

Abstract
A group of 163 men in the Hamilton, Ont. region who had suffered a myocardial infarction were enrolled in a rehabilitation program of physical activity. These men constituted one cohort of a multicentre collaborative study designed to determine the effects of regular exercise of differing intensity on morbidity and mortality over a 4-year period.
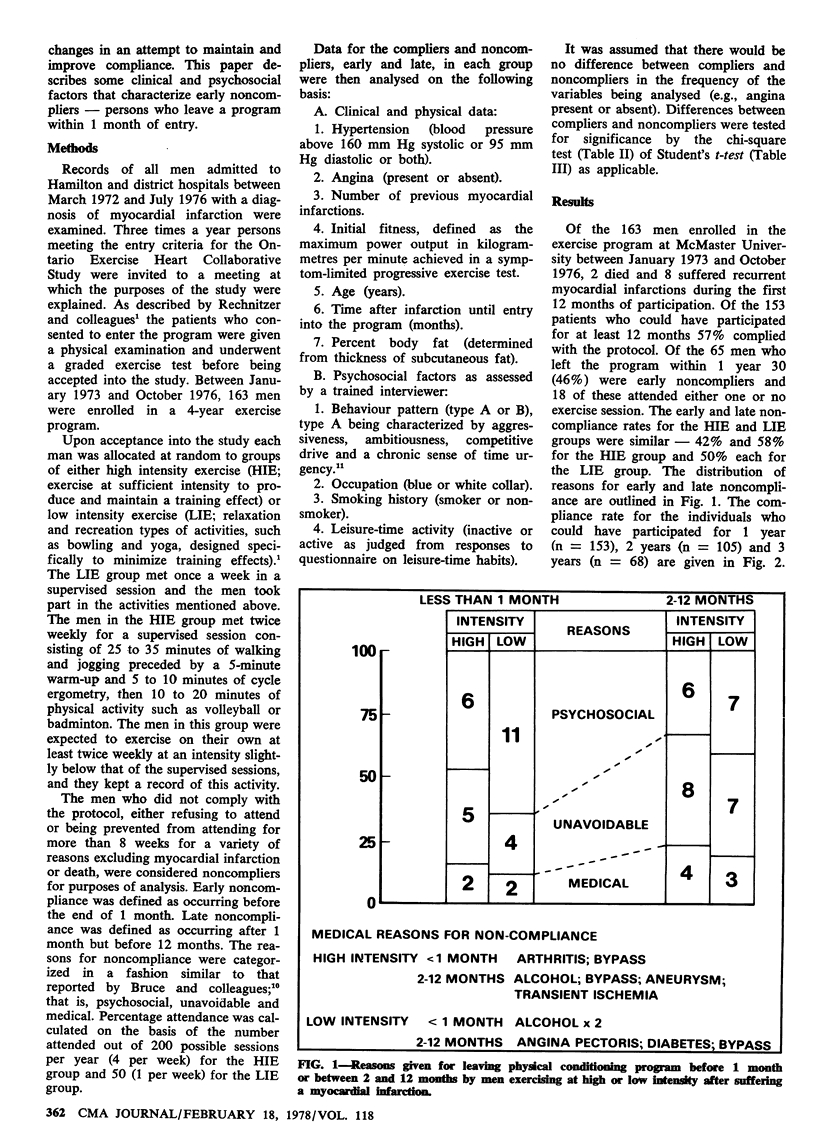
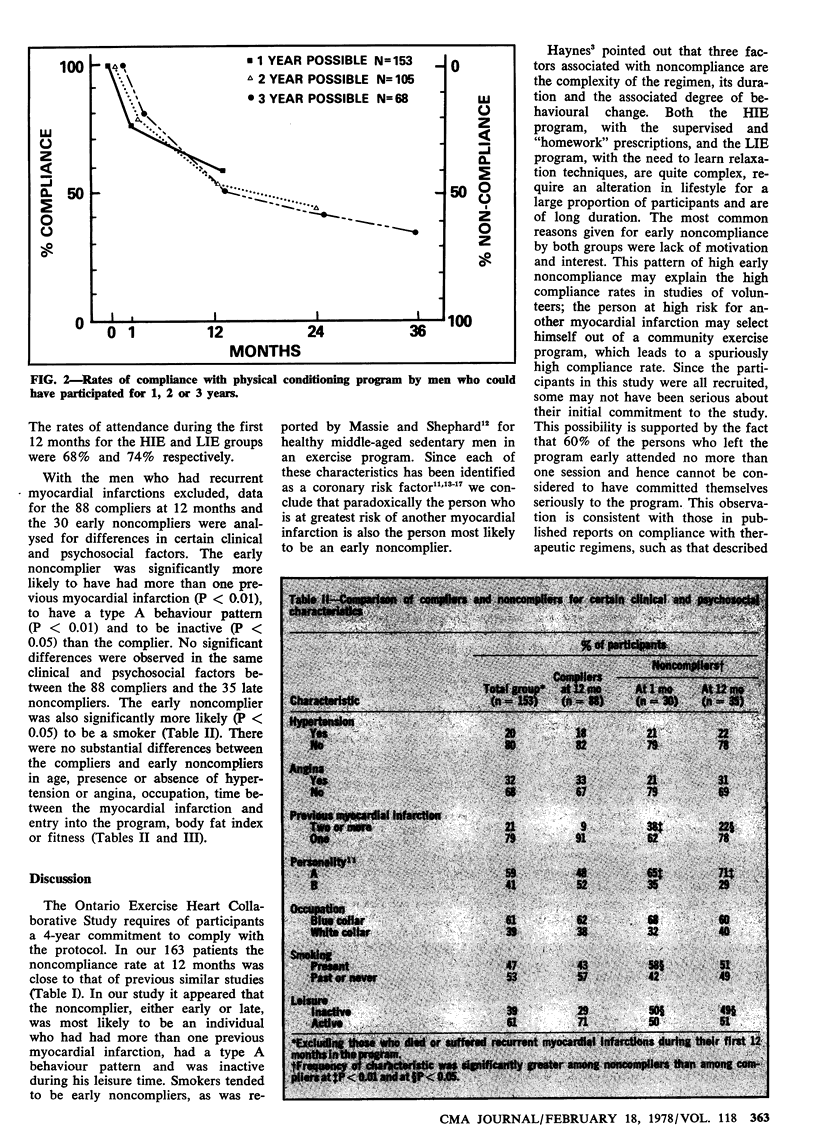
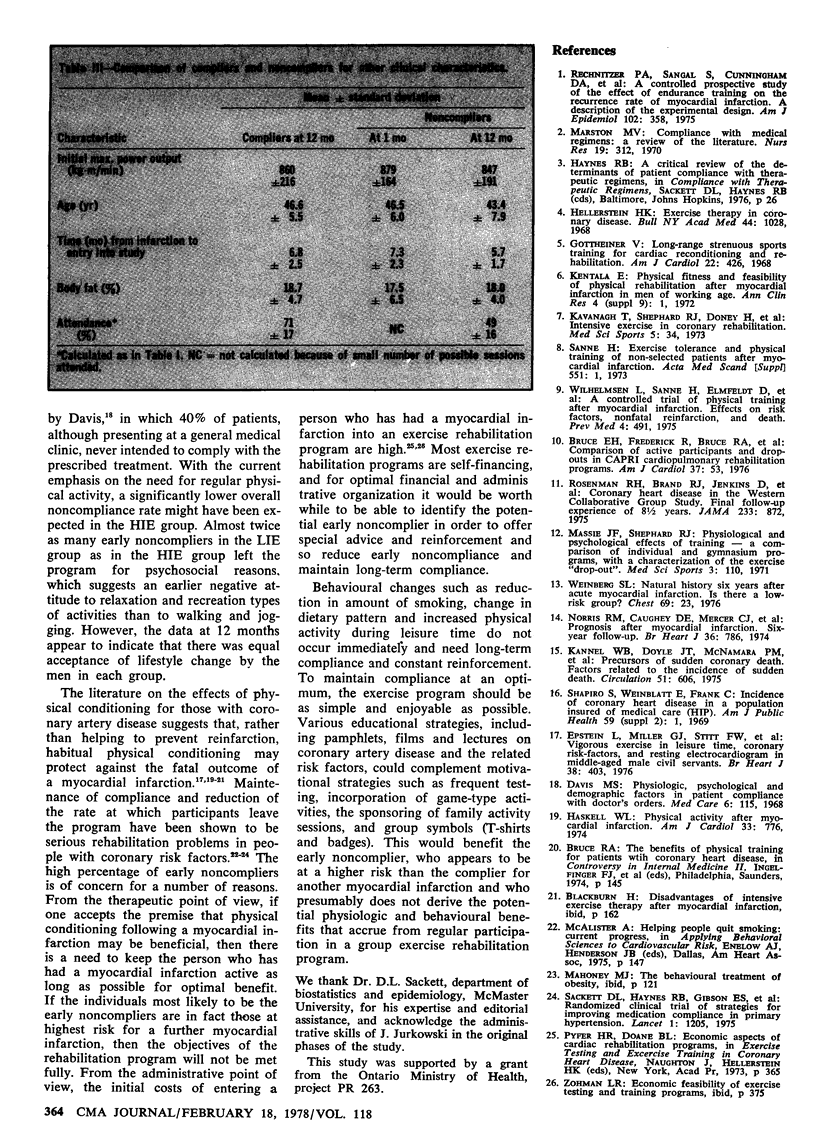
The noncompliance rate was 43% for the men who could have participated for 1 year, 46% of whom were classified as noncompliers within 1 month of entry into the program. There was no difference in overall compliance between the men exercising at high intensity and those exercising at low intensity; lack of motivation or interest was the most common reason for their leaving the program. Those leaving the program early tended to have a type A behaviour pattern (they were aggressive, ambitious and competitive, with a chronic sense of time urgency), were inactive during their leisure time, had had at least two previous infarctions and smoked. These characteristics suggest that the men leaving the program early may have been those at greatest risk for a further myocardial infarction.
