

Abstract
Objectives. We sought to measure the difference in employment rates between HIV-seropositive and HIV-seronegative persons and to establish whether this difference varied according to the HIV-infected persons’ socioeconomic position as defined by education level.
Methods. We used data from the VESPA (VIH: Enquête Sur les Personnes Atteintes) study, a large cross-sectional survey conducted among a nationally representative sample of 2932 HIV-infected patients in France. Age-, gender-, nationality-, and education-standardized employment rates were estimated with the French general population as the reference. The differences in employment rates with the general population were computed overall and according to education level.
Results. Compared with that of the general population, the overall employment rate was 25% lower (95% confidence interval [CI]=16%, 32%) among HIV-infected patients diagnosed before 1994 and 9% lower (95% CI = 5%, 16%) among HIV-infected patients diagnosed from 1994 onward. The difference in employment rates with the general population was significantly higher among patients with a low education level. The employment rate of highly educated HIV-infected patients diagnosed from 1994 onward did not differ from that of the general population.
Conclusions. HIV infection was associated with decreased workforce participation among those with a low education level but not among highly educated individuals.
Employment is a major factor in maintaining income levels and living conditions, especially among patients with long-lasting chronic diseases.1 Moreover, unemployment has been shown to be an independent predictor of morbidity2 and mortality from suicide and external causes3–5 in the general population, thus contributing to social health inequalities in the general population.6
Studies have shown evidence for the existence of an impact of chronic conditions on employment status, including rheumatoid arthritis,7,8 diabetes,9–11 impaired cardiac function,12 and limiting long-standing illness.13,14 This harmful effect of chronic illness on employment has been shown to be higher among the groups with the lowest position in the labor market, i.e., women, low-educated persons, manual workers, and those with the most physically demanding work.15
In Western countries, since 1996 and the wide-scale diffusion of highly active antiretroviral therapies (HAART), HIV infection has become a chronic disease; moreover, the epidemic has shifted toward more socially vulnerable populations, especially immigrants.16–19 In this context, social aspects of HIV infection have emerged as key factors for the management and progression of the disease. Stable partnership and temporary employment (working occasionally) have been shown to constitute independent predictors of health status during the course of the disease as measured by the risk of progression toward AIDS or death,20 or the risk of all-cause hospitalization or death.21 Moreover, because HIV infection mostly affects young adults, patients’ social situation at the time of diagnosis is still largely in evolution, making it likely to be influenced by the disease. The deleterious social impact of HIV infection is likely to be amplified among patients who have the least favorable socioeconomic position at disease outset.22
Studies have reported persistent high unemployment rates among persons living with HIV/AIDS in the era of HAART, ranging from 45% to 65%.23–28 Such unemployment rates are likely to be the result of a debilitating effect of HIV infection on workforce participation, but they may also at least partly reflect sociodemographic or behavioral disadvantages regarding workforce participation (i.e., female gender, advanced age, low educational level, manual occupation, foreign nativity, injection drug use) existing prior to HIV infection.
We sought to measure the difference in employment rates between the population of persons living with HIV/AIDS in France in 2003 and the French general population, taking into account differences in the sociodemographic and educational structure of these 2 populations. Our secondary objective was to establish whether this difference varied according to HIV-infected persons’ socioeconomic position as measured by education level.
We used data from a French nationally representative sample of HIV-infected hospital outpatients. In France, access to care for HIV infection is universal, and because antiretroviral treatments are provided exclusively through hospital physicians’ prescription, HIV infection is mostly managed through hospital outpatient clinics, regardless of disease severity.29 The sample we used has been constituted specifically with the concern for reflecting the diversity of the HIV epidemic in terms both of individuals’ and disease management characteristics, thus allowing us to account for the great heterogeneity in the situations encountered at the country level.
METHODS
We used data from the VESPA (VIH: Enquête Sur les Personnes Atteintes) study, a large cross-sectional survey aimed at studying the social situation and living conditions of HIV-infected individuals in France. The study design has been detailed elsewhere.30 The study was conducted between December 2002 and September 2003 in 102 French hospital departments that delivered HIV care. A total of 4963 HIV-infected outpatients were randomly selected according to the order in which they were received by the participating physicians. The sample was stratified on departments’ geographic location and size of their HIV caseload. Eligible patients were those diagnosed as being infected with HIV-1 for at least 6 months, either French citizens or living in France for at least 6 months, and aged 18 years or older. Patients with very poor understanding of the French language were excluded.
