

Abstract
There is increasing evidence that obesity and overweight may be related, in part, to adverse work conditions. In particular, the risk of obesity may increase in high-demand, low-control work environments, and for those who work long hours. In addition, obesity may modify the risk for vibration-induced injury and certain occupational musculoskeletal disorders.
We hypothesized that obesity may also be a co–risk factor for the development of occupational asthma and cardiovascular disease that and it may modify the worker’s response to occupational stress, immune response to chemical exposures, and risk of disease from occupational neurotoxins. We developed 5 conceptual models of the interrelationship of work, obesity, and occupational safety and health and highlighted the ethical, legal, and social issues related to fuller consideration of obesity’s role in occupational health and safety.
Workplace hazards continue to exact a large toll on society in terms of morbidity, mortality, and financial and social costs, which provides justification for the ongoing national commitment to the protection of the health of the workforce.1–4 At the same time, obesity and overweight are increasingly becoming the focus of public health concern.5–11 Nearly two thirds of US adults have a body mass index (BMI) higher than 25 kg/m2 and are classified as overweight.7 Obesity, defined as a BMI greater than 30 kg/m2, is considered to be a national public health crisis.7,8 Both obesity and occupational morbidity and mortality are global problems as well.6,9,10
Employed adults spend a quarter of their lives at work, and the pressure and demands of work may affect their eating habits and activity patterns, which may lead to overweight and obesity.12–17 These same pressures and other factors at work (such as exposures to harmful agents, physical forces, and psychosocial stress and strain) can also lead to occupational injury and illness. Obesity may affect both work opportunity and performance as well as modify the relationship between work-place exposure and health outcome. The nature of many of these interactions is not well studied or understood. Should the obesity–work relationship be a priority when one is planning for occupational safety and health research? Moreover, should workers’ obesity be given any more consideration than other modifiable risk factors such as smoking, blood pressure, blood glucose levels, alcohol use, and medication levels when one is addressing workplace issues? Is there any particular advantage to intervention in the workplace to affect the prevalence of obesity? We examined the nexus of obesity, work, and occupational disease and injury; identified information gaps and potential research leads; and highlighted ethical, legal, and social issues related to the intersection of these topics.
In some instances, obesity and workplace risks (e.g., organizational factors and hazardous exposures) may be related, and obesity may represent an additional risk factor for particular diseases that result from workplace exposures. Better understanding of relationships between obesity and work may encourage identification of interventions to address both obesity and workplace disease and injury. Historically, these 2 areas have been considered separate domains. Obesity arises from complex social and biological phenomena, but is often perceived as the result of an individual’s behaviors. By contrast, occupational disease and injury prevention is primarily the responsibility of the employer. Strategies to combine protection from occupational risk with programs to encourage individual change to diminish health risk from obesity warrant consideration. Poorly done, such efforts may result in the individual workers being blamed for their obesity and may distract from the workplace contribution to injury or illness. Even if this shift does not occur, there is concern that scarce resources for reduction of risk from workplace hazards will be diluted or decreased by the focus on obesity in workers. Moreover, such attention to the individual’s behavior may shift focus from the more important social, cultural, and environmental causes of, and interventions for, obesity.11,18–20
The following 4 sections focus on the relationships between work, work conditions and exposures, and obesity.
ASSOCIATION OF WORK AND WORK CONDITIONS WITH OBESITY AND BODY WEIGHT
Little research has examined the effects of occupational status and work conditions (including organizational factors) on BMI. BMI is assumed to represent the degree of body fat, but other measures may be better. Nonetheless, BMI has been widely used in studies of the impact of work on obesity.21
Twelve studies (mostly cross-sectional) were identified that have used some measure of job stress to test for associations with BMI.22–33 The demand–control model was used in 8 of these studies,22,24,26,28–31,33 and other measures of job stress were used in the remaining 4 studies, although none of these included the effort–reward imbalance model.34
Four of the studies with the demand–control model (high demands and low control) showed a positive statistically significant relationship with BMI,24,28–30 but the remaining 4 showed no association.22,26,31,33 Two of the remaining 4 studies that used other measures of job strain showed positive and statistically significant relationships with BMI.23,32 These studies did not fully control for physical activity, long hours spent at work, or shift work (all variables that have been associated with obesity in other studies).30
The relationship of nonpsychosocial work conditions to BMI has also been investigated. Using data from the National Population Health Survey in Canada, Shields demonstrated that, after statistical adjustment, men who worked more than 35 hours a week had an odds ratio of 1.4 for being overweight (BMI>25 kg/m2).35 Long hours of work were not associated with overweight in women. Additionally, increased body weight has been reported among shift workers in developed countries,12–16,36 and shift work has been associated with BMI among Dutch men and women36 and among middle-aged Swedish women.32
In a large, population-based Finnish cohort, unemployment was positively associated with BMI for men and women although the association was particularly strong for women with long histories of unemployment.37 Unemployment was also associated with greater BMI among a cohort of Swedish women.32 In a cohort of 14799 Australian women aged 18 to 23 years, overweight and obesity were associated with unemployed status and low occupational and educational status.30 In addition, increased body weight has been reported over a 12-year period among shift workers in developed countries.12–16,36
Yamada et al. hypothesized 3 ways that work could facilitate weight gain17: (1) job stress could impact behaviors such as alcohol consumption and sedentary leisure activities that are related to weight gain, (2) psychological strain could lead to modification of endocrine factors related to weight gain, and (3) long work hours, shift work, and overtime could result in fatigue and inhibit behaviors that prevent weight gain and abdominal fat accumulation.
ASSOCIATION OF OBESITY WITH WORK PERFORMANCE AND HEALTH CARE COSTS
Obesity appears to have a significant positive association with absenteeism (measured as work loss days).38–41 Body fat distribution has been found to be associated with high annual sick leave incidence and long spells of absence in a Belgian workforce.42 In a banking company, workers with high BMI had additional health risks, short-term absences because of disability and illness, and higher health care costs than workers who were not overweight (no elevated BMI).43 Obese workers were found to be 1.7-times more likely to experience a high level of absenteeism (defined as 7 or more absences because of illness during the past 6 months) and were 1.6-times more likely to report moderate absenteeism (3 to 6 absences because of illness during the past 6 months).44 Burton and Conti reported that obese workers also tended to incur greater productivity losses than nonobese workers.45
Other studies have shown that a worker’s BMI classification predicts assignment to high health care cost and high-absence groups.39,46,47 The Insurance Information Institute anticipated higher costs for overweight workers:
Because overweight and obese people suffer from a higher incidence of chronic disease, including musculoskeletal disorders, recovery from any given injury or illness—including those that occur in the workplace or as a result of occupational exposures—is likely to be more difficult and more expensive than for normal-weight individuals.48
In one analysis, obesity was shown to be associated with higher health care costs than were smoking, drinking, and poverty.49,50 It is important, however, to realize that there is not a simple causal link between obesity and those characteristics. Rather, the relationships are complex and not easily explained.
POTENTIAL IMPACT OF OBESITY ON WORK-RELATED DISEASE
Few studies have examined the role of obesity or excess body weight in the modification of risk of occupational diseases and conditions. Henschel reviewed the role of obesity in alteration of the intensity of response to the following 7 occupational hazards—heat exhaustion and heat stroke in hot environments, physiological strain during performance of hard physical work, respiratory strain and disorders during hard physical work, accidents involving equipment operators and other duties, decompression sickness, high altitude tolerance, and pesticide exposures—and concluded that obesity should be considered a significant occupational hazard.51 However, the cited literature in that paper was quite limited.
