

Abstract
Objective To determine if research has adequately examined the health needs of the aboriginal population of Canada.
Design Review.
Study selection Medline search of journal articles published during 1992-2001. The search terms used were “Canada” and various synonyms and categories for Canadian aboriginal people. Each paper was categorised according to the aboriginal group, age-sex group, comparison group, geographic location, and type of research topic (health determinant, health status, or health care).
Results Of 352 citations found, 254 were selected after elimination of those without abstracts, not containing data on Canada, or not focusing on health issues. The proportion of papers does not reflect the demographic composition of aboriginal people in Canada, with severe under-representation of Métis, urban aboriginal people, and First Nations people not living on reserves and over-representation of the Inuit. Children and women received less attention proportional to their share of the population. A few prolific research groups have generated a disproportionate amount of publications from a few communities and regions. 174 papers dealt with health determinants (for example, genetics, diet, and contaminants), 173 with health status, and 75 with health care. Injuries, which account for a third of all deaths, were studied in only 8 papers. None of the health care papers examined rehabilitation.
Conclusion Researchers have not adequately examined several important health needs of the aboriginal population.
Introduction
Despite tremendous progress, the health of the aboriginal population of Canada continues to lag behind that of the national population.1 Health research may hold the key to why such disparities exist and to solutions for eliminating them. In 1990 the Commission on Health Research for Development recognised the close links between health research and equity in development and promoted the concept of “essential national health research.”2 Since then the “10/90 gap” (less than 10% of global spending on health research is devoted to diseases that account for 90% of the global disease burden) has become recognised.3 The Global Forum for Health Research advocates setting priorities on health research on the basis of analyses of disease burden, health determinants, current knowledge, cost effectiveness, and available resources.
This paper aims to review health research conducted among Canadian aboriginal people and to determine if research has examined the health needs of the population. While recent international studies have used a common “currency” (such as disability adjusted life years) to measure disease burden and impact,4 which would facilitate considerably the priority setting process, such an approach cannot yet be used for the Canadian aboriginal population.
According to the 2001 Canadian census, just under one million (3.3%) Canadians identified themselves as aboriginal. The aboriginal population comprises 62% First Nations people (or “Indians”), 30% Métis, 5% Inuit, and 3% people with more than one identity.5
The health status of aboriginal people improved considerably in the second half of the 20th century in relation to, for example, life expectancy, infant mortality, and incidence of tuberculosis.6-8 A health transition can be observed,9 characterised by the decline but persistence of infectious diseases, followed by the rise of chronic diseases such as diabetes and injuries.10
Much early research on the health of aboriginal people in Canada consisted of clinical observations and laboratory investigations into physiological adaptation. In the past 20-30 years, however, population based studies have been conducted on the distribution, aetiology, and control of common diseases—such as tuberculosis and diabetes—and on suicide; studies also examined the cultural aspects of illness and healing.
Methods
I did a Medline search covering 1992-2001. For search terms, I used the various names for aboriginal groups (“Indian,” “Métis,” “Inuit,” “Eskimo,” “Native,” “Aboriginal”) and “Canada.” For each abstract, I obtained information on aboriginal identity, age-sex group, comparison group, geographic location of research, research topic, and associations between exposure and outcome. Each paper can be given more than one label under each category.
Research topics are broadly divided into those dealing with “health determinants,” “health status,” and “health care.” The inter-relations between these three categories are also recorded.
Results
The 352 citations generated by Medline were reduced to 254. Citations without abstracts and those not focusing on Canada, aboriginal people, or health were eliminated.
Over 60% (158) of papers referred to First Nations people, only two of which dealt with those not living on Indian reserves (“off-reserve”). The Inuit were represented in 122 papers. Only two papers provided data on the Métis, and five on urban aboriginal people (figure). The Cree and Ojibwa were the tribal groups most studied, accounting for 37 of papers.
Figure 1.
