

Abstract
This paper presents a survey of side impact trauma-related biomedical investigations with specific reference to certain aspects of epidemiology relating to the growing elderly population, improvements in technology such as side airbags geared toward occupant safety, and development of injury criteria. The first part is devoted to the involvement of the elderly by identifying variables contributing to injury including impact severity, human factors, and national and international field data. This is followed by a survey of various experimental models used in the development of injury criteria and tolerance limits. The effects of fragility of the elderly coupled with physiological changes (e.g., visual, musculoskeletal) that may lead to an abnormal seating position (termed out-of-position) especially for the driving population are discussed. Fundamental biomechanical parameters such as thoracic, abdominal and pelvic forces; upper and lower spinal and sacrum accelerations; and upper, middle and lower chest deflections under various initial impacting conditions are evaluated. Secondary variables such as the thoracic trauma index and pelvic acceleration (currently adopted in the United States Federal Motor Vehicle Safety Standards), peak chest deflection, and viscous criteria are also included in the survey. The importance of performing research studies with specific focus on out-of-position scenarios of the elderly and using the most commonly available torso side airbag as the initial contacting condition in lateral impacts for occupant injury assessment is emphasized.
Keywords: Elderly population, Injury criteria, Fragility, Dynamic response, Side airbag
1. Introduction
Advancements in automotive designs around the world are driven by factors such as research, public awareness, government standards, crashworthiness tests and incorporation of safety features (e.g., airbag). The industry routinely plans and designs newer vehicles a few years in advance with different styles and enhanced safety systems built to current government standards. Frontal and side impact airbags, newer technological additions in the last decade, are meant to increase safety performance. Frontal airbags were introduced as an option to the vehicle fleet in the United States (US) long before regulations were enforced. Although these processes offer emerging technologies to the consumer, lack of immediate real-world field data on the efficacy of such improvements has affected the consumer, industry, and government. It is important to recognize that the negative impact of frontal impact airbags on the consumer was known primarily through field and anecdotal investigations through the mid-1990s. These emerging data showed the occurrence of severe or fatal trauma to the pediatric population (Kleinberger et al., 1998). Injuries were attributed to the aggressive nature of airbags, particularly for out-of-position (seated in close proximity) occupants. The automotive fleet now uses second-generation (less aggressive) frontal airbags. As a precautionary measure for frontal impact protection, late model vehicles include an option for the consumer to deactivate the airbag on the passenger side with a switch, for a lightweight front seat occupant. A review paper published in 2005 discussed the field performance of frontal airbags in frontal crashes (Kent et al., 2005). Side airbag technology was introduced much more recently than frontal airbags, appearing in the vehicle fleet only since 1996.
Side airbags are drawing the attention of the automotive industry, consumer and governmental regulators. Real-world field data are primarily anecdotal, principally because side airbags (SABs) are still nascent and their efficacy is still unknown. Studies synthesizing data from individual cases are limited. McGwin et al. using the US National Automotive Sampling System (NASS) files for the years 1997–2000, concluded the following regarding SAB efficacy (McGwin et al., 2003). “Front seat occupants of vehicles with SABs had a risk of injury similar to that of occupants of vehicles without SABs.” Age and gender did not affect the association. However, the following assumption regarding SAB use was made in the study: “vehicles for which SABs are optional equipment were considered to be equipped with SABs.” Support for the validity of this assumption was not reported. In any model year, not all vehicles with SABs as optional equipment will be sold with this technological feature. Bazarian et al. using 2000 NASS files, studied 187 occupants with brain injuries, out of which 62 occupants were in side impacts (Bazarian et al., 2004). The statement “side impact airbags may reduce risk of brain injury in lateral impact collisions,” was not supported because raw data included less than 1% of occupants in vehicles equipped with SABs. In a recent study, Yoganandan et al. analyzed 61 side impact cases with SAB deployments in the NASS database, and underscored the need for additional investigations to determine efficacy (Yoganandan et al., 2005a, b).
This review focuses on the driver as the primary occupant; consequently, the growing pediatric population is not relevant. As might be expected, the analyses focus on the elderly/older population due to factors such as estimated rapid growth of this population in the future, their increased fragility, co-morbid factors contributing to differences in the treatment regimen compared to the younger population and the use of the younger adult, i.e., 45-year-old, dummy in current crashworthiness evaluations and regulatory standards around the world. Existing biomechanical knowledge and injury criteria are presented following a discussion of epidemiological and clinical aspects. Conclusions are drawn emphasizing the need for biomedical research with a focus on the elderly population and the injury mitigating characteristics of SABs for occupant protection in motor vehicle environments. References are made to recent and pertinent literature. In the interest of maintaining focus, the current paper surveys findings from intact human cadaver (also called post mortem human subject, PMHS) investigations.
2. Involvement of the elderly population
While the World Health Organization uses 65 yr of age as the cut off for the older group, a clear definition does not exist in the biomechanical literature with particular reference to automotive injuries and crash-worthiness. Vehicular occupants including the driver have been defined to as elderly when the age exceeds 70, 65, 60, or 50 yr—termed ‘third agers’ (Augenstein 2001; Green 2001; Lupton 2001; NCSA 2001; Stutts 2001). Some biomechanical studies interpret the cut off to be 40 yr (Viano et al., 1989a). Older people will account for the largest increase in our population in the coming years due to aging baby boomers. Lupton (2001) estimated that there are over 70 million people older than 50 yr of age, and that is the fastest growing segment in the US (Lupton 2001). Driving motor vehicles is not restricted to any adult age group (except for health issues). It is estimated that 50 million people over 65 yr of age will be eligible to drive by 2020. The 2002 study by Lyman et al. reported that drivers 65 and older account for more than one-half of the total increase in fatal crashes and approximately 40% of crash involvements (Lyman et al., 2002). Therefore, older drivers have increased disproportionately to the increase in the general population.
Today's older Americans are active, healthy and wealthy. By the year 2005, 1.7 billion baby boomers worldwide will be over 45 yr of age, 66 million Americans will be over 55 years of age, and they will own 70% of US dollars and 50% of discretionary income. A total of 41% of all new cars and 48% of all luxury cars are purchased by people over 50 yr of age (Lupton, 2001; Vala, 2001). According to the November 2001 US Department of Transportation (DOT) estimates, more than 25 million people are 70 yr and older (NCSA 2001). In 2000, this group was 9.1% of the US total population, compared with 8.5% in 1990. From 1990 to 2000, the older segment of the population grew nearly twice as fast as the total population. There were approximately 19 million older licensed drivers in 2000, representing a 36% increase from 1990. Once in a crash, older drivers are more likely to be seriously injured or sustain fatalities, due to increased fragility; in addition, they have increased hospital costs, are more likely to receive rehabilitative service and contribute to an enhanced morbidity (McCoy et al., 1989; Dulisse 1997; Zhang et al., 2000; Read 2001). Traffic fatalities to this population are second only to the 16–20 yr group. For male drivers, fatality rates increased from 27 per 100,000 for the 70–74 yr group to 41 per 100,000 for the 85+ yr group. A Canadian population-based cross-sectional study published in 2000 by Zhang et al. reported similar results (ratios of 1.37, 1.42 and 2.26 for drivers aged 70–74, 75–59 and 80+ yr compared to the 65–69 yr baseline) (Zhang et al., 2000). Thus, biomedical safety engineering research targeting this group of our population is needed.
3. Side crashes in the elderly group
Bedard and co-authors in 2002 analyzed 1975–1998 Fatality Automotive Reporting System (FARS) database and found 31% of crashes to be side impacts (Bedard et al., 2002). Zaouk et al. analyzed the 1988–1997 NASS and FARS databases wherein approximately 920,000 occupants were exposed to side crashes and accounted for 11,300 fatalities (Zaouk et al., 2001). For vehicle-to-vehicle side crashes, ten and two o'clock positions appeared to be the most harmful with about 48% of total crashes contributing to 56% of MAIS = 3+ injuries; three and nine o'clock were the next detrimental positions with 39% of injuries. AIS refers to the abbreviated injury scale: 0—none, 1— minor, 2—moderate, 3—serious, 4—severe, 5—critical, 6—maximum and 9—unknown; MAIS refers to the maximum AIS (The Abbreviated Injury Scale (AIS), 1990). Using data from Canadian crashes involving 8839 fatally restrained occupants, Green et al. showed that lateral collisions contribute to approximately 50% of the ensemble (Green et al., 1994). Other factors contributing to trauma in the older group are described below.