Evidence of varying strength suggests that obesity increases the risk of certain occupational diseases or conditions such as musculoskeletal disorders, cardiovascular disease, asthma, and vibration-induced injury. Obesity may also modify physiological responses to neurotoxins and immune responses to chemical challenges, many of which are found at work. Obesity may interact with occupational stress. The effectiveness or availability of personal protective equipment may be limited for obese workers. Also, although the role intake plays in the risk of certain cancers is generally well documented in animals, it is not known the extent to which an interaction occurs with occupational cancers. In the following subsections we review what is known about the effects of obesity or excessive body weight on various occupational diseases or conditions. We also offer hypotheses about potential interactions.
Vibration-Induced Injury
In the United States, approximately 1.5 million workers perform tasks in which they are exposed to upper-limb vibration. Depending on their occupation, 6% to 95% (average, 46%) of the workers exposed to upper-limb vibration will develop hand–arm vibration syndrome (HAVS).52 This syndrome can be characterized by vasospasms of the peripheral vasculature that result in blanching of the digits (white finger), reductions in thermal and tactile sensitivity, upper-limb weakness, pain, and reductions in fine-motor coordination.53
Occupational factors such as exposure duration and amplitude of the vibration exposure serve as risk factors for developing HAVS.54 In addition, a number of personal health factors such as hypertension and diabetes are correlated with the presence of HAVS-related symptoms.52 Epidemiological studies that assess body mass demonstrate that the incidence of obesity and diabetes is increased in people with HAVS and other upper-limb musculoskeletal disorders.55–57 Damage resulting from obesity or obesity-related changes in physiology may compromise muscular, neural, and vascular tissues, making them more susceptible to vibration-induced injury.
Work-Related Asthma
Asthma occurs in 10% to 15% of the adult population and is more common in industrialized settings; it has been estimated that up to 15% of all cases are associated with work-place exposure.58,59 No studies have addressed obesity as a risk factor in the development of work-related asthma; however, substantial attention has been devoted to obesity as a risk factor for asthma because of the observation of dyspnea in obese individuals.60–62 In general, excess fat tissue impairs ventilatory functions, although this is thought to be relatively mild except in cases of severe obesity.63
Cross-sectional and prospective cohort studies have shown associations between obesity and asthma in children64 and in women.65 Associations between obesity and asthma in men are less clear; several prospective studies showed a limited association or showed a stronger association in women than in men.61,66 However, a recent study indicated that although women show a monotonic association between asthma and BMI, men show a U-shaped relationship, indicating that both extremes of weight are associated with a higher prevalence of asthma.67 Animal studies are more limited. One study68 indicated that immune mediators involved in asthma in mice are modulated in mice fed high-fat diets. In other studies, ozone-induced airway responses were increased in obese mice compared with controls.69
Chemical Immunomodulation
No reported epidemiological studies have specifically indicated that obesity is a risk factor for microbial infections in adults, but several studies show increased infections in obese adolescents, which suggests that the immune system is affected by obesity.70,71 Evidence also indicates that wound healing is adversely affected in obese adults.72 Bhati et al. concluded from their studies that obesity, uncontrolled diabetes mellitus, and female gender are associated with higher infection rates.73 Chemical exposure in the workplace may lead to altered immune function, including both allergy and immune suppression. Immune suppression can lead to increased susceptibility to infectious agents.74
Laboratory experiments support the biological plausibility of this relationship. Most experimental studies of the effects of obesity on the immune system have focused on the use of ob/ob leptin-deficient animal models.75,76 These animals show pleiotrophic effects on a number of systems in the body, including altered states of immunity. Leptin-deficient mice demonstrate thymus atrophy with the thymic cortex being particularly sensitive. As leptin plays a role in protecting CD4+CD8+ cells from glucocorticoid-induced apoptosis, it may play an important role in chemical-induced immune suppression. Likewise, leptin may play a significant role in the development of allergy and the balance between Th1 and Th2 responses. Increased levels of leptin have been shown to support a Th1 response leading to T cell–mediated disease, whereas low leptin levels are more supportive of Th2 responses, increased levels of interleukin 4, and potentially immunoglobulin E–mediated disease. Obesity in workers that is not related to mutation of the ob gene may be correlated with increased levels of leptin.75–78
Musculoskeletal Disorders
Musculoskeletal disorders are defined as structural damage, inflammation, or pain that results from injuries to nerves, tendons, muscles, blood vessels, or other supportive tissues associated with the musculoskeletal system.79 Certain workplace exposures are correlated with an increased risk for acquiring a work-related musculoskeletal disorders. These include exposures to repetitive movements, excessive loading, muscle overuse, and vibration. A worker’s health status may also affect the risk of acquiring a work-related musculoskeletal disorder. Only a few epidemiological studies have explicitly studied the joint effects of work, obesity, and musculoskeletal disorders. Various musculoskeletal disorders such as carpal tunnel syndrome and osteoarthritis have been associated with increased BMI or obesity in studies that control for work and nonwork risk factors.80–84 Obesity is also associated with type 2 diabetes. This condition has been linked to physiological changes in the cardiovascular, nervous, and skeletal muscle systems. It could be hypothesized that the pathophysiological parameters associated with obesity will increase the risk of acquiring a musculoskeletal disorder and impair the recovery mechanisms.
Neurotoxicity
Although no epidemiological studies have investigated the risk of neurotoxicity in workers as a function of BMI, recent studies provide evidence to show that low calorie intake decreases the risk of Parkinson’s disease85 and Alzheimer’s disease,86 whereas increased midlife adiposity serves as a risk factor for developing Parkinson’s disease.87 Together, these data suggest that the nervous system, like other organ systems, is vulnerable to the adverse consequences of obesity. Indeed, over the past decade, anecdotal and experimental data obtained with animals often suggest that rats and mice with increased body mass show exaggerated neurotoxic responses to diverse classes of known neurotoxic chemicals (e.g., organometals, substituted pyridines, substituted amphetamines).88 Thus, given the linkage between obesity and factors known or suspected to damage the nervous system, it could be hypothesized that obesity may enhance the susceptibility of the nervous system to toxic chemicals found in the work environment.
Stress and Stress Responses
Although there is great interest in understanding the interactions between stress and obesity, most research has focused on the role of stress in weight gain and the determination of whether stress controls where fat is deposited. Occupational studies reviewed earlier support the hypothesis that job stress (from, for example, a low-control and high-demand work environment) is associated with high BMI. Stress alters food choices in humans and shifts it toward energy-dense items that contain saturated fat and sugar.89 Chronic stress results in deposition of intraabdominal (rather than subcutaneous) fat in humans, nonhuman primates, and rodents.90 Although intraabdominal fat is considered to be more detrimental to health, information is limited as to how fat deposition patterns affect the biological consequences of stress; however, in humans it has been demonstrated that a greater stress response is found when fat is intraabdominal, even when the person is lean.91 Intraabdominal stores of fat appear to cause a greater stress response, including the release of glucocorticoids and other stress chemicals. The impact of this heightened activation for brain health is relatively unexplored. However, excess stress is considered to be detrimental to brain health and is associated with conditions such as depression. Furthermore, magnetic resonance imaging studies of the human brain suggest that excessive exposure to stress chemicals such as cortisol in Cushing disease or to extremely traumatic events is associated with shrinkage of brain areas important for cognition.92
Experimental work indicates that stress is linked to maladaptive remodeling of the brain, including atrophy of neurons and shrinkage of the areas and elements of the neuron responsible for communication. Remodeling is believed to play a role in links between stress and diseases such as addiction and dementia.93 Aberrant remodeling is also hypothesized to play a role in depression. It is also known that chemicals associated with the stress response (e.g., glucocorticoids, catecholamines) compromise the activation of pathways responsible for maintaining the structure and function of these same cellular elements. It is not known whether the brain of the obese or overweight person is more susceptible to the impact of stress. An important research question is whether obesity (especially intraabdominal deposition of fat) increases the susceptibility of the brain to stress-induced remodeling. It could be hypothesized that obese persons, especially those with intraabdominal fat, will show elevated stress signaling in the brain and will be more susceptible to stress-induced brain remodeling.
