

Abstract
Objective
The aim was to investigate the hypothesis that patients with first episode schizophrenic disorders have a more favorable treatment response than those with multiple episodes.
Method
A total of 400 inpatients from an ongoing multi-centre, follow-up program who fulfilled ICD-10 criteria for schizophrenic disorders (F2) were assessed at admission to and discharge from hospital using the Positive and Negative Syndrome Scale (PANSS).
Results
At admission, first episode patients (n = 121) showed higher levels of positive symptoms (PANSS positive subscore) and lower ones of negative symptoms (PANSS negative subscore) than multiple episode patients (n = 279), whereas the global disease severity (PANSS total score) was comparable. Analyses of covariance revealed that treatment response (adjusted symptom levels at discharge) was more favorable in first-episode patients, with respect to both positive and negative symptoms.
Conclusion
The results are compatible with the hypothesis that treatment response becomes less favorable during the course of schizophrenic illness. This finding might be associated with progressive neurobiological alterations.
Key words: schizophrenic disorders, first episode, multiple episode, treatment response, PANSS
Introduction
In the past decade there has been increasing interest in early stages of schizophrenic disorders. Numerous studies have shown that a reduction of the duration of untreated psychosis might be associated with a more favorable treatment outcome [6, 25]. These findings are the theoretical basis for early recognition and intervention programs [15]. Furthermore, it seems to be generally accepted that patients suffering from a first episode of a schizophrenic disorder tend to be more responsive to antipsychotic treatment than multiple episode patients [24]. These assumptions have resulted in special recommendations for this group in current treatment guidelines [4, 9, 23].
Indeed, there are several studies which indicate that first episode patients have a favorable treatment response and require lower doses of antipsychotic drugs than multiple episode patients to achieve remission [10, 24]. However, original data comparing first episode with multiple episode schizophrenic disorders with respect to the acute treatment response are rare: Lieberman et al. [16] followed prospectively for up to 5 years a sample of patients with first episode schizophrenic disorders. This study found a clear pattern of decreasing responsiveness to treatment over subsequent episodes of illness in terms of an increased time to remission [17]. Sanger et al. [26] analyzed data from a large multi-centre, double-blind study comparing olanzapine with haloperidol. First episode patients treated with olanzapine showed a greater improvement of psychopathological symptoms than multiple episode patients. However, only slight differences between first and multiple episode patients were found in the haloperidol group.
Furthermore, it is unclear whether patients with first episode schizophrenic disorders display a specific profile of psychopathological symptoms and cognitive impairment. Sanger et al. [26] reported less pronounced negative symptoms in first episode compared with multiple episode patients. Other studies found an increasing frequency of negative symptoms [5, 22] and neuropsychological impairment [7] with a longer duration of illness, which led to the hypothesis of a “neurodegenerative model” of schizophrenic disorders [18]. On the other hand, further studies failed to identify marked differences between first episode and chronic schizophrenic disorders with respect to psychopathological symptoms [20, 27], neuropsychological function [1, 21] or social deficits [11]. These latter results, which indicate that psychopathological and neuropsychological disturbances are already present in early and even premorbid stages of schizophrenic disorder and remain stable in the further course of illness, are more compatible with a “neurodevelopment model”, which hypotheses that schizophrenia has its origin in the early development of the brain.
Taken together, conflicting results have been reported about the clinical characteristics of first episode schizophrenic disorders. The hypothesis of a better treatment response in first episode patients needs further validation.
Based on a large sample of inpatients suffering from schizophrenic disorders and treated under naturalistic conditions, the present study examines differences between first episode and multiple episode patients with respect to psychopathological characteristics at admission and treatment response. The main hypothesis was that first episode patients show a more favorable treatment response than multiple episode patients.