3.1. Human factor
Drivers over 65 yr of age have a higher than average crash rate at intersections during turning maneuvers (1.3 times the average for all age drivers) (Moore et al., 1982). The incidence increased in rural intersections (1.5 times). Older drivers reportedly have an appreciably lower than average crash involvement rate with alcohol use, skidding, loss of control and crashes during darkness (Mourant 1979). Intersection maneuvers are reported to be hazardous for older drivers (Zhang et al., 1998). Drivers 65–69 yr of age were 2.3 times more likely to be involved in intersection crashes than drivers in the 40–49 yr group. This compares with 1.3 times the risk of crashes in other scenarios (Preusser et al., 1998). European studies have also reported involvement of older occupants with particular reference to intersection crashes (Foret-Bruno et al., 1983). Studies suggest changing human factors are causally related to the over-involvement of older drivers in side impacts. For example, age affects the judgment of the velocity of the approaching vehicle and distance (Scialfa et al., 1987).
3.2. Type of side impact
Contrary to the common notion of fatal crashes with higher involvement of younger drivers, multi-vehicle crashes have an over-involvement of older occupants (Viano et al., 1989a). The study projected that occupants over 40 yr of age with serious to fatal injuries in side impacts account for 50% of all those injured in such crashes. Using the 1975–1998 FARS data, Bedard et al. reported that driver-side impacts double the odds ratio of fatality compared to frontal impacts (Bedard et al., 2001). Consequently, the primary focus of injury research should be on this mode of impact and the nearside occupant.
3.3. Impact severity
Fildes et al. in an analysis using the Australian database, revealed an average change in velocity (ΔV) of 9.7 m/s for hospitalized and fatal occupants in side impacts (Fildes et al., 1994). Thomas and Frampton using the United Kingdom (UK) 1992–1998 database reported the median ΔV for MAIS = 3+ survivors to be 9.2 m/s for struck side occupants in car-to-car or carto-wide roadside object impacts and 5.3 m/s for collisions with narrow objects (Thomas and Frampton 1999). Using NASS 1995–1998 data, Zaouk et al. reported in 2001 that 60% of vehicle-to-vehicle or vehicle-to-narrow object crashes have a ΔV <10:7m/s for MAIS = 3+ injuries (Zaouk et al., 2001). The authors of this study concluded that there might be a larger opportunity for protection in the low crash severity.
3.4. Injured body regions
Studies in the 1980s reported specific body regions (e.g., head, chest) injured in side crashes. A study using the NASS data reported that approximately 40% of all crashes are side impacts (Rouhana and Foster, 1985). This study found near-side occupants to experience three times the incidence of serious or immediately fatal injuries compared to far-side occupants, serious injuries to be three to ten times more likely with intrusion into the passenger compartment, and head and neck injuries to be the most prevalent among immediately fatal injuries. Similar results were also reported from other NASS analyses (Warner et al., 1989). Head and neck injuries accounted for more than one-half of immediately fatal injuries, with chest injuries contributing to the remaining 50%. These authors attributed side impact injuries to the head passing through the side window opening and contacting either the lower window frame or parts of the oncoming (bullet) vehicle. As a countermeasure, the authors discussed the potential advantages of a supplemental inflatable restraint system, i.e., SABs. Because no such systems were in the vehicle fleet at that time, it was not possible to evaluate the injury-mitigating characteristics of SABs.
In 1998, passenger vehicle side impacts resulted in 9482 fatalities (Lund, 2000). In 1999, Thomas and Frampton found that the torso and head were the most common sites of AIS = 4+ injuries (fatal and non-fatal), while those seriously injured drivers also commonly sustained AIS = 2+ injuries to the legs, head and arms (Thomas and Bradford, 1989). During an investigation of side crashes between 1988 and 1992, an Australian study reported that the head and chest are most frequently injured at AIS = 3+ levels (Fildes et al., 1994). These national and=international studies, although in varied environments, underscore the need to include the head and chest in an evaluation of emerging technologies, particularly SABs.
Current US side impact Federal Motor Vehicle Safety Standards (FMVSS 214) do not include specific injury criteria for the head although the lateral impact new car assessment program (LINCAP) includes a warning if the head injury criterion (HIC) exceeds the threshold of 1000. Side impact regulations in the US use two acceleration-based criteria: one for the chest and the other for the pelvis. The thoracic trauma index (TTI) is defined using peak accelerations of the lower spine and the maximum accelerations between the fourth and eighth ribs. In regulatory tests, a TTI value of 85 for four-door and 90 for two-door passenger vehicles, and a peak pelvic lateral acceleration of 130g are the thresholds for these body regions. The present trend in SAB systems is targeted to both chest and head protection. These issues are discussed later.
A significant body of knowledge about occupant injury in real-world side impacts in the 1990s came from crashes involving vehicles primarily of the 1980s design (Haddak et al., 1991; Lestina et al., 1991; Fildes et al., 1994; Hassan et al., 1995). Reiff et al. in 2001 indicated SABs to be an option to ameliorate trauma (Reiff et al., 2001). Lyman et al. in 2002 stated, “Further research is needed on vehicle modifications to prevent injuries and deaths due to frailty. Improvements in vehicle crash-worthiness and restraints, such as tailoring airbag deployments to the characteristics of individual older occupants, should provide better protection to the fragile bodies of older occupants involved in crashes” (Lyman et al., 2002). Assessment and mitigation of trauma specific to the elderly, and SAB in lateral crashes are areas of critical importance to current and future motor vehicle design. As explained below, studies focusing on injury criteria are lacking for this group of the population.
4. Existing biomechanical knowledge and injury criteria
Lateral impact protection depends on managing the magnitude and distribution of dynamic forces applied to the occupant during the crash. The dynamic force may be delivered due to the interaction of the occupant with the intruding vehicle structure. The interior surface design of the side structure depends on knowledge of human body biomechanical characteristics in lateral impact, particularly the head, neck and torso, and the development of protective systems and test devices (Melvin 1994). The former is achieved by understanding human tolerance and defining injury criteria. The latter is achieved by the application of this knowledge to develop biofidelic dummies applicable to all populations, and by design and evaluation of safety-engineering systems such as SABs. A significant number of tests have concentrated on quantifying responses and identifying injuries to the chest, abdomen and pelvis. Traditional approaches to quantify responses of the human body secondary to lateral impacts include experimental testing of intact PMHS using full-scale vehicles, free-falls, pendulum/impactors or sleds. Isolated components such as hemi-pelvis and rib tests have delineated elemental structural responses (Yoganandan and Pintar 1998; Beason et al., 2003). Side-impact investigations using each of these models are described below.
4.1. Full-scale vehicle tests
The principal advantage of these tests lies in the close approximation to the field environment because actual vehicles are used in addition to the interaction of vehicular interiors with PMHS. In this approach, intact PMHS placed in motor vehicles are impacted using a bullet vehicle (e.g., barrier). From 1982 to 1984, a series of 35 PMHS tests were conducted in Germany at 11–17 m/s using a moving deformable barrier and an Opel Kadett car body (Klaus and Kalleris, 1982; Klaus and Kalleris, 1983; Klaus et al., 1984). Injured body regions included the chest (rib fractures), abdomen (liver, spleen, kidney), cervical spine, skull and pelvis. Data from these tests were further analyzed in 1986 to confirm the biofidelity of the US-regulated side impact dummy and the applicability of TTI. A probability distribution of TTI was derived for AIS = 3–5 levels (Morgan et al., 1986). The next paragraph briefly describes types of probability analyses used in this area of crashworthiness research. In a later study, Pintar et al. compared sled test results from 26 intact PMHS tests and found that biomechanical tolerance measures (e.g., TTI) are closely correlated between full-scale vehicle-to-vehicle tests and deceleration sled tests (Pintar et al., 1997). Additional information regarding sled tests from this group of authors is provided later. Full-scale vehicle tests have not been systematically conducted using SABs to assess their responses and efficacy.
Different types of probability analyses are used in impact injury biomechanics. For example, Yoganandan et al. used the Weibull approach to establish risk of facial trauma in frontal impact; Pintar et al. used linear regression and survival analysis using the Cox proportional hazards model to derive risk curves for cervical spine injury from impact loading; Cavanaugh et al. used the logist method to obtain thresholds for thorax and pelvis in side impact; Yoganandan et al. used the maximum likelihood approach to determine injury tolerances of the foot and ankle complex to dynamic axial loading; and Kuppa et al. used analysis of variance (ANOVA), linear regression, logistic regression and multivariate analysis including the effects of interaction variables such as age, gender and impacting condition to determine the most appropriate statistical model to describe thoracic injuries from human cadaver side impact tests (Cavanaugh et al., 1990; Yoganandan et al., 1993; Yoganandan, 1996a, b, c, d; Pintar et al., 1998a, b; Kuppa et al., 2000). While such methods have unique applications, no specific procedure is considered standard in impact biomechanics; type of experimental data often dictates the particular methodology used for probability analyses.