Cardiovascular Disease
The interplay between psychosocial stress at work and cardiovascular disease has been investigated.34,94,95 Despite various methodological issues, several reviewers and investigators have supported the hypothesis that the psychosocial aspects of work are related to the risk of developing cardiovascular disease.34,96 Obesity also is a known risk factor for cardiovascular disease, and the question is whether obesity modifies the association between workplace stress and cardiovascular disease.
Another hypothesis of cardiovascular disease development involves occupational risk factors (including carbon disulfide, arsenic, ultrafine dusts, or fumes) that modify atherosclerosis progression through induction of vascular oxidative and inflammatory effects.97–100 Adipose tissue mass, especially visceral fat, in addition to the endocrine and metabolic dysfunction, is also linked with increased production of proinflammatory mediators.101 Thus, inflammatory responses mediated by obesity and occupational exposure to chemicals or dusts may interact synergistically to increase the risk of atherosclerosis-related cardiovascular diseases.
Cancer
Energy restriction has long been known to impact the development of various cancers in animals that were administered chemical carcinogens.102–104 However, no studies have been specifically identified that explore the relationship of BMI to the development of work-related cancers in occupational cohorts. Despite associations of high energy intake with various cancers such as breast, colon, rectum, kidney, thyroid, and prostate, the more traditional occupational cancers such as lung and bladder cancer were found to be inversely associated with body weight. However, these analyses did not generally account for cigarette smoking or competing causes of death.103
Occupational Safety
Limited research has been done on the impact of obesity on worker safety. A few studies of work-related injuries have identified notable characteristics among injured workers, including increased BMI.105–108 Sleep-disordered breathing and obesity have been found to be risk factors in traffic accidents among commercial long-haul truck drivers.109 Various other transportation studies (particularly those that focused on seat belt use) have included BMI as a potential risk factor; however, the studies did not specifically address workers.110–112
Utility of Personal Protective Equipment
Although anthropometric characteristics have been shown to vary among occupations and should be considered in designing personal protective equipment, little information exists on the impact of obesity on personal protective equipment effectiveness or availability.113 Human physiological variables, including body weight, can affect respiratory performance during respirator tests and use.114 Body weight has also been a variable in research on fall protection, impact restraints,115 and the effectiveness of protective clothing.115,116 Because obesity has been shown to be a risk factor for soldiers training in hot and humid environments, it may also be assumed that this result pertains to workers, especially workers in protective equipment.117,118
CONCEPTUAL MODELS OF INTERRELATIONSHIPS OF WORK, OBESITY, AND DISEASE
On the basis of the literature described, it is possible to suggest various ways to view the interrelationship of work, obesity, and disease. Some are shown in testable conceptual models pictured in Figure 1 ▶. Although the models focus primarily on these 3 elements, each is subject to various cultural and social influences. Work is also depicted as a risk factor because of its organization or nature and because of exposures that might occur during work.
FIGURE 1—
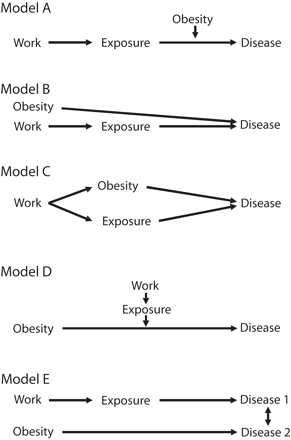
Models of the interrelationships of work, obesity, and disease
Note. Adapted from Ottman.119
In model A, a workplace exposure leads to an occupational disease. This relationship may be modified by obesity or weight gain, so that the risk will be greater (or lesser) in the obese workers. Model B depicts 2 independent and possibly additive pathways to disease. Obesity may serve as an independent risk factor in one pathway, and workplace exposure in another. Model C shows a combination of models A and B, with work as the source of adverse environmental exposures as well as a contributor to obesity and the combination or each factor independently resulting in modified disease risk. Model D illustrates that workplace exposure may be an effect modifier of an obesity–disease relationship. Model E illustrates how obesity may cause a particular disease and workplace exposure may cause another disease and there may be some interaction between the 2 diseases. That is, having 1 disease may put a worker at increased risk of the other. These models are presented for heuristic purposes, but they still require testing and validation. Additional modification of these models could occur as preliminary data are corroborated with regard to the hypothesis that in utero or neonatal exposures to environmental chemicals (notably endocrine disruptors) play a role in the etiology of obesity.120
INTERVENTION
If work, obesity, and occupational health and safety are considered to have some relationship, it may be useful to consider interventions that address them simultaneously. Some evidence exists that workers adhere better to health promotion guidance in a work-place setting when it addresses both workplace and personal risk factors, rather than just personal risk factors.121–124 Within the workplace, there is an opportunity to focus on interventions that realistically address the work organization and environmental factors that increase the risk for obesity.125–126
However, there is a need for further work on strategies that merge traditional workplace health protection with workplace health promotion that relates to weight gain and obesity.123 This logically includes a focus both on the work environment and on individual options, choices, and behaviors. It is also useful to emphasize the role employers and workers could play in advocacy of not only social policy changes that affect workplace hazards, but also those that treat weight control as a national priority supported by environmental, economic, and social initiatives.49,128
ETHICAL, LEGAL, AND SOCIAL ISSUES
To protect all workers, employers are responsible for providing workplaces that are free of recognized hazards. To the extent that obesity increases the risk of adverse health effects from certain occupational exposures, decisionmakers may have to consider strategies for effective protection of these more vulnerable workers. A major challenge will be to determine how to consider health consequences of obesity without using approaches that are prejudicial, discriminatory, stigmatizing, or punitive. Work-related areas where such considerations are likely to arise include worker privacy and autonomy, employment discrimination, risk communication, and workers’ compensation and tort liability.
Worker Privacy and Autonomy
Although work may convey other benefits, most people work to provide economically for themselves and their families and to obtain access to other work-associated benefits such as health insurance. People do not generally work to have their behavior changed or their health improved. As a result of the Health Insurance Portability and Accountability Act of 1996, workers have a reasonable expectation for personal privacy with regard to health information. This privacy expectation is reinforced by certain legal protections, especially with regard to confidentiality of health-related information. Work-based programs that focus on individual behaviors may be perceived accurately as intrusive and insensitive to the privacy and autonomy expectations of workers. Obesity is a particularly sensitive personal issue, and workers may be appropriately resistant to interventions that appear to single out obese persons. Alternatively, these issues may be addressed by worksite interventions that benefit all workers, for example, by diversifying food choices in cafeterias and in snack and soda machines, increasing opportunities for exercise, or reducing work-related stress for all workers.129
Employment Discrimination
Extensive evidence exists that shows bias against and stigmatization of overweight persons.130–136 This may lead to discrimination in employment practices that result in limited job choices and lower wages. Thus far, Michigan is the only state that prohibits employment discrimination on the basis of weight.137 Various misconceptions may lead to discriminatory action. For example, there is the possibility that findings of associations between obesity and work attendance such as described earlier in this article may be taken as causal when that has not been established or when other uncontrollable risk factors, such as age and genetics, confound the association.138–139
One major concern is that attention to obesity in workers will devolve to “blaming the victim.” That is, only a worker’s behavior and attributes may be considered factors for intervention. This approach negates the knowledge that obesity is affected by environmental and organizational as well as genetic, societal, cultural, and economic factors. Obesity may be a bona fide consideration in job placement after a hiring decision is made (as are other health-related considerations), but it generally should not be a determinant in the hiring decision itself.