Methods
Subjects
The sample stems from a multi-centre follow-up program (German Research Network on Schizophrenia) [30] conducted in 11 psychiatric university hospitals (Aachen, Berlin, Bonn, Cologne, Düsseldorf, Essen, Göttingen, Hamburg, Mainz, Munich, Tübingen) and three psychiatric district hospitals (Augsburg, Gabersee, Haar). Subjects were randomly selected from all consecutively admitted patients suffering from schizophrenia and related disorders (ICD-10: F20, F21, F22, F23, F24, F25, F28) who were admitted between January 2001 and December 2004 to one of the 14 hospitals mentioned above. The selection process was carried out using randomization software. Subjects were aged between 18 and 65 years. Exclusion criteria were a history of major medical illness, head injury or symptoms of drug or alcohol dependence.
Patients were treated under naturalistic conditions (e.g. pharmacological treatment with antipsychotics, psychosocial treatment like psychoeducation programs, social skill training or family interventions). All patients had given informed, written consent to participate in the study. The study protocol was approved by the local ethics committees.
Assessments
ICD-10 diagnoses (at time of admission) were based on clinical information including interviews with patients, relatives and care providers, according to ICD-10 research diagnostic criteria [29]. First episode disorder was defined by first hospitalization and absence of a prior episode of schizophrenic disorder. Duration of illness was defined as the time since the first occurrence of any psychopathological symptoms.
Global functioning was assessed using the Global Assessment of Functioning Scale (GAF) [3]. Social parameters (partnership, employment state) were assessed with the Strauss-Carpenter scale [28]. Psychopathological characteristics were assessed with the Positive and Negative Syndrome scale for Schizophrenia (PANSS) [13], and the 17-item version of the Hamilton rating scale for Depression (HAM-D) [12].
Ratings were performed within the first 3 days after admission, and repeated at biweekly intervals during the acute inpatient treatment phase as well as at discharge. All raters had been trained for the instruments and a high inter-rater reliability was achieved (ANOVA-ICC > 0.8).
Statistical analyses
The hypothesis that first episode patients show a more favorable treatment response than multiple episode patients was examined using an analysis of covariance (ANCOVA) with a type III sum of squares based on a general linear model procedure. First episode and multiple episode patients were compared with respect to the PANSS total score at discharge from hospital as the primary criterion for treatment outcome, adjusted for the PANSS total score at admission as the confounding variable. Post-hoc analyses were performed for PANSS positive subscore, PANSS negative subscore, PANSS general psychopathology subscore, HAM-D total score and GAF at discharge, adjusted for the respective values at admission. Lower symptom levels and a higher global functioning at discharge (adjusted for respective values at admission) were taken to indicate a favorable treatment response.
Differences with respect to sociodemographic variables, psychopathological symptoms at admission and treatment characteristics between first episode and multiple episode patients were evaluated using the t-test for continuous and the χ2-test for categorical variables. These tests were used in terms of an exploratory analysis.
All statistical analyses were carried out using the SPSS 12.0 Software for Windows. For all statistical analyses a p-value of ≤ 0.05 (2-tailed) was considered as statistically significant.
Results
Description of the sample
In total, 474 patients with schizophrenic disorders (ICD-10: F2) were enrolled in the study. A total of 46 patients (10%) dropped out for different reasons (e.g. withdrawal of informed consent, retrospective violation of inclusion criteria, incomplete information). A further 28 patients (6%) were excluded from the analysis because they were discharged from hospital within seven days after admission. The present sample therefore comprised 400 subjects, 121 with first episode and 279 with multiple episode schizophrenic disorders. Baseline characteristics are shown in Table 1.
Table 1.