Full text
PDF
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Bruce E. H., Frederick R., Bruce R. A., Fisher L. D. Comparison of active participants and dropouts in CAPRI cardiopulmonary rehabilitation programs. Am J Cardiol. 1976 Jan;37(1):53–60. doi: 10.1016/0002-9149(76)90499-9. [DOI] [PubMed] [Google Scholar]
- Epstein L., Miller G. J., Stitt F. W., Morris J. N. Vigorous exercise in leisure time, coronary risk-factors, and resting electrocardiogram in middle-aged male civil servants. Br Heart J. 1976 Apr;38(4):403–409. doi: 10.1136/hrt.38.4.403. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gottheiner V. Long-range strenuous sports training for cardiac reconditioning and rehabilitation. Am J Cardiol. 1968 Sep;22(3):426–435. doi: 10.1016/0002-9149(68)90126-4. [DOI] [PubMed] [Google Scholar]
- Haskell W. L. Physical activity after myocardial infarction. Am J Cardiol. 1974 May 20;33(6):776–783. doi: 10.1016/0002-9149(74)90220-3. [DOI] [PubMed] [Google Scholar]
- Hellerstein H. K. Exercise therapy in coronary disease. Bull N Y Acad Med. 1968 Aug;44(8):1028–1047. [PMC free article] [PubMed] [Google Scholar]
- Kannel W. B., Doyle J. T., McNamara P. M., Quickenton P., Gordon T. Precursors of sudden coronary death. Factors related to the incidence of sudden death. Circulation. 1975 Apr;51(4):606–613. doi: 10.1161/01.cir.51.4.606. [DOI] [PubMed] [Google Scholar]
- Marston M. V. Compliance with medical regimens: a review of the literature. Nurs Res. 1970 Jul-Aug;19(4):312–323. [PubMed] [Google Scholar]
- Massie J. F., Shephard R. J. Physiological and psychological effects of training--a comparison of individual and gymnasium programs, with a characterization of the exercise "drop-out". Med Sci Sports. 1971 Fall;3(3):110–117. [PubMed] [Google Scholar]
- Norris R. M., Caughey D. E., Mercer C. J., Scott P. J. Prognosis after myocardial infarction. Six-year follow-up. Br Heart J. 1974 Aug;36(8):786–790. doi: 10.1136/hrt.36.8.786. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rechnitzer P. A., Sangal S., Cunningham D. A., Andrew G., Buck C., Jones N. L., Kavanagh T., Parker J. O., Shephard R. J., Yuhasz M. S. A controlled prospective study of the effect of endurance training on the recurrence rate of myocardial infarction. A description of the experimental design. Am J Epidemiol. 1975 Nov;102(5):358–365. doi: 10.1093/oxfordjournals.aje.a112174. [DOI] [PubMed] [Google Scholar]
- Rosenman R. H., Brand R. J., Jenkins D., Friedman M., Straus R., Wurm M. Coronary heart disease in Western Collaborative Group Study. Final follow-up experience of 8 1/2 years. JAMA. 1975 Aug 25;233(8):872–877. [PubMed] [Google Scholar]
- Sackett D. L., Haynes R. B., Gibson E. S., Hackett B. C., Taylor D. W., Roberts R. S., Johnson A. L. Randomised clinical trial of strategies for improving medication compliance in primary hypertension. Lancet. 1975 May 31;1(7918):1205–1207. doi: 10.1016/s0140-6736(75)92192-3. [DOI] [PubMed] [Google Scholar]
- Shapiro S., Weinblatt E., Frank C. W., Sager R. V. Incidence of coronary heart disease in a population insured for medical care (HIP): myocardial infarction, angina pectoris, and possible myocardial infarction. Am J Public Health Nations Health. 1969;59 (Suppl 6):1–101. doi: 10.2105/ajph.59.suppl_6.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Weinberg S. L. Natural history six years after acute myocardial infarction. Is there a low-risk group? Chest. 1976 Jan;69(1):23–28. doi: 10.1378/chest.69.1.23. [DOI] [PubMed] [Google Scholar]
- Wilhelmsen L., Sanne H., Elmfeldt D., Grimby G., Tibblin G., Wedel H. A controlled trial of physical training after myocardial infarction. Effects on risk factors, nonfatal reinfarction, and death. Prev Med. 1975 Dec;4(4):491–508. doi: 10.1016/0091-7435(75)90035-3. [DOI] [PubMed] [Google Scholar]