Whether obesity should be considered a disease, a disability, or a lifestyle condition will influence how it is treated in the work-place.138 No consistent record indicates whether obesity is considered a disability under the Americans With Disabilities Act.139 Similarly, the Centers for Medicaid and Medicare Services (formerly the Health Care Financing Administration) historically did not consider obesity an illness and did not make payments for obesity treatments, except in some cases when obesity was a consequence of another disease or was a direct cause of another serious condition.140 However, a ruling in 2004141 removed the language that “obesity itself cannot be considered an illness.” This step allows members of the public to request a review of their own medical evidence to determine whether treatments related to obesity would be covered by Medicare.
In addition, the Social Security Administration provides disability benefits for people who meet requirements and requires claim adjudicators to examine the effect of obesity on the ability to do basic work.142 Increased awareness of the health consequences of obesity may prompt some employers to consider obesity and weight gain when dealing with insurance, hiring, placement, and promotion, regardless of whether obesity is a disease or disability. Data on increased absenteeism, illness, mortality, and cost of obese workers are likely to be part of this consideration.40,43,143,144 Future research that identifies obesity as an effect modifier of occupational exposure–disease associations may be included in employer decisionmaking, raising significant social, ethical, and potential legal issues about how society deals with the concept of susceptibility.
Risk Communication
Sound scientific information that relates to modifiers of health risk from occupational exposures has been the focus of risk communication. For example, construction workers who smoked and were exposed to asbestos at work have been informed about the health risks of both hazards and the added risk to workers exposed to both.145,146 When sufficient information exists to include consideration of the role of obesity in worksite health communication, such communications will need to be fact-based and directed toward reinforcement of proven health-protective strategies. Because obesity can be a consequence of workplace exposures, an effect modifier, an independent risk factor, a cofactor, or a confounding factor, communications will need to be circumstance-specific and based on the best-available information. Group risk communication may have a different focus than individual risk communication. For the group, population concepts such as prevalence and variability might predominate. For the individual worker, clinical interpretation and individual risk are important.
In ordinary language, “obesity” may be considered a pejorative term despite the intention in its use. Furthermore, many obese persons may not recognize themselves as such. Moreover, a person’s overweight status does not automatically imply ill health.147 The range of opinions and perceptions about the relationship of obesity to personal responsibility, genetic determinism, and environmental pressures should be considered in risk communications.
If obesity is known to modify the effect of an occupational exposure, how should an employer portray the risks without inappropriately shifting responsibility to the worker? To answer this question, it may be useful to consider how employers and workers have handled other personal factors (such as smoking) that are known to modify occupational exposures (such as to asbestos).122
Workers’ Compensation and Tort Liability
Workers’ compensation is supposed to provide partial or complete wage replacement and health care payments for people who experience a disease or injury caused by (or, in some instances, significantly exacerbated by) workplace exposures and conditions. Efforts have grown to limit the costs of workers’ compensation benefits provision in many jurisdictions. In some compensation systems, there are requirements to “apportion” the cause of a disease or injury among various work-related and nonwork factors and to compensate only for work-related causes.148 However, the ability to accurately determine the extent to which a worker’s disability pertains to work or nonwork factors is not a precise science. To the extent that effect modifiers such as obesity or genetic factors are involved, apportionment of causation to work-related factors may be reduced. The issue is further complicated by the fact that state workers’ compensation laws vary in terms of designation of obesity as an underlying medical condition related to specific injuries and illnesses.
CONCLUSIONS
Work and obesity both contribute to population morbidity and mortality as well as to attendant health care and societal costs, but each exists in a separate domain. Employers have traditionally been responsible for the prevention of work-related morbidity and mortality, but workers have been held responsible for the prevention of overweight and obesity. The 2 risks are likely to be interrelated, but the extent, nature, and temporality of these relationships have not been well studied. Research is warranted to explore how the work environment and work practices promote or discourage the development of obesity (and overweight in general) and to define the extent to which obesity acts to modify the risk of occupational diseases and injuries. This research can serve as the basis to determine the extent to which resources should be committed to this area and whether worksite alterations and programs are needed to reduce exposures or risks. In the meantime, it may be useful to consider selective strategies that address both work-related risk factors and obesity together. Such strategies will have to be sensitive to issues of language, prejudice, inappropriate apportionment of causality, and the various perceptions of employers and workers. Occupational morbidity and mortality and obesity are important, highly prevalent national problems. If it is more efficient to consider them together, the use of resources and health outcomes may improve.
Acknowledgments
The authors appreciate the comments of William Dietz, Joseph Fortuna, Sheldon Samuels, Ronald Goetzel, Paul Suadicani, and Neil Rowland on earlier drafts.
Human Participant Protection No human participants were involved in this study.
Peer Reviewed
Note. The findings and conclusions expressed in this paper are those of the authors and do not necessarily represent the views of the National Institute for Occupational Safety and Health.
Contributions P.A. Schulte originated the report, wrote the first draft except for the sections mentioned below, and coordinated its implementation. D.B. Miller coordinated the sections on the impact of obesity on work-related diseases with the following authors who wrote the first draft of the specific sections: K.M. Krajnak, vibration-induced injury; M. Luster, work-related asthma; A.E. Munson, chemical immunomodulation; R.G. Cutlip, musculoskeletal disorders; J.P. O’Callaghan, neurotoxicity; D.B. Miller, stress and stress responses; P.P. Simeonova, cardiovascular diseases; P.A. Schulte, cancer, occupational safety, and personal protective equipment. A. Ostry wrote the section on the impact of work and work conditions on obesity and body weight. G.R. Wagner helped organize and revise the article. L.A. Blanciforti and C.G. Parks provided input into the initial conceptualization, development, and editing.
References
- 1.Steenland K, Burnett C, Lalich N, Ward E, Hurrell J. Dying for work: the magnitude of US mortality from selected causes of death associated with occupation. Am J Ind Med. 2003;43:461–482. [DOI] [PubMed] [Google Scholar]
- 2.Schulte PA. Characterizing the burden of occupational injury and disease. J Occup Environ Med. 2005; 47:607–622. [DOI] [PubMed] [Google Scholar]
- 3.Leigh J, Markowitz S, Fahs M, Landrigan P. Costs of Occupational Injuries and Illnesses. Ann Arbor, Mich: University of Michigan Press; 2000.
- 4.Worker Health Chart Book 2004. Cincinnati, Ohio: National Institute for Occupational Safety and Health, Centers for Disease Control and Prevention. NIOSH publication 2004–146.
- 5.Kuczmarski RJ, Flegal KM. Criteria for definition of overweight in transition: background and recommendations for the United States. Am J Clin Nutr. 2000;72:1074–1081. [DOI] [PubMed] [Google Scholar]
- 6.Obesity: Preventing and Managing the Global Epidemic. Geneva, Switzerland: World Health Organization; 1998.
- 7.Flegal KM, Carroll MD, Ogden CL, Johnson CL. Prevalence and trends in obesity among US adults, 1999–2000. JAMA. 2002;288:1723–1727. [DOI] [PubMed] [Google Scholar]
- 8.Mokdad AH, Serdula MK, Dietz WH, Bowman BA, Marks JS, Koplan JP. The continuing epidemic of obesity in the United States. JAMA. 2000;284: 1650–1651. [DOI] [PubMed] [Google Scholar]
- 9.Visscher TL, Seidell JC. The public health impact of obesity. Annu Rev Public Health. 2001;22: 355–375. [DOI] [PubMed] [Google Scholar]
- 10.World Health Report 2002: Reducing Risk, Promoting Healthy Life. Geneva, Switzerland: World Health Organization; 2002.