Individuals who agreed to participate signed an informed consent and answered a face-to-face standardized questionnaire administered by a trained interviewer. Information on HIV/AIDS and health status characteristics was documented from medical records.
The nonresponse rate was 41% of the randomized patients overall, with substantial differences according to patients’ HIV-transmission category, employment status, and immunologic status. Major sociodemographic and health-related characteristics were collected among both respondents and non-respondents, allowing for a weighting procedure to take into account this participation bias. This weighting procedure included 2 steps: (1) with the unequal probability of enrollment related to the heterogeneous frequency of patients’ hospital visits, a weight was attributed to each individual that corresponded to the inverse number of hospital visits he or she had reported for the preceding year, and (2) to account for nonresponse, an additional weight was computed with a method of calibration adjustment31 in such a way that the weighted distribution of the participants regarding transmission group, employment status, and immunologic status was comparable to that of the entire eligible population.
Information on the French general population was obtained from the Institut National de la Statistique et des Etudes Economiques (National Institute for Statistics and Economic Studies). Each year, to produce information on the labor force, the Labor Force Survey is conducted in France as well as in each country of the European Union among a nationally representative sample of individuals aged 16 to 64 years who live in private households.32 Employment rates are computed according to age, gender, citizenship (documentation of ethnicity is not allowed in such studies in France), and educational level. For the present analyses, we used data from the 2002 survey (n = 38 164).
For each subject, information was available on the employment status at the time of the study and on major sociodemographic characteristics: age, gender, and citizenship; educational level, dichotomized as low (preprimary, primary, and secondary education) and high (postsecondary education), was used as an indicator of individuals’ socioeconomic position. Moreover, information on past or current injection drug use was available for participants of the VESPA study.
Analyses were restricted to participants of working age (younger than 60 years). Given that HIV-infected individuals diagnosed from 1994 onward have benefited from the advent of HAART much more than those diagnosed earlier, our analyses were performed separately according to the period of HIV diagnosis (before 1994 vs from 1994 onward). Direct standardization was used to estimate age-, gender-, citizenship-, and education-standardized employment rates among HIV-infected individuals, with the sample of the general population as reference. That is, we calculated the employment rates expected among HIV-infected participants stratified by period of HIV diagnosis, assuming they had the same distribution as the general population with regard to sociodemographic characteristics, i.e., age (categorized as<35, 35–49, or ≥ 50 years), gender, citizenship (French or other), and socioeconomic position measured by education level.
The differences in employment rates between HIV-infected individuals and the general population were computed overall and separately according to education level. These differences were calculated with the difference between 100% and the ratio of each standardized employment rate to the reference employment rate. Confidence intervals of the standardized rates and of the rates’ differences were computed with a bootstrap procedure, which allowed us to account for data weighting.
Given that in the analysis described above, (1) to avoid empty strata, citizenship was dichotomized rather than categorized according to the country of origin and (2) information on injection drug use could not be accounted for because it was missing for the reference population, we considered that this analysis might fail to account for all differences potentially associated with employment rate between HIV-infected individuals and the general population. Thus, a complementary analysis restricted to French citizens and HIV-infected individuals who were not injection drug users was performed to check the reproducibility of our results in a more homogeneous subsample.
All statistical analyses were performed with Stata version 7.0 (Stata Corp, College Station, Tex).
RESULTS
Study Population
Among 4963 eligible patients, 2932 participants were included in the VESPA study (global response rate=59%). Two hundred sixty-four were not solicited because of major cognitive impairment or health problems, and 1767 patients declined to participate. Patients who refused most frequently cited a lack of time. Non-respondents were more likely than respondents to be employed at the study time and to have been infected with HIV through a way other than homosexual or bisexual contacts.