4.2. Free-fall (drop) tests
These tests provide data such as force, deflection and acceleration. Depending on the region of impact and orientation of the surrogate, free-fall tests characterize the biomechanical response of the chest, abdomen or pelvis. For the chest region, an earlier study, reported in 1979, used 15 intact PMHS (25–70 yr) in free-fall impact onto padded or rigid force plates from a height of 0.5–2.03 m (3–6 m/s) and developed force-deflection corridors (Stalnaker et al., 1979). Half-chest compression of 35% represented the limit for AIS ≤3 rib injury. Compression correlated better to injury than chest acceleration. In the same year, Tarriere et al. conducted free-fall impact tests (from 3 m, ΔV = 8 m/s) using 16 intact PMHS and combined this analysis with previously cited results (Tarriere et al., 1979). For AIS ≤3 chest trauma, full chest compression limit was established at 30%. Peak force thresholds for AIS = 3 and 0 were 10.2 and 7.4 kN. For the abdominal region, Walfisch et al. conducted a study using eleven intact PMHS (45–68 yr) in free-fall lateral impacts at velocities of 4.4 and 6.3 m/s onto rigid or armrest-padded surfaces (Walfisch et al., 1980). For the pelvic region, in the years 1977–1979, 26 PMHS (25–71 yr) were tested in free-fall impact with varying orientations and boundary conditions (e.g., padding) (Fayon et al., 1977; Tarriere et al., 1979). Pelvic fracture tolerance ranged from 80 to 90 g.
4.3. Pendulum/impactor tests
These tests provide localized human body responses. The loading device (pendulum/impactor) imparts dynamic forces to the specific region (e.g., thorax) of the surrogate. For the thoracic region, Stalnaker et al. tested eight PMHS (16–77 yr, 6–13 m/s) using different boundary conditions and reported that rib fractures occurred at 9 m/s and 7.6 cm deflection, not at 6 m/s and 5.3 cm deflection as previously reported (Melvin et al., 1973). Robbins et al. used 18 PMHS to develop a relationship between AIS and rib fractures, called the BLUR criterion (Robbins et al., 1994). By conducting repeated tests on eight intact PMHS (54–80 yr), Cesari et al. found that the BLUR criterion was a poor correlate of thoracic injury (Cesari et al., 1981). Viano et al. conducted lateral impact tests using 14 intact PMHS (29–66 yr) and reported force-deflection data at 4, 7 and 9 m/s (Viano et al., 1989b). Corridors were developed for the chest, abdomen and pelvis. The following criteria represented a probability of 25% critical injury (AIS ≥5). For the chest: product of peak velocity and compression (VCmax = 1.5 m/s) and peak compression (Cmax = 38%), and for the abdomen: VCmax = 2.0 m/s and Cmax = 44% (Viano et al., 1989c). These variables were found to be better predictors of thoracic injury than dorsal spine accelerations. For the pelvic region, this study determined that pelvic acceleration was not an injury correlate, and therefore, the 25% critical injury risk was set at Cmax = 27%. Yoganandan et al. developed upper abdominal force–deflection responses using five intact PMHS (62–86 yr) at 4 m/s (Yoganandan et al., 1996d; Yoganandan et al., 1997b). In 1982, results were reported from 12 intact PMHS (56–89 yr) tests at 5–9 m/s using an impactor with and without padding materials (Nusholtz et al., 1982). Six subjects sustained injuries including pubic rami and ilium fractures without bilateral involvement. Peak forces and accelerations for fracture ranged from 3.3 to 13 kN and 40–135 g. Although this study identified potential variables such as initial position that may contribute to injury, research efforts examining effects of occupant position on side impact-induced injury have not been advanced. Physiological processes such as decreased mobility of the musculoskeletal system may interfere with normal (in-position) automotive seating. Consequently, abnormal or out-of-position effects coupled with SABs with particular reference to the older population should be investigated to advance side impact research.
4.4. Sled tests
These involve impact to PMHS that occurs following a short duration deceleration or acceleration during which the subject moves toward the wall similar to the real-world side impacted occupant. Velocity of the subject relative to the wall is the principal parameter and deceleration of PMHS against the wall depends on mechanical characteristics of the subject and the wall that may include energy absorbing systems such as SABs. These studies provide data such as acceleration, force and deformation of various body regions and assist in deriving secondary variables, such as TTI, for injury evaluations.
An early study tested seven intact PMHS (58–84 yr) at ΔV of 7, 9 and 12 m/s (Melvin et al., 1976). The impact surface configurations included a flat rigid wall and a contoured energy absorbing structure consisting of thorax and pelvis bolsters. Skull fractures occurred in rigid wall tests. At the highest velocity, bilateral skull fractures occurred with hemorrhage of the right temporal and parietal lobes of the brain. The authors stated that padding “did not change the injury level of the thorax at the medium velocity and actually raised it slightly in the low velocity test” (Melvin et al., 1976). Padding was most effective in decreasing chest accelerations at lower velocities. In contrast, padding decreased pelvic accelerations at higher and increased pelvic accelerations at the lower velocities, raising questions about the effectiveness of the chosen padding in mitigating chest and pelvic injuries. Because SABs affect the kinematics of the torso including the chest and pelvis, there may be a different spectrum of injuries to other body regions. Therefore, investigations with SABs should be conducted, with specific reference to the older population due to increased frailty.
During the last decade, data were published from 19 deceleration sled tests. Initial tests were conducted at 7–10 m/s using 17 PMHS (37–68 yr). PMHS seated on a Heidelberg-type seat fixture, impacted a flat rigid wall, an unpadded wall with 150 mm pelvic offset, or a flat padded wall with different padding materials. The load wall was configured to measure shoulder, thorax, abdomen and pelvic forces. Although head and neck injuries were not published, autopsy results were later reported on the pelvis, shoulder, thorax and abdomen (Cavanaugh et al., 1990; Cavanaugh et al., 1993; Irwin et al., 1993; Zhu et al., 1993; Cavanaugh et al., 1996; Koh et al., 2001). To date, head–neck injuries in side impact sled tests have received little attention by biomechanical researchers.
Thoracic injuries were more severe with stiff padding (mean MAIS = 4.7) than with soft padding (mean MAIS = 2.3) or unpadded walls (mean MIAS = 4.0). The authors commented that a reduction in crush strength results in MAIS = 2 or less if 100 mm or more of padding is used, and “this thickness is probably only practically obtainable using a side-door airbag” (Cavanaugh et al., 1992). These authors did not consider using airbags as a boundary condition for interactions with PMHS presumably because SABs were not in the vehicle fleet during this period.
Abdominal injuries were more severe with stiff padding than soft padding and unpadded impacts. The study suggested that abdominal or lower rib cage injury may occur with 138 kPa padding at 9 m/s, while a reduction of stiffness to 69 kPa should mitigate trauma (Cavanaugh et al., 1996). As indicated earlier, crash-worthiness tests do not have established abdominal injury criteria for side impacts despite advancements in this area for the quantification of abdominal injuries. In 2001, Yoganandan et al. reviewed the abdominal injury studies from clinical, epidemiological and biomechanical aspects, with citations to more than 200 references (Yoganandan et al., 2001a). As a first step, these studies may be used to introduce metrics for injury assessments.
Pelvic fractures resulted from thinner padding (75 mm) while thicker (100–150 mm) padding mitigated trauma (Cavanaugh et al., 1990). Peak impact force thresholds for the fifth, 50th and 95th anthropometry were (Cavanaugh et al., 1993): AIS = 2+ shoulder injuries: 2.52, 3.5 and 4.25 kN; for AIS = 4+ thorax injuries or abdominal (visceral) injuries: 2.16, 3.00 and 3.64 kN; and pelvic fracture tolerance: 5.77, 8.00 and 9.71 kN. These data are lower when compared with intact PMHS pendulum impact tests (25% probability of MIAS = 4+ to be 5.48 kN for thorax, 6.73 kN for abdomen, 12.0 kN for pubic rami fracture) (Viano 1989). The thresholds are also lower when compared with European data (pelvic tolerances: 4.38, 10.16 and 15.18 kN for fifth, 50th and 95th anthropometry) (Cesari and Ramet, 1982). Peak force however, may not be the most appropriate injury criterion. Thus, a clear consensus does not exist in literature.
Using prior experience of conducting frontal impact sled tests with advanced instrumentation (chestband, introduced in 1989) with different restraint systems including airbags (published from 1991 to 1997), Yoganandan, Pintar and associates conducted side impact sled tests using dummies and intact PMHS (Eppinger et al., 1984; Yoganandan et al., 1991; Yoganandan, 1994a, b; Yoganandan et al., 1995; Pintar et al., 1996; Yoganandan et al., 1996b; Pintar et al., 1997; Kuppa et al., 2000; Maltese et al., 2002; Yoganandan et al., 2002). Post mortem human subjects were obtained; radiographs of the entire body were taken; triaxial accelerometers were fixed to the spinous processes of the upper and lower thoracic column and sacrum; uniaxial accelerometers were fixed to the left lateral portion of ribs four and eight to record medial to lateral accelerations; a uniaxial accelerometer was fixed to the sternum to record anteroposterior acceleration; and three 40–59 channel chestbands were instrumented under the axilla at the rib-four level, xyphoid process and rib-ten level (Fig. 1).
Fig. 1.