- 11.Drewnowski A, Specter SE. Poverty and obesity: the role of energy density and energy costs. Am J Clin Nutr. 2004;79:6–16. [DOI] [PubMed] [Google Scholar]
- 12.Yamada Y, Kameda M, Noborisaka Y, Suzuki H, Honda M, Yamada S. Excessive fatigue and weight gain among cleanroom workers after changing from an 8-hour to a 12-hour shift. Scand J Work Environ Health. 2001;27:318–326. [DOI] [PubMed] [Google Scholar]
- 13.Niedhammer I, Lert F, Marne MJ. Prevalence of overweight and weight gain in relation to night work in a nurses’ cohort. Int J Obes Relat Metab Disord. 1996; 20:625–633. [PubMed] [Google Scholar]
- 14.Geliebter A, Gluck ME, Tanowitz M, Aronoff NJ, Zammit GK. Work-shift period and weight change. Nutrition. 2000;16:27–29. [DOI] [PubMed] [Google Scholar]
- 15.Knutsson A, Akerstedt T. The healthy-worker effect: self-selection among Swedish shift workers. Work Stress. 1992;6:163–167. [Google Scholar]
- 16.Di Lorenzo L, De Pergola G, Zocchetti C, et al. Effect of shift work on body mass index: results of a study performed in 319 glucose-tolerant men working in a Southern Italian industry. Int J Obes Relat Metab Disord. 2003;27:1353–1358. [DOI] [PubMed] [Google Scholar]
- 17.Yamada Y, Ishizaki M, Tsuritani I. Prevention of weight gain and obesity in occupational populations: a new target of health promotion services at worksites. J Occup Health. 2002;44:373–384. [Google Scholar]
- 18.Hill JO, Wyatt HR, Reed GW, Peters JC. Obesity and the environment: where do we go from here? Science. 2003;299:853–855. [DOI] [PubMed] [Google Scholar]
- 19.Hayne CL, Moran PA, Ford MM. Regulating environments to reduce obesity. J Public Health Policy. 2004;25:391–407. [DOI] [PubMed] [Google Scholar]
- 20.Egger G, Swinburn B, Rosner S. Dusting off the epidemiological triad: could it work with obesity? Obes Rev. 2003;4:115–119. [DOI] [PubMed] [Google Scholar]
- 21.Snijder MB, van Dam RM, Visser M, Seidell JC. What aspects of body fat are particularly hazardous and how do we measure them ? Int J Epidemiol. 2006; 35:83–92. [DOI] [PubMed] [Google Scholar]
- 22.Brisson C, Larocque B, Moisan J, Vezina M, Dagenais GR. Psychosocial factors at work, smoking, sedentary behavior, and body mass index: a prevalence study among 6995 white collar workers. J Occup Environ Med. 2000;42:40–46. [DOI] [PubMed] [Google Scholar]
- 23.Georges E, Wear M, Mueller W. Body fat distribution and job stress in Mexican-American men of the Hispanic health and nutrition examination survey. Am J Hum Biol. 1992;4:657–667. [DOI] [PubMed] [Google Scholar]
- 24.Hellerstedt WL, Jeffery RW. The association of job strain and health behaviours in men and women. Int J Epidemiol. 1997;26:575–583. [DOI] [PubMed] [Google Scholar]
- 25.House JS, Strecher V, Metzner HL, Robbins CA. Occupational stress and health among men and women in the Tecumseh Community Health Study. J Health Soc Behav. 1986;27:62–77. [PubMed] [Google Scholar]
- 26.Jonsson D, Rosengren A, Dotevall A, Lappas G, Wilhelmsen L. Job control, job demands and social support at work in relation to cardiovascular risk factors in MONICA 1995, Goteborg. J Cardiovasc Risk. 1999;6:379–385. [DOI] [PubMed] [Google Scholar]
- 27.Kornitzer M, Kittel F. How does stress exert its effects—smoking, diet and obesity, physical activity? Postgrad Med J. 1986;62:695–696. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Martikainen PT, Marmot MG. Socioeconomic differences in weight gain and determinants and consequences of coronary risk factors. Am J Clin Nutr. 1999; 69:719–726. [DOI] [PubMed] [Google Scholar]
- 29.Netterstrom B, Kristensen TS, Damsgaard MT, Olsen O, Sjol A. Job strain and cardiovascular risk factors: a cross sectional study of employed Danish men and women. Br J Ind Med. 1991;48:684–689. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Ostry AS, Radi S, Louie AM, LaMontagne AD. Psychosocial and other working conditions in relation to body mass index in a representative sample of Australian workers. BMC Public Health. 2006;6:53. Available at: http://www.biomedcentral.com/1471-2458/6/53. Accessed December 8, 2006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Reed DM, LaCroix AZ, Karasek RA, Miller D, MacLean CA. Occupational strain and incidence of coronary heart disease. Am J Epidemiol. 1989;129: 495–502. [DOI] [PubMed] [Google Scholar]
- 32.Rosmond R, Bjorntorp P. Psychosocial and socioeconomic factors in women and their relationship to obesity and regional body fat distribution. Int J Obes Relat Metab Disord. 1999;23:138–145. [DOI] [PubMed] [Google Scholar]
- 33.Wamala SP, Wolk K, Orth-Gomer K. Determinants of obesity in relation to socioeconomic status among middle-aged Swedish women. Prev Med. 1997; 26(5 pt 1):734–744. [DOI] [PubMed] [Google Scholar]
- 34.Siegrist J, Peter R. The effort-reward imbalance model. In: Schnall P, Belkic K, Landsbergis P, Baker D, eds. The Workplace and Cardiovascular Disease. Occup Med. 2000;15:83–87. [PubMed] [Google Scholar]
- 35.Shields M. Long working hours and health [1994–1997 data]. Health Rep. 1999;11:33–48. [PubMed] [Google Scholar]
- 36.van Amelsvoort LG, Schouten EG, Kok FJ. Duration of shiftwork related to body mass index and waist to hip ratio. Int J Obes Relat Metab Disord. 1999;23: 973–978. [DOI] [PubMed] [Google Scholar]
- 37.Laitinen J, Power C, Ek E, Sovio U, Jarvelin MR. Unemployment and obesity among young adults in a northern Finland 1966 birth cohort. Int J Obes Relat Metab Disord. 2002;26:1329–1338. [DOI] [PubMed] [Google Scholar]
- 38.Aldana SG, Pronk NP. Health promotion programs, modifiable health risks, and employee absenteeism. J Occup Environ Med. 2001;43:36–46. [DOI] [PubMed] [Google Scholar]
- 39.Bungum T, Satterwhite M, Jackson AW, Morrow JR Jr. The relationship of body mass index, medical costs, and job absenteeism. Am J Health Behav. 2003; 27:456–462. [DOI] [PubMed] [Google Scholar]
- 40.Pronk NP, Martinson B, Kessler RC, Beck AL, Simon GE, Wang P. The association between work performance and physical activity, cardiorespiratory fitness, and obesity. J Occup Environ Med. 2004;46: 19–25. [DOI] [PubMed] [Google Scholar]
- 41.Schmier JK, Jones ML, Halpern MT. Cost of obesity in the workplace. Scand J Work Environ Health. 2006;32:5–11. [DOI] [PubMed] [Google Scholar]
- 42.Moreau M, Valente F, Mak R, et al. Obesity, body fat distribution and incidence of sick leave in the Belgian workforce: the Belstress study. Int J Obes Relat Metab Disord. 2004;28:574–582. [DOI] [PubMed] [Google Scholar]
- 43.Burton WN, Chen CY, Schultz AB, Edington DW. The economic costs associated with body mass index in a workplace. J Occup Environ Med. 1998;40: 786–792. [DOI] [PubMed] [Google Scholar]
- 44.Tucker LA, Friedman GM. Obesity and absenteeism: an epidemiologic study of 10,825 employed adults. Am J Health Promot. 1998;12:202–207. [DOI] [PubMed] [Google Scholar]
- 45.Burton WN, Conti DJ. The real measure of productivity. Bus Health. 1999;17:34–36. [PubMed] [Google Scholar]
- 46.Rissanen A, Heliovaara M, Knekt P, Reunanen A, Aromaa A, Maatela J. Risk of disability and mortality due to overweight in a Finnish population. BMJ. 1990; 301:835–837. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Wang F, McDonald T, Champagne LJ, Edington DW. Relationship of body mass index and physical activity to health care costs among employees. J Occup Environ Med. 2004;46:428–436. [DOI] [PubMed] [Google Scholar]
- 48.Insurance Information Institute. Obesity, Liability & Insurance. Available at: http://www.iii.org/media/hottopics/insurance/obesity. Accessed November 1, 2004.