Patients characteristics
| First episode (n = 121) | Multiple episode (n = 279) | Total (n = 400) | p-levelb | |
|---|---|---|---|---|
| Age | 32.0 (10.8) | 37.0 (10.9) | 35.5 (11.1) | T = −4.291, p < 0.001 |
| Gender (female) | 43.0% (n = 52) | 43.7% (n = 122) | 43.5% (n = 174) | χ2 = 0.19, p = 0.889 |
| Diagnoses (admission) | χ2 = 26.191, p < 0.001 | |||
| Schizophrenia (F20) | 80.2% (n = 97) | 81.0% (n = 226) | 80.8% (n = 323) | |
| ATPDa (F23) | 13.2% (n = 16) | 2.9% (n = 8) | 6.0% (n = 24) | |
| Schizoaffective disorder (F25) | 4.1% (n = 5) | 15.1% (n = 42) | 11.8% (n = 47) | |
| Others (F21, F22, F24, F28) | 2.5% (n = 3) | 0.7% (n = 3) | 1.6% (n = 6) | |
| Course of illness | ||||
| Age at first symptoms (years) | 28.6 (12.4) | 23.1 (0.1) | 24.7 (11.1) | T = 4.333, p < 0.001 |
| Age at first hospitalization (years) | 29.6 (12.5) | 26.1 (10.6) | 27.1 (11.3) | T = 2.704, p < 0.001 |
| Duration of illness (years) | 3.3 (7.5) | 13.9 (0.9) | 10.7 (11.1) | T = −11.2, p < 0.001 |
| Social functioning | ||||
| Stable partnership | 28.1% (n = 34) | 18.6% (n = 52) | 21.5% (n = 86) | χ2 = 4.476, p = 0.034 |
| Regular employment | 76.0% (n = 92) | 41.9% (n = 117) | 52.3% (n = 209) | χ2 = 39.329, p < 0.001 |
| Global Assessment of Functioning (GAF) at admission | 42.9 (12.3) | 42.3 (11.8) | 42.5 (11.9) | T = 0.502, p = 0.616 |
Values are presented as means (±standard deviation)
a ATPD: Acute and transient psychotic disorders
b First episode patients were compared with multiple episode patients
As expected, first episode patients were younger than multiple episode patients, showed a shorter duration of illness and a higher social functioning in terms of stable partnership and regular employment. First episode patients were more often diagnosed with acute and transient psychotic disorders (ICD-10: F23) and less often with schizoaffective disorders (ICD-10: F25). They were older than multiple episode patients at the time of the occurrence of the first symptoms and at the time of first hospitalization. No differences were found with respect to gender and global functioning (GAF) at admission.
Psychopathological characteristics at admission of first episode patients compared with multiple episode patients
When both groups were compared with respect to psychopathological symptoms at admission (Table 2), significant differences were found with respect to the distribution of positive and negative symptoms: First episode patients showed higher means in the PANSS positive subscore and lower ones in the PANSS negative subscores than multiple episode patients.
Table 2.
Psychopathological characteristics at admission
| First episode (n = 121) | Multiple episode (n = 279) | Total (n = 400) | p-levela | |
|---|---|---|---|---|
| PANSS | ||||
| Total score | 69.6 (20.4) | 72.0 (18.6) | 71.3 (19.2) | T = −1.123, p = 0.262 |
| Positive symptoms | 20.4 (6.3) | 18.5 (6.3) | 19.1 (6.4) | T = 2.720, p = 0.007 |
| Negative symptoms | 15.6 (7.3) | 18.4 (7.2) | 17.6 (7.4) | T = −3.582, p < 0.001 |
| General psychopathology | 33.7 (11.0) | 35.0 (9.7) | 34.6 (10.1) | T = −1.253, p = 0.211 |
| HAM-D total score | 9.8 (6.4) | 10.2 (7.6) | 10.1 (7.3) | T = −0.525, p = 0.600 |
Values are presented as means (±standard deviation)
a First episode patients were compared with multiple episode patients
However, no significant differences were found with respect to the PANSS total score indicating a comparable global severity of illness. The same was also true for the PANSS general psychopathology subscore and the HAM-D score.
Treatment response of first episode patients compared with multiple episode patients
The PANSS total score at discharge was used as the primary criterion for treatment response. The comparisons between first episode patients and multiple episode patients are shown in Fig. 1.
Fig. 1.