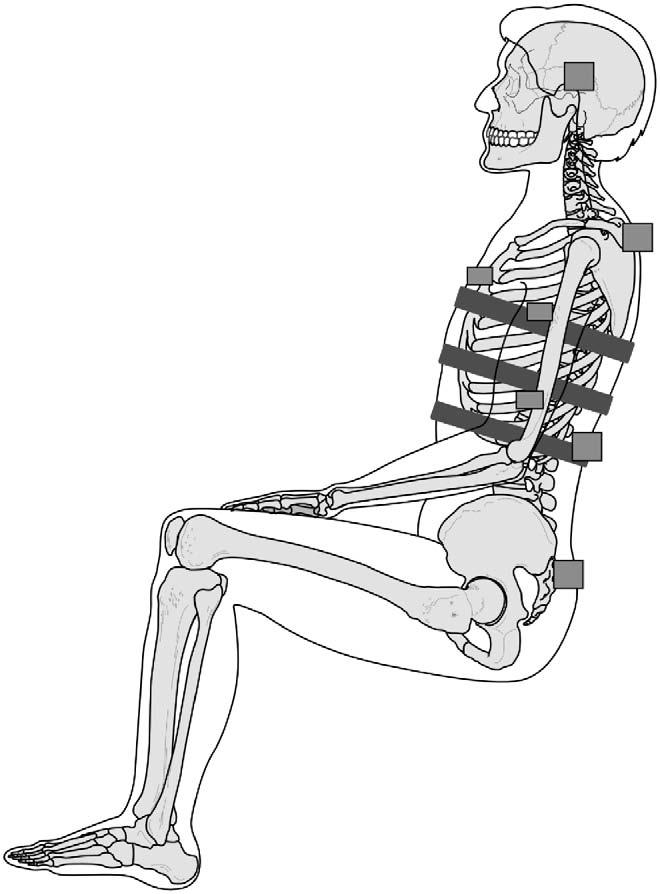
Instrumentation used in PMHS tests. Squares show accelerometers mounted to the upper and lower thoracic spinous processes, ribs and head. Three inclined rectangles show the chestbands affixed at the three levels to obtain time–deformation chest contours from which injury criteria were computed.
The PMHS was seated on a Teflon-coated bench with horizontal tubing to support the back and head; the bench had a footrest. The load wall consisted of four plates instrumented with eleven load cells (Fig. 2). The vertical height of the upper edge of the thoracic plate was set at 400 mm, preventing shoulder contact. This dimension was chosen to represent the average window-sill of passenger cars. The specimen contacted the initially configured load wall (padded, rigid or offset) without any significant changes in the anatomical interrelationships between the various body segments. The entire pelvis up to the level of the iliac crest of PMHS contacted the pelvic load plate. The lower regions of the ribcage were exposed to the abdominal load plate. The thoracic load plate engaged the middle ribcage. Tests were conducted at ΔV of 7 and 9 m/s. Flat rigid wall, flat wall with 10 cm of Ethafoam LC 200 padding and rigid wall with pelvic, abdominal or thoracic offset of 11 cm were the boundary conditions in these tests. Injuries were graded using the 1990 version of the AIS rating scheme (AIS, 1990).
Fig. 2.

Sled buck set-up showing the load cells used to obtain thoracic, abdominal and pelvic forces (Pintar et al., 1997; Yoganandan and Pintar 2005).
Data analysis included computations of deformation contours at each 1 ms time step for the three levels at which chestbands were used. Cmax, TTI and TTI*Cmax were computed. Parameters such as p-value and χ2 of the logistic regressions were extracted to determine the best-fit parameter that described injury at different AIS levels. Initial results from 26 PMHS tests indicated the 50% probability of AIS ≥4 injury to be: TTI 169, Cmax = 30% (full chest width), TTI*Cmax = 58 (Pintar et al., 1997). At 25% and 50% probability of AIS ≥4, TTIs were 151 and 169, respectively (Fig. 3). The product of TTI and chest compression was the best predictor, although other candidates were excellent predictors as shown by the p and χ2 values (Table 1). From an additional 17 PMHS tests using a real vehicle, TTI were 150 and 170 for the same probabilities and injury levels as the sled tests (Morgan et al., 1986). The excellent agreement between TTI values obtained from sled tests (Pintar et al., 1997) and tests using real-world vehicles (Morgan et al., 1986) validated the use of a single sled for simulating side impacts and analyzing injuries and injury biomechanics. This proven deceleration testing methodology can be used to conduct sled tests with PMHS of varying adult age groups with SAB deployments to assess their efficacy for injury reduction in the elderly population.
Fig. 3.
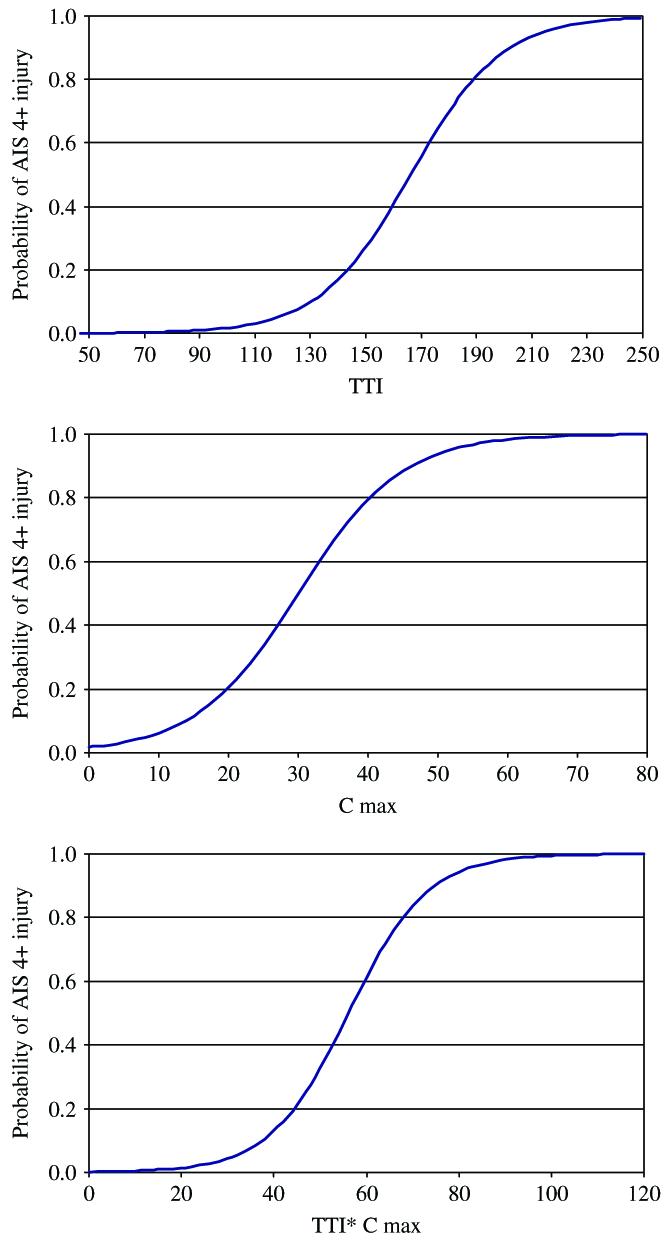
(a) Logistic regression output for TTI injury criteria (Pintar et al., 1997). (b) Logistic regression output for Cmax injury criteria (Pintar et al., 1997). (c) Logistic regression output for TTI*Cmax injury criteria (Pintar et al., 1997).
Table 1.
Statistical analyses of various injury criteria (Pintar et al., 1997)
| Injury criteria | Chi-square | p-Value | 25% Probability AIS ≥4 | 50% Probability AIS ≥4 |
|---|---|---|---|---|
| Cmax | 5.488 | 0.0191 | 22 | 30 |
| TTI | 12.014 | 0.0005 | 148 | 166 |
| TTI*Cmax | 13.961 | 0.0002 | 43 | 54 |
In 2002, Maltese et al. derived corridors applicable to the 50th percentile male (equivalent to a 45-year-old) from these PMHS data (Maltese et al., 2002). A total of138 time–history plots were derived for the flat wall, abdomen, thoracic and pelvic offsets under padded and rigid initial impacting conditions at ΔVs of 7 and 9 m/s. Thoracic, abdominal and pelvic forces; upper and lower spinal and sacrum accelerations; and upper, middle and lower chest deflections for all initial conditions were considered during corridor development. These findings represent a battery of tests valuable in the development of biofidelic anthropomorphic test devices and evaluation of SABs. Although all tests were scaled to the mid-size male (50th percentile) using the equal-stress–equal-velocity approach, no attempt was made to classify corridors as a function of age, and therefore, the applicability of these results to the elderly population needs further research. It should be emphasized that SABs were not implemented in these tests. However, these analyses indicate that sled testing methodology is relevant and important in the evaluation of vehicular crashworthiness. In a recent study, Yoganandan et al. developed corridors specifically applicable to the fifth percentile female (Yoganandan and Pintar, 2005).