- 49.Sturm R. The effects of obesity, smoking, and drinking on medical problems and costs. Health Aff (Millwood). 2002;21:245–253. [DOI] [PubMed] [Google Scholar]
- 50.Sturm R, Wells KB. Does obesity contribute as much to morbidity as poverty and smoking? Public Health. 2001;115:229–235. [DOI] [PubMed] [Google Scholar]
- 51.Henschel A. Obesity as an occupational hazard. Can J Public Health. 1967;58:491–493. [PubMed] [Google Scholar]
- 52.Bernard B, ed. Musculoskeletal Disorders and Workplace Factors: A Critical Review of Epidemiologic Evidence for Work-Related Musculoskeletal Disorders of the Neck, Upper Extremities and Low Back. Cincinnati, Ohio: National Institute for Occupational Safety and Health, Centers for Disease Control and Prevention; 1997. DHHS (NIOSH) publication 97–141.
- 53.Stoyneva Z, Lyapina M, Tzvetkov D, Vodenicharov E. Current pathophysiological views on vibration-induced Raynaud’s phenomenon. Cardiovasc Res. 2003; 57:615–624 [DOI] [PubMed] [Google Scholar]
- 54.Griffin MJ. Handbook of Human Vibration. London, England: Academic Press; 1990.
- 55.Wieslander G, Norback D, Gothe CJ, Juhlin L. Carpal tunnel syndrome (CTS) and exposure to vibration, repetitive wrist movements, and heavy manual work: a case-referent study. Br J Ind Med. 1989;46: 43–47. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Tanaka S, Wild DK, Cameron LL, Freund E. Association of occupational and non-occupational risk factors with the prevalence of self-reported carpal tunnel syndrome in a national survey of the working population. Am J Ind Med. 1997;32:550–556. [DOI] [PubMed] [Google Scholar]
- 57.Walker-Bone KE, Palmer KT, Reading I, Cooper C. Soft-tissue rheumatic disorders of the neck and upper limb: prevalence and risk factors. Semin Arthritis Rheum. 2003;33:185–203. [DOI] [PubMed] [Google Scholar]
- 58.Balmes J, Becklake M, Blanc P, et al. American Thoracic Society statement: occupational contribution to the burden of airway disease. Am J Respir Crit Care Med. 2003;167:787–797. [DOI] [PubMed] [Google Scholar]
- 59.Baur X, Huber H, Degens PO, Allmers H, Ammon J. Relation between occupational asthma case history, bronchial methacholine challenge, and specific challenge test in patients with suspected occupational asthma. Am J Ind Med. 1998;33:114–122. [DOI] [PubMed] [Google Scholar]
- 60.Nystad W, Meyer HE, Nafstad P, Tverdal A, Engeland A. Body mass index in relation to adult asthma among 135,000 Norwegian men and women. Am J Epidemiol. 2004;160:969–976. [DOI] [PubMed] [Google Scholar]
- 61.Chen Y, Dales R, Tang M, Krewski D. Obesity may increase the incidence of asthma in women but not in men: longitudinal observations from the Canadian National Population Health Surveys. Am J Epidemiol. 2002;155:191–197. [DOI] [PubMed] [Google Scholar]
- 62.Xu B, Pekkanen J, Laitinen J, Jarvelin MR. Body build from birth to adulthood and risk of asthma. Eur J Public Health. 2002;12:166–170. [DOI] [PubMed] [Google Scholar]
- 63.Poulain M, Doucet M, Major GC, et al. The effect of obesity on chronic respiratory diseases: pathophysiology and therapeutic strategies. CMAJ. 2006;174: 1293–1299. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64.von Mutius E, Schwartz J, Neas LM, Dockery D, Weiss ST. Relation of body mass index to asthma and atopy in children: the National Health and Nutrition Examination Study III. Thorax. 2001;56:835–838. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65.Camargo CA Jr, Weiss ST, Zhang S, Willett WC, Speizer FE. Prospective study of body mass index, weight change, and risk of adult-onset asthma in women. Arch Intern Med. 1999;159:2582–2588. [DOI] [PubMed] [Google Scholar]
- 66.Shaheen SO, Sterne JA, Montgomery SM, Azima H. Birth weight, body mass index and asthma in young adults. Thorax. 1999;54:396–402. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 67.Luder E, Ehrlich RI, Lou WY, Melnik TA, Kattan M. Body mass index and the risk of asthma in adults. Respir Med. 2004;98:29–37. [DOI] [PubMed] [Google Scholar]
- 68.Mito N, Kitada C, Hosoda T, Sato K. Effect of diet-induced obesity on ovalbumin-specific immune response in a murine asthma model. Metabolism. 2002; 51:1241–1246. [DOI] [PubMed] [Google Scholar]
- 69.Rivera-Sanchez YM, Johnston RA, Schwartzman IN, et al. Differential effects of ozone on airway and tissue mechanics in obese mice. J Appl Physiol. 2004;96: 2200–2206. [DOI] [PubMed] [Google Scholar]
- 70.Jedrychowski W, Maugeri U, Flak E, Mroz E, Bianchi I. Predisposition to acute respiratory infections among overweight preadolescent children: an epidemiologic study in Poland. Public Health. 1998;112: 189–195. [DOI] [PubMed] [Google Scholar]
- 71.Jedrychowski W, Maugeri U, Flak E, Mroz E, Bianchi I. Cohort study on low physical activity level and recurrent acute respiratory infections in schoolchildren. Cent Eur J Public Health. 2001;9:126–129. [PubMed] [Google Scholar]
- 72.Aydin N, Soybir G, Odabas O, Karsidag T, Tuzun S. Factors influencing development of postoperative wound infection. Turkish J Surgery. 2003;19:133–142. [Google Scholar]
- 73.Bhati J, Pandey K, Rodrigues C, Mehta A, Joshi VR. Postoperative wound infection in patients undergoing coronary artery bypass graft surgery: a prospective study with evaluation of risk factors. Indian J Med Microbiol. 2003;21:246–251. [PubMed] [Google Scholar]
- 74.Luster MI, Portier C, Pait DG, et al. Risk assessment in immunotoxicology. II. Relationships between immune and host resistance tests. Fundam Appl Toxicol. 1993;21:71–82. [DOI] [PubMed] [Google Scholar]
- 75.La Cava A, Matarese G, Ebling FM, Hahn BH. Leptin-based immune intervention: current status and future directions. Curr Opin Investig Drugs. 2003;4: 1327–1332. [PubMed] [Google Scholar]
- 76.Collins S, Martin TL, Surwit RS, Robidoux J. Genetic vulnerability to diet-induced obesity in the C57BL/ 6J mouse: physiological and molecular characteristics. Physiol Behav. 2004;81:243–248. [DOI] [PubMed] [Google Scholar]
- 77.Marcos A, Nova E, Montero A. Changes in the immune system are conditioned by nutrition. Eur J Clin Nutr. 2003;57(suppl 1):S66–S69. [DOI] [PubMed] [Google Scholar]
- 78.Petro AE, Cotter J, Cooper DA, Peters JC, Surwit SJ, Surwit RS. Fat, carbohydrate, and calories in the development of diabetes and obesity in the C57BL/6J mouse. Metabolism. 2004;53:454–457. [DOI] [PubMed] [Google Scholar]
- 79.National Research Council, Institute of Medicine. Musculoskeletal Disorders and the Workplace: Low Back and Upper Extremities. Washington, DC: The National Academies Press; 2001. [PubMed]
- 80.Kortt M, Baldry J. The association between musculoskeletal disorders and obesity. Aust Health Rev. 2002;25:207–214. [DOI] [PubMed] [Google Scholar]