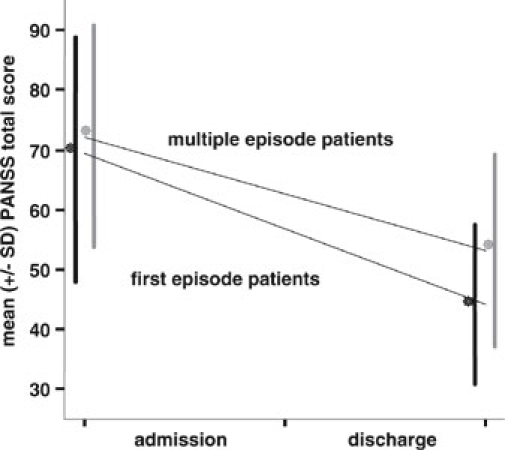
Treatment response (unadjusted changes in PANSS total score) of first episode compared with multiple episode schizophrenic disorders
Both groups were compared using an ANCOVA model with PANSS total score at discharge as the dependent variable and PANSS total score at admission as the covariate: The overall ANCOVA was significant (F = 89.176, df = 2, p < 0.001, adjusted R2 = 0.307), suggesting that 31% of the variance could be explained with this model. Significant differences were found between first episode and multiple episode patients indicating a more favorable treatment response in first episode patients. p-levels and means of PANSS total scores at discharge adjusted for respective levels at admission are shown in Table 3.
Table 3.
Adjusted levels of psychopathological symptoms and global functioning at discharge
| First episode (n = 121) | Multiple episode (n = 279) | p-level | |
|---|---|---|---|
| PANSS | |||
| Total score | 45.1 (CI: 42.8–47.5) | 52.7 (CI: 51.1–54.3) | F = 28.542, df = 1, p < 0.001 |
| Positive symptoms | 9.1 (CI: 8.5–9.7) | 11.1 (CI: 10.7–11.5) | F = 26.249, df = 1, p < 0.001 |
| Negative symptoms | 13.5 (CI: 12.6–14.5) | 15.0 (CI: 14.3–15.6) | F = 6.030, df = 1, p = 0.014 |
| General psychopathology | 22.9 (CI: 21.7–24.1) | 26.5 (CI: 25.7–27.3) | F = 25.215, df = 1, p < 0.001 |
| HAM-D total score | 3.6 (CI: 2.8–4.4) | 4.4 (CI: 3.9–4.9) | F = 2.336, df = 1, p = 0.125 |
| GAF | 71.0 (CI: 69.0–73.0) | 62.9 (CI: 61.6–64.2) | F = 44.537, df = 1, p < 0.001 |
Values are presented as adjusted means for scores at admission and 95% confidence intervals in parenthesis
Post hoc analyses (ANCOVA-model) revealed that first episode patients showed lower levels in the PANSS positive subscore, the PANSS negative subscore and the PANSS general psychopathology subscore at discharge than multiple episode patients, too. On the other hand, first episode patients showed a higher level of the Global Assessment of Functioning (GAF) score at discharge than multiple episode patients. No significant differences, however, were found with respect to the total HAM-D score at discharge. Symptom levels and global functioning at discharge were adjusted for respective values at admission (Table 3).
Treatment characteristics are shown in Table 4. No differences between first episode and multiple episode patients were found with respect to the duration of hospitalization and the frequency of treatment with tranquilizers, first generation antipsychotics or second generation antipsychotics. However, first episode patients were less often treated with antidepressant drugs and mood stabilizers.
Table 4.