Kuppa et al. conducted statistical analyses using various injury metrics and demographics (Kuppa et al., 2000). Techniques such as ANOVA and linear and logistic regressions were used. Parameters evaluated included TTI, Cmax, peak force, energy and energy rate. Subject age influenced injury severity while gender and body mass had little influence. Fig. 4 shows a logistic regression plot of chest deflection as a function of MAIS = 3 probability of injury for the “standard 45-year-old” occupant and the elderly (60-year-old) occupant. Tests with SAB deployments were not available, and therefore, their statistical predictions may have to be revisited subsequent to additional data acquisition.
Fig. 4.
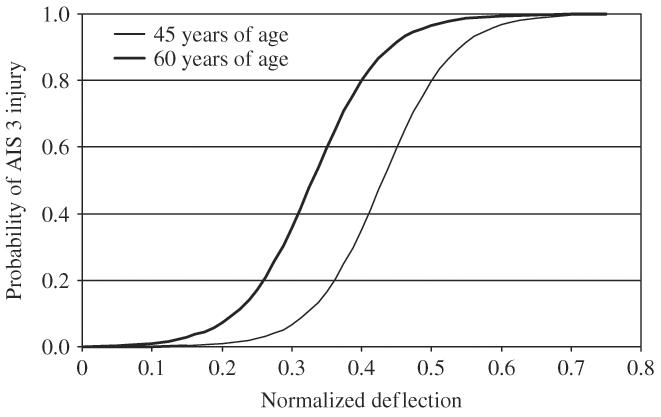
Logistic regression output for the probability of MAIS = 3 injury (ordinate) as a function of chest deflection; data based¼on Kuppa et al. (2000).
4.5. Injury criteria
Although various injury criteria have been evaluated for side impacts, in regulatory crashworthiness tests, as indicated earlier, the US FMVSS 214 for side impact specifies the determination of TTI and pelvic acceleration, and values of 85g and 90g for TTI are specified as thresholds for four- and two-door vehicles, and 130g is the limit for the pelvic acceleration (NHTSA 2005). These data are recorded in side impact dummies (SID) placed in the driver and left rear seats in actual cars. A more recent dummy, ES-2re, is being considered for future crashworthiness tests because of its enhanced biofidelity compared to SID (Federal Register, 2004). The pole test is also being considered (2004). US FMVSS 214 specifies impacting the target vehicle oriented at an angle of 27° and impacted on the left side at a velocity of 54 km/h. Consumer information LINCAP tests use an impact velocity of 62 km/h for the moving deformable barrier. The star rating is independently calculated from TTI from the two dummies in the LINCAP test. Table 2 shows the star ratings, probability of injury, and associated TTI values. Pelvic accelerations exceeding 130g, although not included in the star rating, receive a remark indicating the potential for trauma. Specific limits for head injury assessment do not exist in the current LINCAP test. However, since April 2002, the US National Highway Safety Administration (NHTSA) has noted safety concerns not reflected in the star-rating. One of those is specific to head injuries in the LINCAP test. A safety concern remark is introduced informing the consumer about the potential for head injury in tests with the HIC exceeding 1000, although probabilities are not attached with respect to specific HIC values. Because of space limitations, injury criteria adopted in other countries are not described in this survey article.
Table 2.
Summary of injury criteria used in the star-rating scheme for side impacts
| # Of stars | Injury probability data (chance of serious injury to the torso) |
TTI |
|---|---|---|
| 1 | 5% or less | ≤57 |
| 2 | 6–10% | >57 and ≤72 |
| 3 | 11–20% | >72 and ≤91 |
| 4 | 21–25% | >91 and ≤98 |
| 5 | 26% or greater | >98 |
5. Elderly and SAB issues
5.1. With regard to age
It is well known that bone tolerance to mechanical input decreases with increasing age. The elastic modulus and tensile strength decrease after approximately 40 yr (Lindahl and Lindgren 1967; Yamada 1970; Currey and Butler 1975; Currey 1979; Wall et al., 1979). Between 40 and 70 yr, bone loss occurs gradually; after 70 yr, the rate of loss increases (Goldstein et al., 1993; McCalden et al., 1993). The decrease is manifested by increases in porosity and plays a key role in the decrease in bone mineral density (BMD) (McCalden et al., 1993). Spine and hip are frequent BMD measurement sites in a clinical environment (Wilson 1977; Asch 1997; Yoganandan et al., 2006). Fracture toughness also decreases by approximately 55% between 27 and 80 yr (Bonfield et al., 1985). In other words, the strength of young mature skeletal structures is approximately twice that of 80-year-olds. The strength of human vertebral bones decreases by approximately 56% between 20–80 yr (Mosekilde and Mosekilde 1986). Other studies have also shown that the material properties of the human bones decrease with increasing age (Yamada 1970; Burstein et al., 1976; Hayes 1991; Zioupos and Currey 1998). Testing of human ribs is also available (Granik and Stein 1973; Schultz et al., 1974; Yoganandan and Pintar, 1998; Kimpara et al., 2003). During an analysis of 42 side impact PMHS tests in 1983, Marcus et al. showed that the number of rib fractures (approximately 0.2 fractures ribs/year) and injury severity (0.025*AIS/yr) increase with increasing age, emphasizing the fragility of older occupants (Marcus et al., 1983). Analysis of 26 PMHS tests conducted at velocities of 7 and 9 m/s without SAB revealed that the number of rib fractures and fractured ribs increases appreciably with age (Pintar et al., 1997; Kuppa et al., 2003). Data shown in Fig. 5 indicate that rib injuries increase at a higher rate for the older population than for the younger group, emphasizing the fragility of older occupants. Although the PMHS model is very useful for assessing rib fractures, assessment can also be extended to soft tissues, e.g., lung contusions. It can be implied that rib cage compromise may endanger organs housed within the cage including the great vessels. Pintar et al. reported hemothorax and unstable flail chest in PMHS sled tests. However, conclusive studies have not been conducted using SAB as the initial boundary condition. As discussed earlier, different research teams used PMHS with widely varying age to determine tolerance limits and injury criteria. Tolerances were expressed, e.g., as mean and standard deviations or logistic regression analyses for risk curves at different levels of severity. However, most studies combined adults without any classification by age group. In order to derive injury metrics specific to the elderly, it is important to incorporate demographic, physiological and/or biomechanical factors in experimental and analysis paradigms.
Fig. 5.

Comparison of rib fractures and number of ribs fractured from PMHS sled tests. Note the increase in trauma particularly at the high velocity for the older (≥60 yr) age group (Pintar et al., 1997; Kuppa et al., 2003).
Clinical outcome studies have shown that age is an independent predictor in blunt trauma, as documented by increased mortality and increased length of hospital stay (Shorr et al., 1989; Cameron et al., 1996; Bergeron et al., 2003). In 2003, Bergeron et al. found that elderly patients (>65 yr), admitted with rib trauma from a variety of sources including motor vehicle crashes and falls, had increased mortality due to skeletal injury (Bergeron et al., 2003). Even after accounting for comorbidities, elderly patients had higher mortality than younger patients. Bulger et al., stated: “despite similar injury patterns and injury severity, elderly patients (>65 yr) who sustain blunt chest trauma with rib fractures have twice the mortality and thoracic morbidity than younger patients” (Bulger et al., 2000). While the younger population had a “threshold” or plateau effect, the morbidity and mortality of older patients demonstrated a linear increase with the number of rib fractures. For each additional rib fracture, mortality increases by 19% and the risk of pneumonia by 27%. Taylor et al. compiled data from 37,762 patients admitted to 26 trauma centers and showed similar susceptibility of elderly patients (Taylor et al., 2002). Aging rates of human bones indicate that a significant turning point occurs in the aging process between 60 and 70 yr (Zhou et al., 1996). This study showed that with age, the tolerance reduction for soft tissues is similar to reductions for rib fracture tolerance from blunt and lateral loading experiments. Studies using individual bones and trabecular architecture evaluations have consistently showed thinning of the lattice arrangements to be a structural reason for decreased BMD and hence, strength (Pugh et al., 1972; Keaveny and Hayes 1993; Rho et al., 1995; Singer et al., 1995; Riggs, 2004). It should be noted that strength of bones, e.g., spinal vertebrae, correlates with compressive strength (Hansson et al., 1980; Hansson and Roos 1981). In addition, compressive load is a strong predictor of cycles to failure for osteoporotic vertebrae (Lindsey et al., 2005). Keaveny and Yeh indicated a need for large scale studies to describe the morphological effects of age for trabecular bone and hip, with an emphasis on mechanical assays to test the response under different loading systems (Keaveny and Yeh 2002).