- 81.Miranda H, Viikari-Juntura E, Martikainen R, Takala EP, Riihimaki H. A prospective study of work related factors and physical exercise as predictors of shoulder pain. Occup Environ Med. 2001;58:528–534. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 82.Koleva M, Kostova V. Occupational and personal risk factors for musculoskeletal disorders in fertilizer plant workers. Cent Eur J Public Health. 2003;11: 9–13. [PubMed] [Google Scholar]
- 83.Roquelaure Y, Mariel J, Dano C, Fanello S, Penneau-Fontbonne D. Prevalence, incidence and risk factors of carpal tunnel syndrome in a large footwear factory. Int J Occup Med Environ Health. 2001;14:357–367. [PubMed] [Google Scholar]
- 84.Holmberg S, Thelin A, Thelin N. Knee osteoarthritis and body mass index: a population-based case–control study. Scand J Rheumatol. 2005;34: 59–64. [DOI] [PubMed] [Google Scholar]
- 85.Logroscino G, Marder K, Cote L, Tang MX, Shea S, Mayeux R. Dietary lipids and antioxidants in Parkinson’s disease: a population-based, case–control study. Ann Neurol. 1996;39:89–94. [DOI] [PubMed] [Google Scholar]
- 86.Mayeux R, Costa R, Bell K, Merchant C, Tang MX, Jacobs D. Reduced risk of Alzheimer’s disease among individuals with low caloric intake. Neurology. 1999; 52(suppl 2):A296–A297. [Google Scholar]
- 87.Abbott RD, Ross GW, White LR, et al. Midlife adiposity and the future risk of Parkinson’s disease. Neurology. 2002;59:1051–1057. [DOI] [PubMed] [Google Scholar]
- 88.Sriram K, Benkovic SA, Miller DB, O’Callaghan JP. Obesity exacerbates chemically induced neurodegeneration. Neuroscience. 2002;115:1335–1346. [DOI] [PubMed] [Google Scholar]
- 89.Wardle J, Steptoe A, Oliver G, Lipsey Z. Stress, dietary restraint and food intake. J Psychosom Res. 2000; 48:195–202. [DOI] [PubMed] [Google Scholar]
- 90.Jayo JM, Shively CA, Kaplan JR, Manuck SB. Effects of exercise and stress on body fat distribution in male cynomolgus monkeys. Int J Obes Relat Metab Disord. 1993;17:597–604. [PubMed] [Google Scholar]
- 91.Epel ES, McEwen B, Seeman T, et al. Stress and body shape: stress-induced cortisol secretion is consistently greater among women with central fat. Psychosom Med. 2000;62:623–632. [DOI] [PubMed] [Google Scholar]
- 92.Miller DB, O’Callaghan JP. Aging, stress and the hippocampus. Ageing Res Rev. 2005;4:123–140. [DOI] [PubMed] [Google Scholar]
- 93.McEwen BS. Glucocorticoids, depression, and mood disorders: structural remodeling in the brain. Metabolism. 2005;54(5 suppl 1):20–23. [DOI] [PubMed] [Google Scholar]
- 94.Fine LJ, Rosenstock L. Cardiovascular disorders. In: Rosenstock L, Cullen MR, Brodkin CA, Redlich CA, eds. Textbook of Clinical Occupational and Environmental Medicine. Philadelphia, Pa: Elsevier Saunders; 2005:563.
- 95.Olsen O, Kristensen TS. Impact of work environment on cardiovascular diseases in Denmark. J Epidemiol Community Health. 1991;45:4–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 96.Karasek R, Theorell T. The demand-control-support model and CVD. In: Schnall P, Blekic K, Landsbergis P, Baker D, eds. The Workplace and Cardiovascular Disease. Occup Med. 2000;15:78–83. [Google Scholar]
- 97.Simeonova PP, Hulderman T, Harki D, Luster MI. Arsenic exposure accelerates atherogenesis in apolipoprotein E(–/–) mice. Environ Health Perspect. 2003;111:1744–1748. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 98.Simeonova PP, Luster MI. Arsenic and atherosclerosis. Toxicol Appl Pharmacol. 2004;198:444–449. [DOI] [PubMed] [Google Scholar]
- 99.Suadicani P, Hein HO, Gyntelberg F. Airborne occupational exposure, ABO phenotype and risk of ischaemic heart disease in the Copenhagen Male Study. J Cardiovasc Risk. 2002;9:191–198. [DOI] [PubMed] [Google Scholar]
- 100.Pope CA III, Burnett RT, Thurston GD, et al. Cardiovascular mortality and long-term exposure to particulate air pollution: epidemiological evidence of general pathophysiological pathways of disease. Circulation. 2004;109:71–77. [DOI] [PubMed] [Google Scholar]
- 101.Wisse BE. The inflammatory syndrome: the role of adipose tissue cytokines in metabolic disorders linked to obesity. J Am Soc Nephrol. 2004;15:2792–2800. [DOI] [PubMed] [Google Scholar]
- 102.Dirx MJ, Zeegers MP, Dagnelie PC, van den Bogaard T, van den Brandt PA. Energy restriction and the risk of spontaneous mammary tumors in mice: a meta-analysis. Int J Cancer. 2003;106:766–770. [DOI] [PubMed] [Google Scholar]
- 103.Albanes D. Caloric intake, body weight and cancer: a review. Nutr Cancer. 1987;9:199–217. [DOI] [PubMed] [Google Scholar]
- 104.Kritchevsky D, Klurfeld DM. Influence of caloric intake on experimental carcinogenesis: a review. Adv Exp Med Biol. 1986;206:55–68. [DOI] [PubMed] [Google Scholar]
- 105.Brown ND, Thomas NI. Exploring variables among medical center employees with injuries: developing interventions and strategies. AAOHN J. 2003; 51:470–481. [PubMed] [Google Scholar]
- 106.Bhattacherjee A, Chau N, Sierra CO, et al. Relationships of job and some individual characteristics to occupational injuries in employed people: a community-based study. J Occup Health. 2003;45:382–391. [DOI] [PubMed] [Google Scholar]
- 107.Chau N, Mur JM, Touron C, Benamghar L, Dehaene D. Correlates of occupational injuries for various jobs in railway workers: a case–control study. J Occup Health. 2004;46:272–280. [DOI] [PubMed] [Google Scholar]
- 108.Froom P, Melamed S, Kristal-Boneh E, Gofer D, Ribak J. Industrial accidents are related to relative body weight: the Israeli CORDIS study. Occup Environ Med. 1996;53:832–835. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 109.Stoohs RA, Guilleminault C, Itoi A, Dement WC. Traffic accidents in commercial long-haul truck drivers: The influence of sleep-disordered breathing and obesity. Sleep. 1994;17:619–623. [PubMed] [Google Scholar]
- 110.Lichtenstein MJ, Bolton A, Wade G. Body mass as a determinant of seat belt use. Am J Med Sci. 1989; 297:233–237. [DOI] [PubMed] [Google Scholar]
- 111.Mock CN, Grossman DC, Kaufman RP, Mack CD, Rivara FP. The relationship between body weight and risk of death and serious injury in motor vehicle crashes. Accid Anal Prev. 2002;34:221–228. [DOI] [PubMed] [Google Scholar]
- 112.Edwards M. Anthropometric measurements and ejection injuries. Aviat Space Environ Med. 1996;67: 1144–1147. [PubMed] [Google Scholar]
- 113.Hsiao H, Long D, Snyder K. Anthropometric differences among occupational groups. Ergonomics. 2002;45:136–152. [DOI] [PubMed] [Google Scholar]
- 114.Turner N, Sinkule E, Eschenbacher W. Metabolic and respiratory responses during the performance of a 60-minute man test 4. Presented at: International Society for Respiratory Protection Conference, Pittsburgh, Pa: September 1999. Available at: http://www.isrp.com.au/isrpcom/journal/pa_abstracts/abstract__turner.htm. Accessed December 8, 2006.