Treatment characteristics
| First episode (n = 121) | Multiple episode (n = 279) | Total (n = 400) | p-levela | |
|---|---|---|---|---|
| Duration of hospitalization (days) | 53.7 (39.1) | 53.4 (47.0) | 53.5 (44.7) | T = 0.048, p = 0.962 |
| Medicationb | ||||
| First generation antipsychotics | 69.4% (n = 84) | 63.8% (n = 178) | 65.5% (n = 262) | χ2 = 1.181, p = 0.277 |
| Second generation antipsychotics | 46.3% (n = 56) | 52.7% (n = 147) | 50.8% (n = 203) | χ2 = 1.386, p = 0.239 |
| Antidepressants | 11.6% (n = 14) | 23.3% (n = 65) | 19.8% (n = 79) | χ2 = 7.323, p = 0.007 |
| Tranquilizers | 57.9% (n = 70) | 50.9% (n = 142) | 53.0% (n = 212) | χ2 = 1.639, p = 0.200 |
| Mood stabilizers | 5.8% (n = 7) | 14.3% (n = 40) | 11.8% (n = 47) | χ2 = 5.952, p = 0.015 |
Values are presented as means (±standard deviation)
a First episode patients were compared with multiple episode patients
b Multiple entries are possible. The duration of application of these drugs during the whole inpatient treatment period is not mentioned in this presentation
Discussion
Sample
Based on a sample of 400 inpatients suffering from schizophrenic disorders (ICD-10: F2), the aim of the present study was to compare first episode (n = 121) with multiple episode patients (n = 279) with respect to sociodemographic and other clinical variables, psychopathological symptoms and treatment response. The sample was randomly selected from all patients consecutively admitted to university or district hospitals. In contrast to the study by Sanger et al. [26], patients in the present study did not have to fulfill the strict inclusion criteria of a clinical double-blind trial.
Patients were treated under naturalistic conditions. Differences between first episode and multiple episode patients were found with respect to the frequency of treatment with antidepressant drugs and mood stabilizer. Surprisingly, a high administration rate of first generation antipsychotics was found in both groups. This finding may be explained by the fact that the group of first generation antipsychotics includes low potency antipsychotics that are often used for the treatment of agitation and sleep disturbances.
Treatment response
The present study was able to confirm the hypothesis that first episode patients have a more favorable treatment response than multiple episode patients: First-episode patients showed lower levels in PANSS total scores at discharge (the primary outcome criterion) than multiple episode patients. The same was true for the PANSS subscores for positive symptoms, negative symptoms and general psychopathology at discharge. On the other hand, first-episode patients showed higher levels in the Global Assessment of Functioning (GAF) score at discharge than multiple episode patients. Statistical analyses were adjusted for the respective scores at admission as confounding variables (ANCOVA-model).
Similar results were reported by Sanger et al. [26], who compared first episode (n = 83) and multiple episode patients (n = 1913) with respect to the reduction of psychopathological symptoms after 6 weeks antipsychotic treatment with haloperidol or olanzapine. In this study, only first episode patients treated with olanzapine (n = 58) showed a greater improvement in PANSS total scores than multiple episode patients of this group, whereas no significant differences were found between first episode (n = 24) and multiple episode patients in the haloperidol group. Furthermore, no significant differences were found with respect to the changes of PANSS negative subscores either in the haloperidol or the olanzapine group. These conflicting findings may result from a lower statistical power, especially in the haloperidol group, and the fact that the analyses were not adjusted for baselines scores.
The results of the present study, i.e. that first episode patients show a more favorable treatment response than multiple episode patients, are compatible with the findings of Lieberman et al. [17] who followed prospectively a sample of first episode patients and found a decreased responsiveness to treatment over subsequent episodes in terms of an increased time to remission. The present study failed to reveal differences between first episode and multiple episode patients with respect to the duration of hospitalization. In contrast to Lieberman et al. [17], however, the time to remission was not addressed in the present study, and the duration of hospitalization is not only influenced by the time to remission.
Psychopathological characteristics
Although the overall severity of schizophrenic symptoms (PANSS total score) was comparable in both groups, first episode patients showed more pronounced positive symptoms (PANSS positive subscore) and less pronounced negative symptoms (PANSS negative subscore) than multiple episode patients at admission. With respect to depressive symptoms, no significant differences were found between the two groups at admission.