For the present analysis, we focused on the 2750 participants of the VESPA study who were aged younger than 60 years at the time of data collection. Median time since HIV diagnosis at the time of the study was 10 years (range, 6 months to 21 years): 1442 had been diagnosed as being infected with HIV before 1994, and 1308 were diagnosed from 1994 onward. Of the participants, 592 were past or current injection drug users (454 diagnosed before 1994 and 138 diagnosed from 1994 onward). The sample of the general population included 35423 individuals aged younger than 60 years. Compared with the general population, HIV-infected participants were more frequently men (73.2% of those diagnosed before 1994 and 68.1% of those diagnosed from 1994 onward vs 49.6% of the general population), aged between 35 and 49 years (77.6% and 53.2% vs 35.4%, respectively), and non–French citizens (9.6% and 29.0% vs 6.6%, respectively); this latter difference was almost exclusively related to a much higher proportion of individuals originating from sub-Saharan Africa among the HIV-infected population (2.5% and 19.6% vs 0.8%, respectively) (Table 1 ▶).
TABLE 1—
Gender, Age, Citizenship, Education Level, and Injection Drug Use Characteristics of the General Population Compared With Those of HIV-Infected Individuals Diagnosed Before 1994 and Diagnosed From 1994 Onward: France
| General Population, % (n = 35 423) | HIV Diagnosis Before 1994,a % (n = 1442) | HIV Diagnosis From 1994 Onward,a % (n = 1308) | |
| Gender | |||
| Men | 49.6 | 73.2 | 68.1 |
| Women | 50.4 | 26.8 | 31.9 |
| Age in 2003, y | |||
| < 35 | 43.5 | 7.2 | 31.4 |
| 35–49 | 35.4 | 77.6 | 53.2 |
| ≥ 50 | 21.1 | 15.2 | 15.4 |
| Citizenship | |||
| France | 93.4 | 90.4 | 71.0 |
| Other European country | 2.9 | 3.7 | 4.1 |
| North Africa | 2.2 | 1.9 | 2.5 |
| Sub-Saharan Africa | 0.8 | 2.5 | 19.6 |
| Other | 0.7 | 1.5 | 2.8 |
| Education level | |||
| High | 29.0 | 29.6 | 30.4 |
| Low | 71.0 | 70.4 | 69.6 |
| Past or current injection drug use | |||
| No | NA | 68.1 | 90.0 |
| Yes | NA | 31.9 | 10.0 |
Note. NA = data not available.
aData concerning HIV-infected individuals were weighted.
Employment Rates
As shown in Figure 1 ▶, crude employment rates reached 53.9% among HIV-infected patients diagnosed before 1994 and 59.3% among HIV-infected patients diagnosed from 1994 onward. Substantial differences were observed according to individuals’ sociodemographic and educational characteristics with lower rates of employment among women (44.6% among HIV-infected women diagnosed before 1994 and 46.9% among those diagnosed later vs 57.3% and 65.1%, respectively, among HIV-infected men), non–French citizens (49.5% and 47.0% vs 54.3% and 64.3%, respectively, among the French), and individuals with low education levels (48.5% and 53.4% vs 66.5% and 72.7%, respectively, among the highly educated). After standardization for characteristics of individuals’ sociodemographic and educational situation, estimated employment rates were 49.0% (95% confidence interval [CI]=44.7%, 55.1%) among HIV-infected individuals diagnosed before 1994 and 59.3% (95% CI=55.0%, 61.9%) among those diagnosed later. The overall employment rate reached 65.3% in the general population, with lower rates among females, non–French citizens, individuals aged younger than 35 years, and those with a low education level.
FIGURE 1—
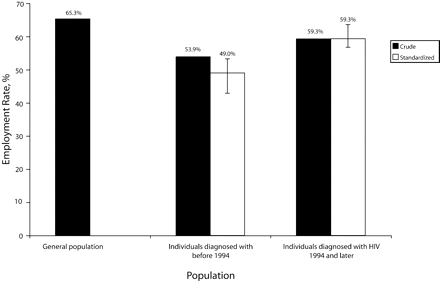
Crude and standardized employment rates (and 95% Confidence Intervals) among individuals diagnosed with HIV before 1994 and from 1994 onward, and employment rates among the French general population.
Difference in Employment Rates Between HIV-Infected Individuals and the General Population
As shown in Figure 2 ▶, compared with that of the general population, overall standardized employment rate was estimated to be 25% lower (95% CI=16%, 32%) for HIV-infected patients diagnosed before 1994 and 9% lower (95% CI=5%, 16%) for those diagnosed later.