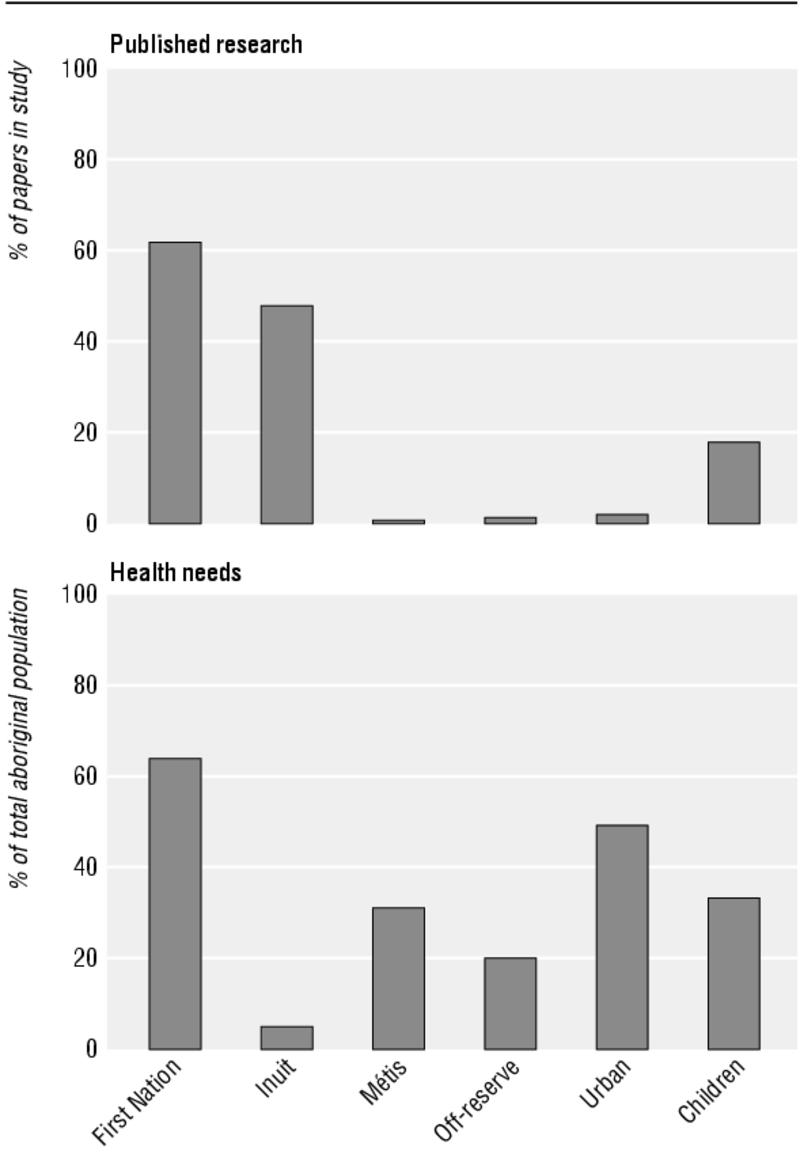
Comparison of published research and health needs among Canadian aboriginal populations
The age-sex group was specified in 148 papers. Twenty eight papers dealt specifically with women, and 46 specifically with children.
One hundred and thirty eight papers did not specify a comparison group. Eighty one used the non-aboriginal population in the study area, “all Canadians,” or the total population in the province; four specified the southern regions of the country. Eleven papers specified “caucasian,” “white,” or “euro-Canadian” as the comparison group.
Forty two studies were national in scope. All three northern territories, but only six (out of 10) provinces and three cities were represented in regional or community studies. Fifty one studies were based on single communities; one of these communities, the site of a long term diabetes study, accounted for 25 studies.11
One hundred and seventy four papers dealt with health determinants, 173 with health status, and 75 with health care.
Human biology (including genetics) accounted for 72 of the 174 papers dealing with health determinants, followed by lifestyle (49), social environment (49), and physical environment (33). Genetics was studied in 39 of the 72 human biology papers. The most important lifestyle factor studied was diet, mentioned in half of the papers on lifestyle and personal behaviours; other behaviours such as smoking, sexual practices, and alcohol and drug misuse together accounted for 22 of the papers on health determinants.
Most (29) of the 33 studies on the physical environment related to chemical contaminants, with only 10 dealing with housing, climate, and geographic isolation.
Studies dealing with the social environment encompassed socioeconomic and psychosocial factors and broader issues such as marginalisation, social disorganisation, colonialism, and cultural change.