These findings are in line with those of Sanger et al. [26], who also reported lower means of PANSS negative subscores in first episode patients before antipsychotic treatment. The results are also compatible with those of Murphy et al. [22] and Bottlender et al. [5], who found an increasing frequency of negative symptoms with a longer duration of illness. Conflicting results, however, have been reported by Shtasel et al. [27], who compared 37 first episode patients with 70 chronic schizophrenic patients and found no marked differences in the psychopathological symptom profile, and especially no differences with respect to negative symptoms. However, these results are limited by the small sample size. The same is true for the study by Moritz et al. [20] who compared 20 first episode patients with 36 chronic patients and found a comparable psychopathological profile for both groups.
Disease progression in schizophrenic disorders or sampling effect?
The findings that multiple episode patients have more pronounced negative symptoms and a less favorable treatment response than first episode patients are compatible with the model of a progressive and deteriorating illness [5, 18], which derives from Kraepelin’s original concept of “dementia praecox” [14]. The progressive course might be associated with neurobiological alterations. However, this concept may apply only to a subgroup of patients with schizophrenic disorders.
These conclusions, however, should be regarded with caution. One has to consider that the results of the present cross-sectional study could reflect a sampling bias because patients with an initially more unfavorable course of illness have a higher likelihood of further hospitalizations, regardless of whether there is a progressive course or not. In this context, one has to note that first episode patients were older than multiple episode patients at the time of the occurrence of the first symptoms and at the time of first hospitalization. Similar results indicating an earlier onset of illness in the group of multiple episode patients were reported by previous studies [2, 26, 27] although these surprising findings were not discussed in detail. Other studies, however, revealed that patients with an early onset of schizophrenic disorders show a poorer response to antipsychotic treatment [19] and a higher risk for further hospitalization [8], which might explain the results mentioned above in terms of a sampling effect.
Limitations
The present analysis is limited by its cross-sectional design, so that conclusions about the concept of disease progression should be made with caution because the results could reflect a sampling bias.
Furthermore, one has to consider that symptom levels and global functioning at discharge from hospital were used as criterion for treatment response. Follow-up examinations were not included in the present study. Therefore, the present analyses are limited to the acute treatment response during the inpatient treatment period.
Moreover, the aim of the present study was to examine an unselected and representative sample of patients routinely treated in a psychiatric hospital. Patients were treated under naturalistic conditions and effects of medication were not controlled. Therefore, the results could be confounded by potential treatment differences between first episode and multiple episode patients. Particularly, this may be true for the early course of illness, because systems of care and treatment guidelines have chanced substantially in the past decades.
Finally, one should note that the sample was not limited to patients suffering from schizophrenia, but also included patients with delusional, acute and transient psychotic disorders and schizoaffective disorders in terms of schizophrenic spectrum disorders.
Conclusions
The present study was able to confirm the hypothesis that patients with first episode schizophrenic disorders have a more favorable treatment response than multiple episode patients. The results can be interpreted in terms of a model which considers schizophrenia or a subtype of schizophrenic disorders as a progressive illness. The decrease of treatment response in multiple episode patients might be associated with progressive neurobiological alterations. The differences in treatment response between first episode and multiple episode patients should be considered in the analysis and interpretation of clinical trials comparing antipsychotic drugs.
Acknowledgement
The network study was conducted in 14 psychiatric hospitals: Aachen (P. Hoff, K. Podoll), Augsburg (M. Schmauß, M. Eichinger), Berlin (I. Heuser, M. Jockers-Scherübl), Bonn (W. Maier, K.-U. Kühn, M.R. Lemke, R. Hurlemann), Cologne (J. Klosterkötter, W. Huff), Düsseldorf (W. Gaebel, A. Klimke, M. Eickhoff, M. von Wilmsdorff), Essen (M. Gastpar, V. Reißner), Gabersee (G. Laux, B. Hermann, B. Plichta), Göttingen (E. Rüther, D. Degner), Haar (H. Pfeiffer, M. Albus, S. Scharf-Büssing), Hamburg (D. Naber, D. Golks), Mainz (L.G. Schmidt, B. Kaufmann-Grebe), Munich (H.-J. Möller, R. Bottlender, M. Riedel, M. Jäger, C. Schorr, B. Schillinger, C. Mirlach), Tübingen (G. Buchkremer, M. Mayenberger).