- 115.Hsiao H, Bradtmiller B, Whitestone J. Sizing and fit of fall-protection harnesses. Ergonomics. 2003;46: 1233–1258. [DOI] [PubMed] [Google Scholar]
- 116.Ilmarinen R, Lindholm H, Koivistoinen K, Helisten P. Physiological evaluation of chemical protective suit systems (CPSS) in hot conditions. Int J Occup Saf Ergon. 2004;10:215–226. [DOI] [PubMed] [Google Scholar]
- 117.Marszalek A, Smolander J, Soltynski K. Age-related thermal strain in men while wearing radiation protective clothing during short-term exercise in the heat. Int J Occup Saf Ergon. 2004;10:361–367. [DOI] [PubMed] [Google Scholar]
- 118.Chung NK, Pin CH. Obesity and occurrence of heat disorders. Mil Med. 1996;161:739–742. [PubMed] [Google Scholar]
- 119.Ottman R. An epidemiologic approach to gene–environment interaction. Gen Epid. 1990;7:177–185. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 120.Mead MN. Origins of obesity. Environ Health Perspect. 2004;112:A344. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 121.Dejoy DM, Southern DJ. An integrative perspective on work-site health promotion. J Occup Med. 1993; 35:1221–1230. [PubMed] [Google Scholar]
- 122.Barbeau EM, Wallace L, Lederman R, Lightman N, Stoddard A, Sorensen G. Recruiting small manufacturing worksites that employ multiethnic, low-wage work-forces into a cancer prevention research trial. Prev Chronic Dis [serial online]. July 2004. Available at: http://www.cdc.gov/pcd/issues/2004/jul/03_0020.htm. Accessed December 8, 2006. [PMC free article] [PubMed]
- 123.Sorensen G, Barbeau EM. Integrating occupational health, safety and worksite health promotion: opportunities for research and practice. Med Lav. 2006; 97:240–257. [PubMed] [Google Scholar]
- 124.Sorensen G, Barbeau E, Stoddard A, Hunt M, Kaphingst K, Wallace L. Promoting behavior change among working-class, multiethnic workers: results of the healthy directions–small business study. Am J Public Health. 2005;95:1389–1395. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 125.Yancey AK, McCarthy WJ, Taylor WC, et al. The Los Angeles Lift Off: a sociocultural environmental change intervention to integrate physical activity into the workplace. Prev Med. 2004;38:848–856. [DOI] [PubMed] [Google Scholar]
- 126.Chenoweth D. Using obesity-related medical claims cost analysis to influence obesity prevention and intervention approaches in worksite environment. Presented at: Obesity and the Built Environment: Improving Public Health Through Community Design; sponsored by National Institute of Environmental Health Sciences; May 24–25, 2004; Washington, DC.
- 127.Perbellini L. Job as a risk factor for obesity … and the contrary [In Italian]. Med Lav. 2004;95:211–222. [PubMed] [Google Scholar]
- 128.Swinburn B, Egger G. Preventive strategies against weight gain and obesity. Obes Rev. 2002;3:289–301. [DOI] [PubMed] [Google Scholar]
- 129.Katz DL, O’Connell M, Yeh MC, et al. Public health strategies for preventing and controlling overweight and obesity in school and worksite settings: a report on recommendations of the Task Force on Community Preventive Services. MMWR Recomm Rep. 2005;54(RR-10):1–12. [PubMed] [Google Scholar]
- 130.Puhl R, Brownell KD. Ways of coping with obesity stigma: review and conceptual analysis. Eat Behav. 2003;4:53–78. [DOI] [PubMed] [Google Scholar]
- 131.Paul RJ, Townsend JB. Shape up or ship out? Employment discrimination against the overweight. Employer Responsibilities Rights J. 1995;8:133–145. [Google Scholar]
- 132.Roehling MV. Weight-based discrimination in employment: psychological and legal aspects. Personnel Psychol. 1999;52:969–1017. [Google Scholar]
- 133.Neumark-Sztainer D, Story M, Harris T. Beliefs and attitudes about obesity among teachers and school health care providers working with adolescents. J Nutr Educ. 1999;31:3–9. [Google Scholar]
- 134.Maroney D, Golub S. Nurses’ attitudes toward obese persons and certain ethnic groups. Percept Mot Skills. 1992;75:387–391. [DOI] [PubMed] [Google Scholar]
- 135.Young LM, Powell B. The effects of obesity on the clinical judgments of mental health professionals. J Health Soc Behav. 1985;26:233–246. [PubMed] [Google Scholar]
- 136.Carr D, Friedman MA. Is obesity stigmatizing? Body weight, perceived discrimination, and psychological well-being in the United States. J Health Soc Behav. 2005;46:244–259. [DOI] [PubMed] [Google Scholar]
- 137.Mich. Elliot–Larsen Civil Rights Act §453.
- 138.Walters GA. Future of obesity and chronic-disease management in health care: the employer perspective. Obes Res. 2002;10(suppl 1):S84–S86. [DOI] [PubMed] [Google Scholar]
- 139.Moorman AM, Eickhoff-Shemek JM. The legal aspects: is obesity a disability under the ADA (Americans With Disabilities Act). ACSM Health Fitness J. 2005;9: 29–31. [Google Scholar]
- 140.Primack A. Future of obesity and disease management in health care: the government perspective. Obes Res. 2002;(10 suppl 1):S82–S83. [DOI] [PubMed]
- 141.Centers for Medicare and Medicaid Services. Treatment of Obesity. Medlearn Matters no. MM3502; October 1, 2004.
- 142.Social Security Ruling, SSR 00-3p. Titles II and XVI: Evaluation of obesity, 65 Federal Register 31039–31043 (2000).
- 143.Wolf AM, Colditz GA. Current estimates of the economic cost of obesity in the United States. Obes Res. 1998;6:97–106. [DOI] [PubMed] [Google Scholar]
- 144.Tsai SP, Donnelly RP, Wendt JK. Obesity and mortality in a prospective study of a middle-aged industrial population. J Occup Environ Med. 2006;48: 22–27. [DOI] [PubMed] [Google Scholar]
- 145.Tillett S, Sullivan P. Asbestos screening and education programs for building and construction trades unions. Am J Ind Med. 1993;23:143–152. [DOI] [PubMed] [Google Scholar]
- 146.Waage HP, Vatten LJ, Opedal E, Hilt B. Smoking intervention in subjects at risk of asbestos-related lung cancer. Am J Ind Med. 1997;31:705–712. [DOI] [PubMed] [Google Scholar]
- 147.Cassell JA. Social anthropology and nutrition: a different look at obesity in America. J Am Diet Assoc. 1995;95:424–427. [DOI] [PubMed] [Google Scholar]
- 148.Whittington G. Changes in workers’ compensation laws in 2004. Monthly Labor Rev. 2005;Jan:28–32.