5.2. Initial positioning (termed as orientation, posture, etc.)
As indicated in the Introduction, effects of initial occupant position on injury severity have significantly changed frontal airbag technologies. Particularly to the driver small in stature and sitting in close proximity to the steering wheel (termed out-of-position), first generation frontal airbags produced serious-to-fatal injuries, including upper cervical spine–head junction trauma (Kleinberger et al., 1998). As a consequence of this retrospective finding, newly designed second generation frontal airbags were implemented in the vehicle fleet beginning in 1998. Epidemiological studies reported that while frontal airbags protect the head and chest, lower extremity injuries have increased, and the pattern of injuries to the hip–femur complex has changed; specifically, the occurrence of pelvic–acetabulum complex fracture without femoral or knee injury (Yoganandan, 2001a, b). Recognizing this change, Yoganandan et al. underscored the importance of initial positioning in the determination of the mechanism of hip injury without distal femur fracture (Yoganandan, 2001b). This study showed that pelvic tolerance decreases to 6.8 kN with an initially flexed–adducted hip–femur–knee complex in contrast to the 10 kN tolerance with a straightened knee–femur complex for pure femoral bone trauma. Similar analyses of initial position effects on injury occurrence, mechanism and tolerance were advanced for the knee by Ewers et al., for the neck by Pintar et al. and Maiman et al., and for the lower extremity by Yoganandan et al. (Pintar et al., 1995; Yoganandan et al., 1996c; Yoganandan et al., 1997a, b; Pintar et al., 1998a, b; Yoganandan et al., 1999a, b; Ewers et al., 2002; Maiman et al., 2002). Such out-of-position analyses on changes in injury metrics and identification of injury as a function of occupant age are not available for side impacts.
5.3. Out-of-position in side impacts
As discovered from field experiences in frontal impacts with frontal airbag scenarios, a short stature occupant sitting in close proximity to the steering wheel poses enhanced risk of injury from deployment; normally seated occupants may be forced out-of-position by pre-crash events such as braking or hard maneuvering; some occupants drive in positions different from those considered normal (Lund 2000). In 2000, the SAB out-of-position injury technical working group (formed by the Alliance of Automobile Manufacturers, Association of International Automobile Manufacturers, Automotive Restraints Council and Insurance Institute for Highway Safety) remarked; “there have not been enough deployments to assess the out-of-position injury risk of SABs from accident data,” and the group viewed that “new systems should be designed according to these recommendations for further limiting out-of-position occupant injury risk largely because new technology is emerging that is expected to meet the guidelines while still providing side impact protection.” Based on the retrospective experience in frontal crashes, the International Standards Organization (ISO) defined out-of-position to evaluate frontal airbags. The side impact technical working group of the ISO identified out-of-positions for this crash mode particularly for child dummies and small female occupants (Lund 2000). However, this group emphasized that the issue of assessing SAB effectiveness was outside its mission, and recommended that new SAB systems be designed “for further limiting out-of-position occupant injury risk largely because the new technology is emerging.” Another study comparing results between PMHS seated in different positions but subjected to impacts to the greater trochanter observed differences in pathology and correlations with biomechanical parameters and further stated, “additional test parameters, such as subject configuration also affect comparisons between test results” (Nusholtz et al., 1982). Thus, it is important to conduct research and obtain data regarding the effects of out-of-position in side impacts.
Pintar et al. identified different out-of-position scenarios potentially harmful to the chest and head-neck regions from side impact airbags for the pediatric population (Pintar et al., 1999). However, effects of out-of-position on injury and biomechanics are yet to be quantified for the adult population in side impacts. Since SABs deploy earlier in side impacts than frontal airbags in frontal impacts, positioning may be an important factor in the lateral mode in vehicles equipped with SABs. The type of SAB may affect occupant kinematics; the area of coverage is a function of airbag type; and torso combined with head bags differ from separate torso and curtain airbags and torso-only airbags. Yoganandan et al. described injury patterns and associated crash variables as a function of SAB type in side impacts using 1997–2004 NASS data (Yoganandan et al., 2005a, b). These retrospective studies do not contain information on occupant positioning. Therefore, out-of-position issues need a careful evaluation of field data coupled with occupant kinematics and biomechanical analysis.
Side airbags are entering the vehicle fleet at a rapid rate. In 2002, NHTSA reported the growth of annual sales for cars, light trucks and vans with SABs from 1996 to 2001 (NHTSA, 2002a, b, c). In 2001, 36% of cars and 15% of light trucks and vans sold in the US had SABs, compared to very small numbers just a few years before. According to NHTSA, the number of vehicle models sold in the US increased from 230 in 2000, to 251 in 2001, to 276 in 2002 (NHTSA, 2002a, b, c). Compared to model year 2000 wherein 41% vehicles were equipped with SABs (thorax or thorax and head bags) and 13% vehicles with head airbags, in 2002, these percentages increased by approximately 50%. Typically, SABs are installed as thorax or torso airbags alone, thorax–head airbag (also termed combination airbags) or separate thorax airbag and head airbag (inflatable tubular structure or curtain). Fig. 6 summarizes trends in the type of SAB installed in passenger cars and light trucks/sports utility vehicle (SUV)/minivans in the US from 1996 to 2004. Data were obtained from US side impact tests and websites providing data on vehicles with SABs showing type and availability, i.e., standard or optional. A general trend in the increasing nature of SAB use can be appreciated. Fig. 7 shows the data based on the type of SAB. As can be seen, torso/head airbags, i.e., combination airbags, are on the decline in contrast to the torso alone or torso/curtain airbags that show an increasing trend. In model year 2004, torso SABs outnumbered the combined torso/head airbag system by a ratio of 3 to 1. Therefore, it appears that torso airbags will continue to increase in the vehicle fleet. Because curtain airbags are effective in decreasing HIC and do not have occupant positioning issues, it is necessary to conduct studies with torso airbags to assess their efficacy in preventing torso injuries, particularly in the out-of-position scenario.
Fig. 6.
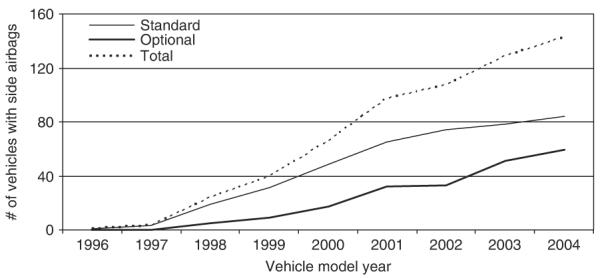
Side airbag availability as a function of year.
Fig. 7.
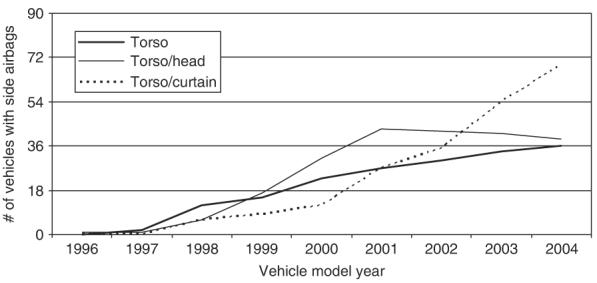
Type of side airbag as a function of year. Torso–head is a combination airbag. Torso–curtain is two separate airbag system. Note the decline of the torso/head airbags with increasing separate torso/curtain airbags.
Very few studies have been conducted with SABs to demonstrate their interaction with human surrogates and potential injury mitigating characteristics. In 2002, Arbelaez et al. compared responses from dummies in full-scale vehicle tests with and without airbags (Arbelaez et al., 2002). This study simulated a SUV impacting a passenger car with and without SABs at ΔV of 15 m/s. Tests with the small-size female dummy (SID-IIs) produced approximately 50% higher VCmax results (with SABs) for ribs 2 and 3, while for rib 1, VCmax remained unchanged (Fig. 8), although head injury measures were significantly lower with SABs. In 2003, Kuppa et al. provided 7 m/s sled test data (summarized in Table 3) from four PMHS tests using two seat- and two door-mounted SABs (Kuppa et al., 2003). Three chestbands were used in each test (except in the first seat-mounted system). The airbag was positioned such that the in-position PMHS occupant contacted the airbag at the time of full deployment; the optimum situation for protection of the occupant from the airbag. This was accomplished by conducting a preliminary test without the surrogate to adjust the timing sequence for the airbag to obtain its full deployment position. Door-mounted airbag tests did not result in injury while the two seat-mounted airbag tests responded with AIS = 3 and 2 for the thorax, and one PMHS sustained pelvic trauma (AIS = 2). Although the sample size is small, these preliminary tests show that PMHS tests can be conducted using SABs as an impacting condition. These tests also indicate that all types of SABs do not always offer identical protection. It can be immediately observed that door-mounted airbags seem to offer better protection than seat-mounted airbags. This is most likely due to the larger size and more aggressive nature of the door-mounted bags. As learned from frontal airbags in the 1990s, occupant position and anthropometry affect field performance (Kent et al., 2005). Because a vast majority of SABs in the US originate in a seat-mounted design, it is important to focus studies on this type of airbag. Because such tests have not been conducted with out-of-position PMHS for the elderly driving population, it is important to pursue this line of research, and assess occupant safety with emerging technologies.