Under the category of health status, 173 studies covered specific diseases, general measures of health status, or physiological function. Chronic diseases accounted for the largest number (77, of which 30 dealt with diabetes and related disorders and 19 with cancer), followed by infectious diseases (41, of which 14 dealt with tuberculosis and 8 with HIV). Injury (mostly suicide) was studied only in eight papers and mental health (mostly substance misuse) in seven papers.
Of 75 papers dealing with some aspect of health care, 48 dealt with curative services and 26 with prevention and public health. None dealt with rehabilitation.
The table shows the inter-relations between health determinants, health status, and health care. The 254 papers can be classified according to nine non-mutually exclusive categories (box).
Table 1.
Classification of studies on aboriginal health in Canada : health determinants, health status, and health care and their inter-relations
|
Outcome variable
|
|||
|---|---|---|---|
| Exposure variable | Health determinants | Health status | Health care |
| Health determinants | 60 (A) | 92 (B) | 20 (C) |
| Health status | 1 (D) | 36 (E) | 20 (F) |
| Health care | 1 (G) | 24 (H) | 10 (I) |
Categories are not mutually exclusive.
See box for key to letters A to I.
Discussion
I reviewed only research that was reported in journal articles indexed in Medline. I assessed the content but not the quality of research. I also did not take into account research which falls outside the Western scientific tradition—often conducted by indigenous people and based on indigenous knowledge.
The research fails to reflect the demographic composition of Canadian aboriginal people, with severe under-representation of Métis, urban residents, and First Nations people not living on reserves. The Inuit are overstudied relative to their share of the aboriginal population. Research has not focused enough on the unique health needs of women and children.
The choice of a comparison group is driven by the hypothesis being tested—for example, whether it is “ethnicity,” “race,” “poverty,” or “isolation” that is being used to explain the disparities. The comparison group used most often is Canadians nationally, which is appropriate as improving the health of aboriginal people to the level of all Canadians is a declared goal of governments. Often overlooked are the considerable geographic, cultural, socioeconomic, and indeed health differences in the aboriginal population. A case can be made to compare communities in similar circumstances in terms of variables such as access to health services and infrastructure. On the other hand, statistically “controlling” for socioeconomic status and geographic isolation, while feasible, may not be advisable, as such factors are central to the aboriginal experience in many regions, and removing them takes away the most powerful explanatory variable.
Non-mutually exclusive categories to which papers were assigned
Health determinants only (the distribution of a health determinant (for example, the prevalence of smoking) or the inter-relations among different types of determinants (for example, diet and environmental contaminants))
Effect of a health determinant on health status (for example, the risk factors for suicide)
Effect of a health determinant on health care—that is, how a health determinant affects the use of health services (for example, socioeconomic status and hospitalisation rate)
Effect of health status on a health determinant (for example, the impact of diabetes on employment)
Health status only (the clinical features of a disease, pattern of health, or course of an epidemic—for example, growth monitoring of children)
Effect of health status on health care—that is, how disease burden determines the need for and costs of services (for example, the prevalence of caries and planning dental services)
Effect of health care on a health determinant—that is, the effects of a service or intervention on the prevalence of a risk factor (for example, health promotion on drug misuse)
Effect of health care on health status—that is, the impact of health interventions on reducing disease burden or improving health status (for example, dietary supplementation and rickets)
Health care only (organisation and delivery of health care or a specific intervention programme without evaluation—for example, aeromedical evacuation (transfer of patients by air for medical care)) circumstances in terms of variables such as access to health services and infrastructure. On the other hand, statistically “controlling” for socioeconomic status and geographic isolation, while feasible, may not be advisable, as such factors are central to the aboriginal experience in many regions, and removing them takes away the most powerful explanatory variable.
Comparative studies often assume implicitly that the non-aboriginal is the “ideal” or “normal” group. From a policy perspective, it is useful to consider the population with the “better” rate as indicating what is feasible and achievable. The discrepancy can then be used to direct research into seeking explanations and designing appropriate interventions. Traditionally, First Nation data are broken down by externally defined regions. Increasingly First Nations people prefer to see data aggregated according to tribal affiliations (such as Cree Nation and Mohawk Nation), which transcend provincial boundaries.
A few prolific research groups have generated a disproportionate amount of publications from several communities and regions. At the moment, aboriginal health research is limited to only a few centres in the country.
