

A 35-year-old man presented to his family physician with complaints of redness and discomfort in his left eye. His family physician noted on examination that there appeared to be “sparkles” in the patient's eye (Figs. 1 and 2) and referred him for ophthalmologic assessment. The patient said that he had lost his sight in his left eye some years before, although he could not recall precisely when this had occurred, or the nature of his loss of vision. He was mentally retarded to a mild degree, but had no other medical problems.
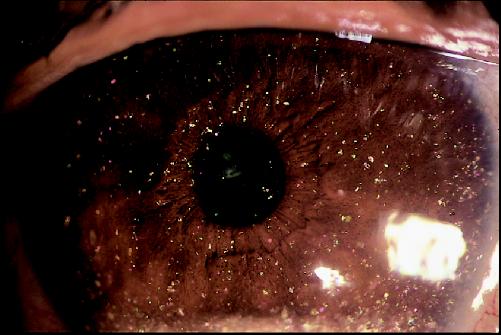
Figure 1. Photo: Images courtesy of the Ophthalmic Photography Department, University of British Columbia

Figure 2. Photo: Images courtesy of the Ophthalmic Photography Department, University of British Columbia
Examination of this patient revealed visual acuities of 20/20 in the right eye and no light perception in the left eye. Crystals could be seen layering inferiorly in the anterior chamber of the left eye on gross examination. The pupil was bound to the lens, with the lens itself being clear. There were also crystals in the vitreous and a total funnel-shaped retinal detachment. A diagnosis of anterior chamber cholesterolosis was reached.
It is believed that cholesterol is released from the breakdown of intraocular red blood cells and then crystallizes. This may be secondary to trauma or protracted inflammation.1 Vitreous hemorrhage occurring in the posterior chamber may cause cholesterol crystal formation that is specifically termed synchisis scintillans. Diffusion into the anterior chamber is facilitated by aphakia (absence of a lens) or lens subluxation, but these conditions are not required.2 Phacolysis (removal of the lens) itself can also cause crystal formation, possibly from the degradation of intralenticular membranes.3 Chronic retinal detachment can cause leakage of cholesterol-rich subretinal fluid without hemorrhage, resulting in cholesterolosis (the likely mechanism involved in this case). Finally, cholesterol crystals in the anterior chamber may also form in situ and have been reported following hyphema.4
The presence of crystals in the anterior chamber always indicates some serious underlying disorder1 requiring ophthalmologic assessment. Microscopy of an anterior chamber aspirate may reveal characteristic rectangular or rhomboid cholesterol crystals. Slit-lamp specular microscopy has also been described as a useful noninvasive diagnostic tool.5 Other types of anterior chamber crystals include calcium oxalate and multiple myeloma, but these are even rarer.
Unfortunately, treatment options for anterior chamber cholesterolosis are limited and relate to the underlying disease process. Steroids may be used for reactive endophthalmitis and in this case improved the patient's painful symptoms. Loss of vision, however, is less amenable to treatment, except when phacolysis is the underlying cause.1
Suren Sanmugasunderam Ari Giligson Department of Ophthalmology University of British Columbia Vancouver, BC Stephen B. Choi Editorial Fellow CMAJ
References
- 1.Kennedy CJ. The pathogenesis of polychromatic cholesterol crystals in the anterior chamber. Aust N Z J Ophthalmol 1996;24(3):267-73. [DOI] [PubMed]
- 2.Eagle RC Jr, Yanoff M. Cholesterolosis of the anterior chamber. Albrecht Von Graefes Arch Klin Exp Ophthalmol 1975;193:121-34 [DOI] [PubMed]
- 3.Brooks AM, Drewe RH, Grant GB, Billington T, Gillies WE. Crystalline nature of the iridescent particles in hypermature cataracts. Br J Ophthalmol 1994;78(7):581-2. [DOI] [PMC free article] [PubMed]
- 4.Hemady R, Foster CS. Anterior chamber crystals following hyphema. Arch Ophthalmol 1990;108(1):14-5. [DOI] [PubMed]
- 5.Hurley IWJ, Brooks AMV, Reinehr DP, Grant GB, Gillies WE. Identifying anterior segment crystals. Br J Ophthalmol 1991;75:329-31. [DOI] [PMC free article] [PubMed]