FIGURE 2—
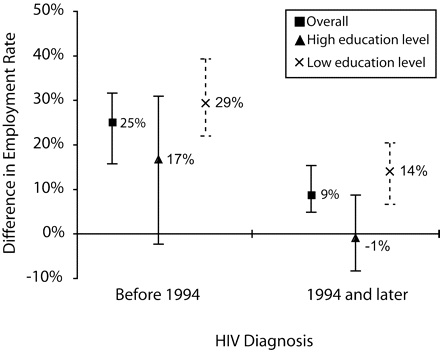
Difference in employment rates (and 95% confidence intervals [CIs]) with the French general population for persons diagnosed with HIV before 1994 and from 1994 onward, overall and according to educational level.
Note. For example, the employment rate of HIV-infected individuals diagnosed from 1994 onward who have a low education level is 14% lower (95% CI = 7%, 20%) than that of individuals who have a comparable educational level in the general population.
The difference in employment rates between HIV-infected participants and the general population varied according to individuals’ socioeconomic position (Figure 2 ▶). For HIV-infected individuals diagnosed from 1994 onward, the employment rate difference with the general population was significantly greater among those with a low education level (difference of 14% [95% CI=7%, 20%]) than among those with a high education level, whose employment rate was comparable to that of the general population of the same sociodemographic and educational characteristics (difference of −1% [95% CI = −8%, 8%]). Among HIV-infected individuals diagnosed before 1994, the difference was less marked, although a similar trend was observed (differences of 29% [95% CI=22%, 39%] for those with a low education level and 17% for those with a high education level [95% CI=−2%, 30%]).
Results remained unchanged when analyses were performed that excluded non–French citizens and the HIV-infected injection drug users.
DISCUSSION
As HIV infection has shifted to population subgroups with poor socioeconomic status, estimation of the social impact of the disease appears to be a key issue. To our knowledge, this study is the first to compare a large and diverse sample of HIV-infected individuals with the general population with regard to a major aspect of patients’ living conditions (i.e., employment), which allows us to provide original information on this question.
Study Strengths and Limitations
The VESPA study, thanks to its large, randomized sample of HIV-infected hospital outpatients from all over France, provides a unique data set for studying the social aspects of HIV infection in their diversity at the level of a country. The nonresponse rate was 41% of the patients randomized for the study, with higher rates of refusal among those employed, mostly attributed to a lack of time for answering the questionnaire. However, the information on employment status was collected both for respondents and nonrespondents, allowing for a weighting procedure to account for this participation bias. Thus, employment rates reported in this study are likely to be generalizable to the whole population of individuals living with HIV/AIDS and followed at hospital in France in 2002 to 2003 and to allow comparisons with data from the French general population.
Data on both HIV-infected individuals and the general population were collected between 2002 and 2003, a period over which labor market characteristics did not encounter major changes in France, which allowed appropriate comparisons between the 2 data sets. In Western countries, HIV infection preferentially reaches selected groups of the population with specific sociodemographic and behavioral characteristics that may themselves be associated with employment rate. Indeed, the frequency of drug use is particularly high among HIV-infected individuals (20% of the participants of the VESPA study were past or current injection drug users vs <1% in the French general population33). Moreover, non-French HIV-infected individuals were characterized by a recent date of immigration (median time since immigration at the time of HIV diagnosis was 1 year among immigrants in the VESPA study) and a high frequency of migration from regions of high HIV prevalence, especially sub-Saharan Africa (55% of the immigrants in the VESPA study were born in sub-Saharan Africa vs 9% in the French general population).19 However, results were similar when non–French citizens and HIV-infected injection drug users were excluded from the analyses, suggesting that our findings are not explained by these differences.
Our results show that, in France, the overall difference in employment rates between individuals living with HIV/AIDS in the HAART era and the general population persists after accounting for the sociodemographic and educational differences between these populations. Logically, the difference in employment rates with the general population appears to be more marked among patients whose HIV infection was diagnosed before 1994—i.e., those whose disease has had the time to progress before they could benefit from HAART. However, our results show that even among patients who have had access to effective therapies from the early times of their HIV infection, employment rate in 2003 was significantly lower than that in the general population.