Footnotes
The study was performed within the framework of the German Research Network on Schizophrenia, which is funded by the German Federal Ministry for Education and Research BMBF (grant 01 GI 0233).
References
- 1.Addington J, Addington D (2002) Cognitive functioning in first-episode schizophrenia. J Psychiatry Neurosci 27:188–192 [PMC free article] [PubMed]
- 2.Albus M, Hunmann W, Ehrenberg CH, Forcht U, Mohr U, Sobizack N, Wahlheim CH, Hecht S (1996) Neuropsychological impairment in first-episode and chronic schizophrenic patients. Eur Arch Psychiatry Clin Neurosci 146:249–255 [DOI] [PubMed]
- 3.American Psychiatric Association (1994) Diagnostic and statistical manual of mental disorders, 4th edn. (DSM-IV). American Psychiatric Association, Washington DC
- 4.American Psychiatric Association (2004) Practice guideline for the treatment of patients with schizophrenia, 4th edn. American Psychiatric Association, Washington DC
- 5.Bottlender R, Jäger M, Groll C, Strauss A, Möller HJ (2001) Deficit states in schizophrenia and their association with the length of illness and gender. Eur Arch Psychiatry Clin Neurosci 251:272–278 [DOI] [PubMed]
- 6.Bottlender R, Sato T, Jäger M, Wegener U, Wittmann J, Strauß A, Möller HJ (2003) The impact of untreated psychosis prior to first psychiatric admission on the 15-year outcome in schizophrenia. Schizophr Res 62:37–44 [DOI] [PubMed]
- 7.Cuesta MJ, Peralta V, Zarzuela A (1998) Illness duration and neuropsychological impairments in schizophrenia. Schizophr Res 33:141–150 [DOI] [PubMed]
- 8.Eaton WW, Mortensen PB, Herrman H, Freeman H, Bilker W (1992) Long term course of hospitalization for schizophrenia: part I. Risk for rehospitalisation. Schizophr Bull 18:217–228 [DOI] [PubMed]
- 9.Falkai P, Wobrock T, Lieberman J, Glenthoj B, Gattez WF, Möller HJ, WFSBP Task Force on Treatment Guidelines for Schizophrenia (2005) World Federation of Societies of Biological Psychiatry (WFSBP) guidelines for biological treatment of schizophrenia, part 1: acute treatment of schizophrenia. World J Biol Psychiatry 6:132–91 [DOI] [PubMed]
- 10.Gaebel W, Jänner M, Frommamm (2002) First vs multiple episode schizophrenia: two year outcome of intermittent and maintenance medication strategies. Schizophr Res 53:145–159 [DOI] [PubMed]
- 11.Grant C, Addington J, Addington D, Konnert C (2001) Social functioning in first and multiepisode schizophrenia. Can J Psychiatry 46:746–749 [DOI] [PubMed]
- 12.Hamilton M (1960) A rating scale for depression. J Neurol Neurosurg Psychiatry 23:56–62 [DOI] [PMC free article] [PubMed]
- 13.Kay SR (1991) Positive and negative syndromes in schizophrenia: assessment and research. Clinical and experimental psychiatry monography No. 5 Brunner/Mazel, New York
- 14.Kraepelin E (1899) Psychiatrie, 6th edn. Barth, Leipzig
- 15.Larsen TK, Friis S, Haahr U, Joa I, Johannessen JO, Melle I, Opjordsmoen S, Simonsen E, Vaglum P (2001) Early detection and intervention in first episode schizophrenia: a critical review. Acta Psychiatr Scand 103:323–334 [DOI] [PubMed]