Fig. 8.
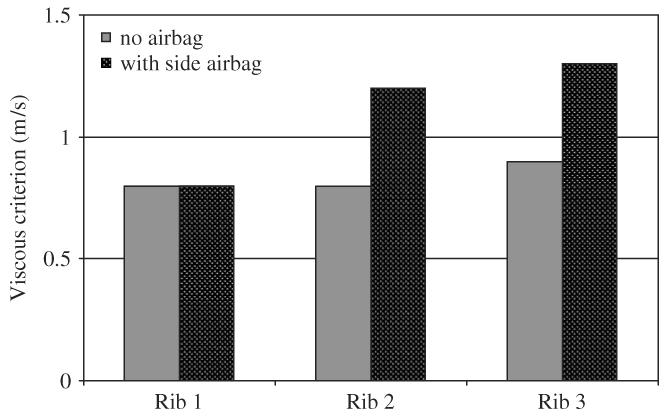
Comparison of viscous criteria at the three rib levels with and without side airbag. Note the approximate 50% increase VCmax in rib 2 (0.8–1.2 m/s) and rib 3 (0.9–1.3 m/s); rib 1 VCmax remained the same (Arbelaez et al., 2002).
Table 3.
Summary of PMHS sled tests with side airbags (Kuppa et al., 2003)
| ID | Age (yr) | TTI (g) | Upper Cmax (%) |
Upper VCmax (m/s) |
Middle Cmax (%) |
Middle VCmax (m/s) |
Lower Cmax (%) |
Lower VCmax (m/s) |
Pelvis Accel (g) |
Spine ASA (g) |
Thorax AIS |
|---|---|---|---|---|---|---|---|---|---|---|---|
| SM | 61 | 117 | 22 | 0.7 | 33 | 2.0 | — | — | 60 | 23 | 3 |
| SM | 70 | 146 | 12 | 0.2 | 19 | 2.9 | 35 | 3.0 | 51 | 37 | 2 |
| DM | 61 | 111 | 14 | 0.5 | 16 | 0.4 | 28 | 1.8 | 58 | 58 | 0 |
| DM | 60 | 137 | 20 | 0.4 | 25 | 0.4 | 18 | 0.5 | 53 | 16 | 0 |
SM and DM represent seat- and door-mounted airbags. Upper, middle and lower refer to data from three chestbands placed under the axilla at rib-four level, xyphoid process and rib-ten level.
It should be noted that in the 1990s, as frontal airbags were being more commonly introduced into the vehicle fleet, considerable research efforts were expended to understand the biomechanics of PMHS with frontal airbags. Post mortem human subject sled studies were conducted with varying combinations of airbags and different types of seatbelts (Yoganandan et al., 1994a, b; Yoganandan et al., 1995; Yoganandan et al., 1996b). The recently promulgated US FMVSS 208 used these studies as a basis (Kleinberger et al., 1998). Such studies have not been systematically conducted with SABs. Thus, a need exists for side impact occupant protection and following the 208 path appears to be prudent. Because out-of-position is critical for the lateral mode, it is also necessary to use positioning as a variable in the test matrix. A potential confounding factor is the availability and multiplicity of SAB systems. Side curtains are intended to protect the head, and seat-mounted SABs are primarily intended to protect the chest and pelvis. Seat-mounted SABs are more common than curtains, and even in the optional category in the US market, curtains come with seat-mounted thorax airbags. Because LINCAP tests have shown that side curtains are effective in protecting the head in lateral crashes (HIC considerably lower with curtains), it would be necessary to evaluate the efficacy of a seat-mounted airbag for torso protection when not accompanied by the curtain. This type of assessment eliminates changes in torso kinematics (if any) due to curtain deployment, and may conceivably preclude the benefits of a curtain assisting in the seat-mounted airbag for torso protection. The use of the seat-mounted airbag alone will provide conservative estimates of airbag efficacy.
As indicated in the Introduction, the present survey has focused on human cadaver experimental models. Physical models using anthropomorphic test devices (BIOSID, WorldSID with various modifications, EuroSID with modifications such as the ES2 and ES 2-re, SID IIs, etc.) are developed, upgraded and used in this area of research (Maltese et al., 2002; Yoganandan et al., 2002; Kuppa et al., 2003; Yoganandan and Pintar 2005). Experimental animal models are also used in side impact studies; e.g., Yoganandan et al. presented a review of models used for abdominal injury assessment (Yoganandan et al., 2001a). Similarly, various computational models have been used (Wismans et al., 2005). While cited references are not inclusive, these models also play a role.
The PMHS model is the best surrogate to replicate trauma, determine the biomechanical variables associated with trauma, and study the effectiveness of emerging technologies such as SABs to the older driving population. Under dynamic loading conditions, the mass and mass moment of inertia properties are essentially the same as those for the in vivo human. The PMHS model allows for direct invasive measurements that are difficult in other experimental models. A disadvantage of the cadaver model is the lack of muscle tone and physiological environment. In side impacts, however, because the effects of muscles are insignificant, SIDs have been developed based on PMHS data without adjusting for active musculature. This is particularly true with SABs because deployment times are very rapid (less than 20 ms after initiation of impact), and this time is insufficient for muscles to respond and redirect action in the in vivo situation. In other words, once side impact initiates, the central nervous system has little time to respond to the initiation; hence, changes in muscular activity needed to affect human response either do not occur or are insignificant. Other studies have underscored the secondary role of the muscle reflex contraction on kinematics (Stemper et al., 2005). It is well known in biomechanics that trauma occurs early during the impact event when acceleration/deceleration is most severe. From these perspectives, it is appropriate to use the intact PMHS as a model in side impact research.
6. Summary
Recent studies acknowledge increases in the role of the older population in motor vehicle use and underscore the urgent need to serve this group with technological advancements to ensure safety. Recognizing that current US FMVSS use the “45-year-old” side impact dummy for crashworthiness assessments, the need is further reinforced to include older age groups in the examination of emerging technologies (NHTSA, 2002a, b, c). Although human cadaver tests have used elderly specimens, injury-related data have not been systematically derived for this group. It is prudent to pursue this line of research focusing on side airbag technology as it applies to the elderly population. This is critical because human tolerance decreases and morbidity increases with increasing age. The out-of-position scenario in combination with the fragility of the older driver increases the risk of injury and fatality from impact.
Reasoning for the assessment of automotive safety in the elderly population is straightforward because a significant majority of studies in the past placed special emphasis on obtaining data pertinent to the younger population (regulatory standards around the world for this group). Using the proven methods discussed earlier, it should be possible to conduct biomechanically based studies specifically aimed at the elderly and side airbags, including out-of-position scenarios, to gather critically needed data to advance safety for this population. This research may open additional and new avenues for quantitative assessments in occupant safety and safety technology improvements in the motor vehicle environment. Both the industry and consumer will derive benefit from this research.
Acknowledgments
This study was supported in part by NIH Grant (R01AG024443) and VA Medical Research.