Interpretation of the Results
Although the present study precludes from drawing any conclusion on a causal relationship between HIV infection and workforce participation, the persisting difference in employment rates we have shown is likely to reflect an independent influence of HIV infection on employment status. First, HIV infection may constitute a barrier to access (or return) to work for those who are unemployed: Studies have reported that although large proportions of unemployed HIV-infected individuals have contemplated work reentry as efficient treatments have emerged, few have actually done so.28,34–37 Moreover, HIV infection may constitute a cause of employment loss. The existence of a phenomenon of employment loss during HIV infection has been reported in several studies: Among the 319 patients followed in the French PRIMO prospective cohort from 1996, almost 1 in 5 employed patients (18%) had lost their job after a median time of 2.5 years since HIV infection.38 In a representative sample of HIV-infected patients in the United States, 6% of those who were employed had lost their job within the first 6 months following HAART initiation.27 Additionally, data on employment trajectory since HIV diagnosis collected retrospectively in the VESPA study indicate that 28% of the 647 patients who were diagnosed with HIV since 1996 and employed at the time of diagnosis had lost their job in 2003; HIV was reported to have played an important role in employment loss by 52% of them (data available on request).
Both low access (or return) to work and employment loss may result from the functional consequences of HIV infection. However, in the HAART era, the level of HIV-related physical disability is limited, suggesting that additional phenomena are likely to be involved. In particular, HIV-related discrimination from employers may impair individuals’ chances of both being recruited and maintaining employment. Stigma associated with HIV has been shown to be greater than for other chronic conditions such as hypertension, diabetes, or depression.39 Among those participants of the VESPA study who were employed in 2003, a large majority (70%) had kept their HIV status secret from their employer and colleagues, probably for fear of stigma, and only 6% reported that they had experienced HIV-related discrimination at their workplace. By comparison, this rate reached 13% among those who had lost their employment during the course of the disease (data available on request), which suggests that HIV-related discrimination may have played a role in these employment losses.
Moreover, we have found that the difference in employment rates between HIV-infected individuals and the general population is not homogeneous according to the socioeconomic position of the HIV-infected patients as defined by education level. Among highly educated patients diagnosed with HIV from 1994 onward, employment rate appears to be comparable to that observed in the general population of the same sociodemographic and educational level, suggesting that, in the HAART era, HIV infection does not impair employment among socially privileged individuals. Nonetheless, our results show marked differences in employment rates with the general population among those who have classically the most disadvantages with regard to work-force participation in France40—i.e., those with a low education level. As a result, inequalities regarding employment status are likely to be greater among HIV-infected individuals compared with the general population. This finding is consistent with studies that report a socially differentiated impact of HIV infection38 and various chronic conditions including rheumatoid arthritis,7,8 impaired cardiac function,12 and limiting long-standing illness13,14,41,42 on employment status.
Such inequalities may be related to various factors. First, these inequalities may be explained by a poorer health status—i.e., a more severe HIV infection or a higher co-morbidity among patients of the least advantaged social classes compared with those who are more privileged. Indeed, we have previously shown the existence of social inequalities in HIV-infected patients’ health status in France, despite equal access to care and treatment for the disease.21 However, a recent study has shown that among HIV-infected patients followed in the French PRIMO prospective cohort, employment loss occurred more frequently among those with adverse socioeconomic conditions regardless of markers of HIV severity and co-morbidity,38 suggesting that health status does not explain on its own the social inequalities in the consequences of HIV infection on employment. Second, because they have to face adverse working conditions (e.g., low control over work pace and scheduling, high level of physical demand) and work insecurity (nonpermanent employment) more often than others, subjects of the least advantaged social classes are likely to encounter more difficulties in maintaining work once they have to manage their chronic condition. Third, HIV-related stigma has been shown to strengthen the class inequalities that preexist in society,43 suggesting that patients who have the most disadvantaged social position may experience more workplace discrimination than the others. Lastly, in France, as in other countries, HIV-infected individuals may receive disability benefits in relation to their disease. For patients qualified only for insecure or casual jobs, workforce entry or reentry may jeopardize these benefits and, thus, the overall financial situation of those receiving them; such benefits may therefore act as a poverty trap among these patients.44 Further studies with longitudinal design and detailed data both on HIV-infected patients’ health status and living conditions (e.g., working conditions, discriminations, resources) are needed to discriminate among the possible mechanisms of such inequalities.