Without estimates of attributable risks specific to the aboriginal population, it is difficult to assess if research on determinants corresponds to their public health significance. It seems that genetics and environmental contaminants have received far more attention than other, especially social, determinants. The prevalence of smoking, for example, is very high (62%) among aboriginal people, yet only 3% of publications deal with the issue of smoking
Although the increasing importance of chronic diseases such as diabetes is reflected in the research literature, researchers have not paid sufficient attention to injuries. Although injuries account for a third of all deaths, they are the subject of research in only 3% of publications. It is not surprising that curative services received the most attention, as it reflects their relative importance in healthcare financing. Rehabilitation has been grossly neglected by health researchers.
Aboriginal health research in Canada has taken a quantum leap in the past two years, with the establishment of the Institute of Aboriginal People's Health (an institute of the Canadian Institutes of Health Research). Not only has funding been increased substantially, but several strategic initiatives and special programmes were launched to build capacity and develop the infrastructure nationally.12 It is too early to assess if the increased funding for research is adequate or appropriate to the needs.
Although gaps are identified in this study, the solution is not necessarily to make the bars in the upper and lower parts of the figure equal in length. In developing research priorities, it is not just health needs that should be considered, but also the amenability of the health issue to research. There will continue to be a need to strike a balance between targeted research based on an explicit planning process and curiosity driven, investigator initiated research.
What is already known on this topic
Considerable research has been conducted on Aboriginal health issues in Canada
Whether this research assesses the health needs of the population has never been examined
What this study adds
Discrepancies exist between research and major health indicators
Research priorities need to be set on the basis of health status and health determinants of the aboriginal population
Supplementary Material
 Sixty six of the 254 references appear on bmj.com as examples of the articles reviewed
Sixty six of the 254 references appear on bmj.com as examples of the articles reviewed
TKY has received a senior investigator award from the Canadian Institute of Health Research.
Contributors: TKY is the sole author of this paper.
Funding: No special funding.
Competing interests: None declared.
References
- 1.Waldram JB, Herring DA, Young TK. Aboriginal health in Canada: historical, cultural, and epidemiological perspectives. Toronto: University of Toronto Press, 1995.
- 2.Commission on Health Research for Development. Health research: essential link to equity in development. New York: Oxford University Press, 1990.
- 3.Global Forum for Health Research. The 10/90 report on health research 2001-2002. Geneva: 2002. www.globalforumhealth.org/pages/index.asp (accessed 22 July 2003)
- 4.World Health Organization. The world health report 2002. Geneva: WHO, 2002.
- 5.Statistics Canada. 2001 Census. Aboriginal peoples of Canada: a demographic profile. Ottawa: Statistics Canada, 2003. www12.statcan.ca/english/census01/products/analytic/companion/abor/contents.cfm (accessed 22 July 2003)
- 6.Young TK. The Health of Native Americans: towards a biocultural epidemiology. New York: Oxford University Press, 1994.
- 7.MacMillan HL, MacMillan AB, Offord DR, Dingle JL. Aboriginal health. Can Med Assoc J 1996;155: 1569-78. [PMC free article] [PubMed] [Google Scholar]
- 8.Bjerregaard P, Young TK. The circumpolar Inuit: health of a population in transition. Copenhagen: Munksgaard International, 1998.
- 9.Young TK. Are subarctic Indians undergoing the epidemiologic transition? Soc Sci Med 1988;26: 659-71. [DOI] [PubMed] [Google Scholar]
- 10.Young TK, Reading J, Elias B, O'Neil JD. Type 2 diabetes mellitus in Canada's First Nations: status of an epidemic in progress. Can Med Assoc J 2000;163: 561-6. [PMC free article] [PubMed] [Google Scholar]
- 11.Harris SB, Gittelsohn J, Hanley AJG, Barnie A, Wolever TMS, Gao J, et al. The prevalence of NIDDM and associated risk factors in native Canadians. Diabet Care 1997;20: 185-97. [DOI] [PubMed] [Google Scholar]
- 12.Reading J, Nowgesic E. Improving the health of future generations: the Canadian Institutes of Health Research Institute of Aboriginal People's Health. Am J Public Health 2002;92: 1396-400. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.