- 16.Lieberman JA, Alvir J, Woerner M, Degreet G, Bilder RM, Ashtari M, Bogerts B, Mayerhoff DI, Geisler SH, Loebel A, Levy DL, Hinrichsen G, Szymanski S, Chakos M, Koreen A, Borenstein M, Kane J (1992) Prospective study of psychobiology in first episode schizophrenia at Hillside Hospital. Schizophr Bull 18:351–371 [DOI] [PubMed]
- 17.Lieberman JA, Koreen AR, Chakos M, Sheitman B, Woerner M, Alvir J, Bilder R (1996) Factors influencing treatment response and outcome of first episode schizophrenia: implications for Understanding the pathophysiology of schizophrenia. J Clin Psychiatry 57(suppl9):5–9 [PubMed]
- 18.Lieberman JA (1999) Is schizophrenia a neurodegenerative disorder? A clinical and neurobiological perspective. Biol Psychiatry 46:729–739 [DOI] [PubMed]
- 19.Meltzer HY, Rabinowitz J, Lee MA (1997) Age at onset and gender in schizophrenic patients in relation to neuroleptic resistance. Am J Psychiatry 154:475–482 [DOI] [PubMed]
- 20.Moritz S, Lambert M, Andresen B, Bothern A, Naber D, Krausz M (2001) Subjective cognitive dysfunction in first-episode and chronic schizophrenic patients. Compr Psychiatry 42:213–216 [DOI] [PubMed]
- 21.Moritz S, Andresen B, Perro C, Schickel M, Kraus M, Naber D, PERSIST Study Group (2002) Neurocognitive performance in first episode and chronic schizophrenic patients. Eur Arch Psychiatry Clin Neurosci 252:33–37 [DOI] [PubMed]
- 22.Murphy BM, Burke JG, Bray JC, Walsh D, Kendler KS (1994) An analysis of the clinical features of familial schizophrenia. Acta Psychiatr Scand 89:421–427 [DOI] [PubMed]
- 23.National Institute for Clinical Excellence (2002) Schizophrenia. Core interventions in the treatment and management of schizophrenia in primary and secondary care. NICE, London
- 24.Ohlsen RI, O’Toole MS, Purvis RG, Walters JTR, Taylor TM, Jones HM, Pilowsky LS (2004) Clinical effectiveness in first episode patients. European Neuropsychopharamacology 14:S445–S451 [DOI] [PubMed]
- 25.Oosthuizen P, Emsley RA, Keyter K, Niehaus DJH, Koen L (2005) Duration of untreated psychosis and outcome in first episode psychosis. Perspective from a developing country. Acta Psychiatr Scand 11:214–219 [DOI] [PubMed]
- 26.Sanger TM, Lieberman JA, Tohen M, Grundy A, Beasly C, Tollefson GD (1999) Olanzapine versus haloperidol treatment in first-episode psychosis. Am J Psychiatry 165:79–87 [DOI] [PubMed]
- 27.Shtasel DL, Gur RE, Gallacher F, Heimberg C, Cannon T, Gur RC (1992) Phenomenology and functioning in first-episode schizophrenia. Schizophr Bull 18:449–462 [DOI] [PubMed]
- 28.Strauss JS, Carpenter WT Jr (1974) The prediction of outcome in schizophrenia. II. Relationsships between predictor and outcome variables: a report from the WHO International Pilot Study of Schizophrenia. Ach Gen Psychiatry 31:37–42 [DOI] [PubMed]
- 29.WHO (1993) The ICD-10 classification of mental and behavioural disorders. Diagnostic criteria for research. WHO, Geneva
- 30.Wölwer W, Buchkremer G, Häfner H, Klosterkötter J, Maier W, Möller HJ, Gaebel W (2003) German research network on schizophrenia. Bridging the gap between research and care. Eur Arch Clin Neurosci 253:321–329 [DOI] [PubMed]