Public Health Implications
Our findings have important social and public health implications. First, because HIV infection mostly affects adults of prime working age, among whom a substantial and increasing proportion belong to socially vulnerable populations, the influence of HIV infection on employment suggested by our data is likely to translate to a high socioeconomic burden in France as well as in other Western countries. Thus, social interventions are needed to assist HIV-infected individuals in their access to employment or in their maintenance of work from the earliest times of the disease. Such interventions should include adjustment of working conditions for HIV-infected individuals in employment, actions of work incentive for those who are inactive, and the implementation of measures aimed at fighting HIV-related discrimination, especially at the workplace.
Second, our finding of an increased level of inequalities with regard to employment among individuals living with HIV compared with the general population is likely to have public health consequences. Indeed, given previous analyses that showed that unfavorable employment status was predictive of poor health status among HIV-infected patients,21 one can think that such an increase in the level of employment inequalities may result in increased social health disparities among individuals living with HIV compared with what occurs in the general population. Because social inequalities in health have been shown to be persistently marked among the general population of various Western countries,45 tackling the inequalities in the social consequences of HIV infection appears to be of importance. Thus, social interventions should focus preferentially on the most socially vulnerable populations. To design such interventions, further studies should provide a better understanding of the mechanisms of employment loss and should identify barriers to access or return to work during the course of chronic HIV infection.
Acknowledgments
The VESPA study was funded by the Agence Nationale de Recherche sur le Sida et les Hépatites Virales (ANRS-EN12-VESPA study). The French Labor Force Survey is funded by the Institut National de la Statistique et des Etudes Economiques.
We acknowledge all the patients and physicians who have participated in the VESPA study. Grateful thanks to Jean Bouyer for his methodological help relating to bootstrap procedures and to Archana Singh-Manoux for carefully reading the manuscript.
Human Participant Protection The study fulfilled the ethical requirements of the French Commission Nationale Informatique et Libertés.
Peer Reviewed
Contributors R. Dray-Spira, J. F. Ravaud, and F. Lert contributed to the study design. R. Dray-Spira and A. Gueguen performed data management and statistical analyses. All authors contributed to the interpretation of the results and the writing of the paper.
References
- 1.Greenwald HP, Dirks SJ, Borgatta EF, McCorkle R, Nevitt MC, Yelin EH. Work disability among cancer patients. Soc Sci Med. 1989;29:1253–1259. [DOI] [PubMed] [Google Scholar]
- 2.Bartley M, Sacker A, Clarke P. Employment status, employment conditions, and limiting illness: prospective evidence from the British household panel survey 1991–2001. J Epidemiol Community Health. 2004;58: 501–506. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Moser KA, Fox AJ, Jones DR. Unemployment and mortality in the OPCS Longitudinal Study. Lancet. 1984;2:1324–1329. [DOI] [PubMed] [Google Scholar]
- 4.Sorlie PD, Rogot E. Mortality by employment status in the National Longitudinal Mortality Study. Am J Epidemiol. 1990;132:983–992. [DOI] [PubMed] [Google Scholar]
- 5.Voss M, Nylen L, Floderus B, Diderichsen F, Terry PD. Unemployment and early cause-specific mortality: a study based on the Swedish twin registry. Am J Public Health. 2004;94:2155–2161. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Bartley M, Ferrie J, Montgomery SM. Living in a high-unemployment economy: understanding the health consequences. In: Marmot M, Wilkinson RG, eds. Social Determinants of Health. New York, NY: Oxford University Press; 1999.
