant misuse among college students, July 2005. [Accessed April 19, 2006.]; Available from www.cesar.umd.edu.
- 7.Johnston LD, O’Malley PM, Bachman JG, Schulenberg JE. Monitoring the future: national survey results on drug use, 1975–2003. Volume I: Secondary school students (NIH publication no. 04-5507) Bethesda, MD: National Institute on Drug Abuse; 2004. [Google Scholar]
- 8.Office of Applied Studies. Results from the 2002 national survey on drug use and health: national findings. DHHS publication no. SMA 04–3964, NSDUH Series H–25. Rockville, MD: Substance Abuse and Mental Health Services Administration; 2003. [Google Scholar]
- 9.Teter CJ, McCabe SE, Cranford JA, Boyd CJ, Guthrie SK. Prevalence and motivations for the illicit use of prescription stimulants in an undergraduate student sample . J Am Coll Health. 2005;53:253–62. doi: 10.3200/JACH.53.6.253-262. [DOI] [PubMed] [Google Scholar]
- 10.Wechsler H, Lee JE, Kuo M, Seibring M, Nelson TF, Lee H. Trends in college binge drinking during a period of increased prevention efforts: findings from 4 Harvard School of Public Health college alcohol study surveys: 1993–2001 . J Am Coll Health. 2002;50:203–17. doi: 10.1080/07448480209595713. [DOI] [PubMed] [Google Scholar]
- 11.McCabe SE, Boyd C, Couper M, Crawford S, D’Arcy H. Mode effects for collecting alcohol and other drug data: Web and U.S. mail. J Stud Alcohol. 2002;63:755–61. doi: 10.15288/jsa.2002.63.755. [DOI] [PubMed] [Google Scholar]
- 12.ABC News. Illicit ‘study drugs’ tempting more students: attention deficit drugs sweep colleges as a way to boost grades, June 2005. [Accessed October 12, 2005.]; Available from http://abcnews.go.com/Primetime.
- 13.FOX News. Study: 1 in 5 teens abused prescription drugs, April 2005. [Accessed August 17, 2006.]; Available from www.foxnews.com/story/0,2933,154190,00.html.
- 14.New York Times. High-school chemistry, February 2005. [Accessed October 12, 2005.]; Available from www.nytimes.com.
- 15.Arria AM, Wish ED. Nonmedical use of prescription stimulants among students . Psychiatr Ann. 2005;35:228–35. doi: 10.3928/0090-4481-20060801-09. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Markowitz JS, Straughn AB, Patrick KS. Advances in the pharmacotherapy of attention-deficit–hyperactivity disorder: focus on methylphenidate formulations . Pharmacotherapy. 2003;23:1281–99. doi: 10.1592/phco.23.12.1281.32697. [DOI] [PubMed] [Google Scholar]
- 17.Greenhill LL. The science of stimulant abuse . Psychiatr Ann. 2005;35:210–14. doi: 10.3928/0090-4481-20060801-07. [DOI] [PubMed] [Google Scholar]
- 18.Pliszka SR, McCracken JT, Maas JW. Catecholamines in attention-deficit hyperactivity disorder: current perspectives . J Am Acad Child Adolesc Psychiatry. 1996;35:264–72. doi: 10.1097/00004583-199603000-00006. [DOI] [PubMed] [Google Scholar]
- 19.Medscape Psychiatry and Mental Health. An established record of efficacy and tolerability makes long-acting stimulants “first-line” therapy for ADHD, 2005. [Accessed April 19, 2006.]; Available from www.medscape.com.
- 20.McCabe SE, Teter CJ, Boyd CJ, Guthrie SK. Prevalence and correlates of illicit methylphenidate use among 8th, 10th, and 12th grade students in the United States, 2001 . J Adolesc Health. 2004;35:501–4. doi: 10.1016/j.jadohealth.2004.02.004. [DOI] [PubMed] [Google Scholar]
- 21.Wallace JM, Bachman JG, O’Malley PM, Johnston LD, Schulenberg JE, Cooper SM. Tobacco, alcohol, and illicit drug use: racial and ethnic differences among U.S. high school seniors, 1976–2000. Public Health Rep. 2002;117(suppl 1):S67–75. [PMC free article] [PubMed] [Google Scholar]
- 22.Galvan FH, Caetano R. Alcohol use and related problems among ethnic minorities in the United States. Alcohol Res Health. 2003;27:87–94. [PMC free article] [PubMed] [Google Scholar]
- 23.Cooper ML, Frone MR, Russell M, Mudar P. Drinking to regulate positive and negative emotions: a motivational model of alcohol use . J Pers Soc Psychol. 1995;69:990–1005. doi: 10.1037//0022-3514.69.5.990. [DOI] [PubMed] [Google Scholar]
- 24.Hall KM, Irwin MM, Bowman KA, Frankenberger W, Jewett DC. Illicit use of prescribed stimulant medication among college students . J Am Coll Health. 2005;53:167–74. doi: 10.3200/JACH.53.4.167-174. [DOI] [PubMed] [Google Scholar]
- 25.Volkow ND, Swanson JM. Variables that affect the clinical use and abuse of methylphenidate in the treatment of ADHD. Am J Psychiatry. 2003;160:1909–18. doi: 10.1176/appi.ajp.160.11.1909. [DOI] [PubMed] [Google Scholar]
- 26.The National Center on Addiction and Substance Abuse at Columbia University. Under the counter: the diversion and abuse of controlled prescription drugs in the U.S., 2005. [Accessed April 19, 2006.]; Available from www.casacolumbia.org.
- 27.Spencer TJ, Biederman J, Ciccone PE, et al. PET study examining pharmacokinetics, detection and likeability, and dopamine transporter receptor occupancy of short- and long-acting oral methylphenidate. Am J Psychiatry. 2006;163:387–95. doi: 10.1176/appi.ajp.163.3.387. [DOI] [PubMed] [Google Scholar]