- 7.Fex E, Larsson BM, Nived K, Eberhardt K. Effect of rheumatoid arthritis on work status and social and leisure time activities in patients followed 8 years from onset. J Rheumatol. 1998;25:44–50. [PubMed] [Google Scholar]
- 8.Sokka T. Work disability in early rheumatoid arthritis. Clin Exp Rheumatol. 2003;21(5 suppl 31): S71–S74. [PubMed] [Google Scholar]
- 9.Kraut A, Walld R, Tate R, Mustard C. Impact of diabetes on employment and income in Manitoba, Canada. Diabetes Care. 2001;24:64–68. [DOI] [PubMed] [Google Scholar]
- 10.Matsushima M, Tajima N, Agata T, Yokoyama J, Ikeda Y, Isogai Y. Social and economic impact on youth-onset diabetes in Japan. Diabetes Care. 1993;16: 824–827. [DOI] [PubMed] [Google Scholar]
- 11.Robinson N, Yateman NA, Protopapa LE, Bush L. Unemployment and diabetes. Diabet Med. 1989;6: 797–803. [DOI] [PubMed] [Google Scholar]
- 12.Nielsen FE, Sorensen HT, Skagen K. A prospective study found impaired left ventricular function predicted job retirement after acute myocardial infarction. J Clin Epidemiol. 2004;57:837–842. [DOI] [PubMed] [Google Scholar]
- 13.Lindholm C, Burstrom B, Diderichsen F. Class differences in the social consequences of illness? J Epidemiol Community Health. 2002;56:188–192. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.van de Mheen H, Stronks K, Schrijvers CT, Mackenbach JP. The influence of adult ill health on occupational class mobility and mobility out of and into employment in the The Netherlands. Soc Sci Med. 1999; 49:509–518. [DOI] [PubMed] [Google Scholar]
- 15.Ravaud JF, Mormiche P. Handicaps et incapacités [Handicap and disability]. In: Leclerc A, Fassin D, Grandjean H, Kaminski M, Lang T, eds. Les Inégalités Sociales de Santé [Social Health Inequalities]. Paris, France: La Découverte; 2000.
- 16.Hamers FF, Downs AM. The changing face of the HIV epidemic in western Europe: what are the implications for public health policies? Lancet. 2004;364: 83–94. [DOI] [PubMed] [Google Scholar]
- 17.Staehelin C, Egloff N, Rickenbach M, Kopp C, Furrer H, for the Swiss HIV Cohort Study. Migrants from sub-Saharan Africa in the Swiss HIV Cohort Study: a single center study of epidemiologic migration-specific and clinical features. AIDS Patient Care STDS. 2004;18:665–675. [DOI] [PubMed] [Google Scholar]
- 18.Stone VE. Optimizing the care of minority patients with HIV/AIDS. Clin Infect Dis. 2004;38: 400–404. [DOI] [PubMed] [Google Scholar]
- 19.Lert F, Obadia Y, et l’équipe de l’enquête VESPA [and the ANRS-VESPA survey team]. Comment vit-on en France avec le VIH/sida? [Living with HIV/AIDS in France]. Population et Sociétés. 2004;(406)1–5.
- 20.Young J, De Geest S, Spirig R, et al. Stable partnership and progression to AIDS or death in HIV infected patients receiving highly active antiretroviral therapy: Swiss HIV cohort study. BMJ. 2004;328:15. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Dray-Spira R, Gueguen A, Persoz A, et al. Temporary employment, absence of stable partnership, and risk of hospitalisation or death during the course of HIV infection. J Acquir Immune Defic Syndr. 2005;40: 190–197. [DOI] [PubMed] [Google Scholar]
- 22.Dray-Spira R, Lert F. Social health inequalities during the course of chronic HIV disease in the era of highly active antiretroviral therapy. AIDS. 2003;17: 283–290. [DOI] [PubMed] [Google Scholar]
- 23.Cunningham WE, Andersen RM, Katz MH, et al. The impact of competing subsistence needs and barriers on access to medical care for persons with human immunodeficiency virus receiving care in the United States. Med Care. 1999;37:1270–1281. [DOI] [PubMed] [Google Scholar]
- 24.Dray-Spira R, Lert F, Marimoutou C, Bouhnik AD, Obadia Y. Socioeconomic conditions, health status and employment among persons living with HIV/AIDS in France in 2001. AIDS Care. 2003;15:739–748. [DOI] [PubMed] [Google Scholar]
- 25.Ezzy D, de Visser R, Bartos M. Poverty, disease progression and employment among people living with HIV/AIDS in Australia. AIDS Care. 1999;11: 405–414. [DOI] [PubMed] [Google Scholar]
- 26.Fleishman JA. Transitions in insurance and employment among people with HIV infection. Inquiry. 1998;35:36–48. [PubMed] [Google Scholar]
- 27.Goldman DP, Bao Y. Effective HIV treatment and the employment of HIV(+) adults. Health Serv Res. 2004;39:1691–1712. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Rabkin JG, McElhiney M, Ferrando SJ, Van Gorp W, Lin SH. Predictors of employment of men with HIV/ AIDS: a longitudinal study. Psychosom Med. 2004;66: 72–78. [DOI] [PubMed] [Google Scholar]
- 29.Bourdillon F, Nadal J. Les Problèmes de Santé et les Besoins des Personnes Atteintes d’Infection à VIH: Enquête Hospitalière Multicentrique [Health problems and needs of HIV-infected persons: multicentric hospital survey]. Paris, France: Ministère de l’Emploi et de la Solidarité, Direction des Hôpitaux - Mission Sida; 1996.
- 30.Peretti-Watel P, Riandey B, Dray-Spira R, Bouhnik AD, Obadia Y. Comment enquêter la population séropositive en France?: l’enquête ANRS-EN12-VESPA 2003 [Surveying the HIV-positive population in France. The ANRS-EN12-VESPA Survey.]. Population. 2005;60:525–550. [Google Scholar]
- 31.Deville J-C, Särndal C-E. Calibration estimation in survey sampling. J Am Stat Assoc. 1992;87:375–382. [Google Scholar]
- 32.Eurostat. The European Union Labour Force Survey—Methods and Definitions 2001. Luxembourg: European Communities; 2003.
- 33.Drugs and Dependencies, Essential Data [in French]. Paris, France: Observatoire Français des drogues et des toxicomanies; 2005.
- 34.Brooks RA, Martin DJ, Ortiz DJ, Veniegas RC. Perceived barriers to employment among persons living with HIV/AIDS. AIDS Care. 2004;16:756–766. [DOI] [PubMed] [Google Scholar]
- 35.Ferrier SE, Lavis JN. With health comes work? People living with HIV/AIDS consider returning to work. AIDS Care. 2003;15:423–435. [DOI] [PubMed] [Google Scholar]
- 36.Martin DJ, Brooks RA, Ortiz DJ, Veniegas RC. Perceived employment barriers and their relation to workforce-entry intent among people with HIV/AIDS. J Occup Health Psychol. 2003;8:181–194. [DOI] [PubMed] [Google Scholar]
- 37.Lem M, Moore D, Marion S, et al. Back to work: correlates of employment among persons receiving highly active antiretroviral therapy. AIDS Care. 2005; 17:740–746. [DOI] [PubMed] [Google Scholar]
- 38.Dray-Spira R, Persoz A, Boufassa F, et al. Employment loss following HIV infection in the era of highly active antiretroviral therapies. Eur J Public Health. 2006;16:89–95. [DOI] [PubMed] [Google Scholar]
- 39.Roeloffs C, Sherbourne C, Unutzer J, Fink A, Tang L, Wells KB. Stigma and depression among primary care patients. Gen Hosp Psychiatry. 2003;25: 311–315. [DOI] [PubMed] [Google Scholar]
- 40.Données Sociales—La Société Française [Social data—The French Society]. Paris, France: Institut National de la Statistique et des Etudes Economiques; 2002.
- 41.Bartley M, Owen C. Relation between socioeconomic status, employment, and health during economic change, 1973–93. BMJ. 1996;313:445–449. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Burstrom B, Whitehead M, Lindholm C, Diderichsen F. Inequality in the social consequences of illness: how well do people with long-term illness fare in the British and Swedish labor markets? Int J Health Serv. 2000;30:435–451. [DOI] [PubMed] [Google Scholar]
- 43.Parker R, Aggleton P. HIV and AIDS-related stigma and discrimination: a conceptual framework and implications for action. Soc Sci Med. 2003;57:13–24. [DOI] [PubMed] [Google Scholar]
- 44.Voelker R. Protease inhibitors bring new social, clinical uncertainties to HIV care. JAMA. 1997;277: 1182, 1184. [DOI] [PubMed] [Google Scholar]
- 45.Kunst AE, Mackenbach JP. The size of mortality differences associated with educational level in nine industrialized countries. Am J Public Health. 1994;84: 932–937. [DOI] [PMC free article] [PubMed] [Google Scholar]