References
- Arbelaez R, Nolan J, Dakin G, Lund AK. Comparison of EuroSID-2 and SID-IIs in vehicle side impact tests with the IIHS barrier. Stapp. Car Crash Journal. 2002;46:397–415. doi: 10.4271/2002-22-0019. [DOI] [PubMed] [Google Scholar]
- Asch E. Interpreting bone mineral density reports: pitfalls and parameters. Internal Medicine World Report. 1997;12:24–27. [Google Scholar]
- Augenstein J. Aging and Driving Symposium. AAAM; Southfield, MI: 2001. Differences in clinical response between the young and the elderly. [Google Scholar]
- Beason D, Dakin G, Lopez R, Alonos J, Bandak F, Eberhardt A. Bone mineral density correlated with fracture load in experimental side impacts of the pelvis. Clinical Biomechanics. 2003;36:219–227. doi: 10.1016/s0021-9290(02)00330-5. [DOI] [PubMed] [Google Scholar]
- Bedard M, Stones M, Guyatt G, Hirdes J. Traffic-related fatalities among older drivers and passengers: past and future trends. The Gerontologist. 2001;41:751–756. doi: 10.1093/geront/41.6.751. [DOI] [PubMed] [Google Scholar]
- Bedard M, Guyatt G, Stones M, Hirdes J. The independent contribution of driver, crash, and vehicle characteristics to driver fatalities. Accident Analysis & Prevention. 2002;34:717–727. doi: 10.1016/s0001-4575(01)00072-0. [DOI] [PubMed] [Google Scholar]
- Bergeron E, Lavoie A, Clas D, Moore L, Ratte S, Tetreault S, Lemarie J, Martin M. Elderly trauma patients with rib fractures are at greater risk of death and pneumonia. Journal of Trauma. 2003;54:478–485. doi: 10.1097/01.TA.0000037095.83469.4C. [DOI] [PubMed] [Google Scholar]
- Bonfield W, Behiri J, Charalambides C. Orientation and age-related dependence of the fracture of toughness of cortical bone. In: Perren S, Schneider E, editors. Biomechanics: Current Interdisciplinary Research. Martinus Nijhoff; Dordrecht, Netherlands: 1985. pp. 185–189. [Google Scholar]
- Bulger E, Arneson M, Mock C, Jurkovich G. Rib fractures in the elderly. Journal of Trauma. 2000;48:1040–1045. doi: 10.1097/00005373-200006000-00007. [DOI] [PubMed] [Google Scholar]
- Burstein A, Reilly D, Martens M. Aging of bone tissue: mechanical properties. Journal of Bone and Joint Surgery—American. 1976;58A:82–86. [PubMed] [Google Scholar]
- Bazarian J, Fisher S, Flesher W, Lillis R, Knox K, Pearson T. Lateral automobile impacts and the risk for traumatic brain injury. Annals of Emergency Medicine. 2004;44:142–152. doi: 10.1016/j.annemergmed.2004.03.029. [DOI] [PubMed] [Google Scholar]
- Cameron P, Dziukas L, Hadj A, Clark P, Hooper S. Rib fractures in major trauma. Australian and New Zealand Journal of Surgery. 1996;66:530–534. doi: 10.1111/j.1445-2197.1996.tb00803.x. [DOI] [PubMed] [Google Scholar]
- Cavanaugh J, Walilko T, Malhotra A, Zhu Y, King A. Biomechanical response and injury tolerance of the pelvis in twelve sled side impacts; Stapp Car Crash Conference; Orlando, FL. 1990. pp. 1–12. [Google Scholar]
- Cavanaugh J, Zhu Y, King AI. Mechanical properties of various padding meterials used in cadaveric side impact sled tests; SAE International Congress and Exposition; Detroit, MI. 1992. [Google Scholar]
- Cavanaugh J, Huang Y, Zhu Y, King A. Regional tolerance of the shoulder, thorax, abdomen and pelvis to padding in side impact; Stapp Car Crash Conference; San Antonio, TX. 1993. pp. 973–980. [Google Scholar]
- Cavanaugh J, Walilko T, Chung J, King A. Abdominal injury and response in side impact; Stapp Car Crash Conference; Albuquerque, NM. 1996. pp. 1–16. [Google Scholar]
- Cesari D, Ramet M. Pelvic tolerance and protection criteria in side impact; Stapp Car Crash Conference; Ann Arbor, MI. 1982. pp. 145–154. [Google Scholar]
- Cesari D, Ramet M, Bloch J. Influence of arm position on thoracic injuries in side impact; Stapp Car Crash Conference; San Francisco, CA. 1981. [Google Scholar]
- Currey J. Changes in the impact energy absorption of bone with age. Journal of Biomechanics. 1979;12:459–469. doi: 10.1016/0021-9290(79)90031-9. [DOI] [PubMed] [Google Scholar]
- Currey J, Butler G. The mechanical properties of bone tissue in children. Journal of Bone and Joint Surgery—American. 1975;57A:810–814. [PubMed] [Google Scholar]
- Dulisse B. Older drivers and risk to other road users. Accident Analysis & Prevention. 1997;29:573–582. doi: 10.1016/s0001-4575(97)00010-9. [DOI] [PubMed] [Google Scholar]
- Eppinger R, Marcus J, Morgan R. Development of dummy and injury index for NHTSA's thoracic side impact protection research program; Government/Industry Meeting and Exposition; Washington, DC. 1984. [Google Scholar]
- Ewers B, Weaver B, Haut R. Impact orientation can significantly affect the outcome of a blunt impact to the rabbit patellofemoral joint. Journal of Biomechanics. 2002;35:1591–1598. doi: 10.1016/s0021-9290(02)00230-0. [DOI] [PubMed] [Google Scholar]
- Fayon A, Tarriere C, Walfisch G, Got C, Patel A. Contributions to defining the human tolerance to perpendicular side impact. IRCOBI; Berlin, Germany: 1977. pp. 297–309. [Google Scholar]
- Federal Register . Anthropomorphic test devices; ES-2re side impact crash test dummy. Vol. 69. US Government Printing Office; Washington, DC: Sep 15, 2004. pp. 55550–55571. Docket No. NHTSA-2004-18864. 49 CFR Part 572. [Google Scholar]
- Fildes B, Vulcan P, Lane J. Side impact crashes in Australia; 14th International Tech Conference on Experimental Safety Vehicles.1994. [Google Scholar]
- Foret-Bruno J, Hartemann F, Tarriere C, Got C, Patel A. Conditions required to avoid being killed in cars in side-impact. SAE World Congress; Detroit, MI. 1983. [Google Scholar]
- Goldstein S, Frankenburg E, Kuhn J. Biomechanics of bone. In: Nahum A, Melvin J, editors. Accidental Injury. Springer; New York: 1993. pp. 198–223. [Google Scholar]
- Granik G, Stein I. Human ribs: Static testing as a promising medical application. Journal of Biomechanical Engineering. 1973;6:9–15. doi: 10.1016/0021-9290(73)90045-6. [DOI] [PubMed] [Google Scholar]
- Green P. Aging and Driving Symposium. AAAM; Southfield, MI: 2001. Variations in task performance between younger and older drivers. [Google Scholar]
- Green P, German A, Nowak E, Dalmotas D, Stewart D. Fatal injuries to restrained passenger car occupants in Canada: crash modes and kinematics of injury. Accident Analysis & Prevention. 1994;26:207–214. doi: 10.1016/0001-4575(94)90090-6. [DOI] [PubMed] [Google Scholar]
- Haddak M, Ramet M, Vallet G, Cesari D. Side impact into a fixed object: what is at stake?; 13th International Tech Conference on Experimental Safety Vehicles; Paris, France. 1991. [Google Scholar]
- Hansson T, Roos B. The relation between bone mineral content, experimental compression fractures, and disc degeneration in lumbar vertebrae. Spine. 1981;6:147–153. doi: 10.1097/00007632-198103000-00007. [DOI] [PubMed] [Google Scholar]
- Hansson T, Roos T, Nachemson A. The bone mineral content and ultimate compressive strength of lumbar vertebrae. Spine. 1980;5:46–55. doi: 10.1097/00007632-198001000-00009. [DOI] [PubMed] [Google Scholar]
- Hassan A, Morris A, Mackey M, Haland Y. Severity in side impacts: implications for side impact airbag. IRCOBI; Brunnen, Switzerland: 1995. [Google Scholar]
- Hayes W. Biomechanics of cortical and trabecular bone. Raven Press, Ltd.; New York, NY: 1991. [Google Scholar]
- Irwin A, Walilko T, Cavanaugh J, Zhu Y, King A. Displacement responses of the shoulder and thorax in lateral sled impacts; Stapp Car Crash Conference; San Antonio, TX. 1993. pp. 166–173. [Google Scholar]
- Keaveny TM, Hayes WC. A 20 year perspective on the mechanical properties of the trabecular bone. Journal of Biomechanical Engineering. 1993;115:534–542. doi: 10.1115/1.2895536. [DOI] [PubMed] [Google Scholar]
- Keaveny TM, Yeh OC. Architecture and trabecular bone—toward an improved understanding of the biomechanical effects of age, sex, and osteoporosis. Journal of Musculoskeletal & Neuronal Interactions. 2002;2:205–208. [PubMed] [Google Scholar]
- Kent R, Viano D, Crandall J. The field performance of frontal airbags: a review of the literature. Traffic Injury Prevention. 2005;6:1–23. doi: 10.1080/15389580590903131. [DOI] [PubMed] [Google Scholar]
- Kimpara H, Iwamoto M, Miki K, Lee J, Begeman P, Yang K, King A. Biomechanical properties of the male and female chest subjected to frontal and lateral impacts. IRCOBI; Lisbon, Portugal: 2003. pp. 235–247. [Google Scholar]
- Klaus G, Kalleris D. Side impact—a comparison between HSRI, APROD and HYBRID II dummies and cadavers. Ninth International Tech Conference on Experimental Safety Vehicles; Kyoto, Japan. 1982. [Google Scholar]
- Klaus G, Kalleris D. Side impact—a comparison between HSRI, APROD and HYBRID II dummies and cadavers; Stapp Car Crash Conference; San Diego, CA. 1983. pp. 365–381. [Google Scholar]
- Klaus G, Sinnhuber R, Hoffman G, Kalleris D, Mattern R. Side impact—a comparison between dummies and cadavers, correlations between cadaver loads and injury severity; Stapp Car Crash Conference; Chicago, IL. 1984. pp. 237–259. [Google Scholar]
- Kleinberger M, Yoganandan N, Kumaresan S. Biomechanical considerations for child occupant protection. AAAM; Charlottesville, VA: 1998. pp. 115–136. [Google Scholar]
- Koh S, Cavanaugh J, Zhu J. Injury response of the shoulder in lateral sled tests; Stapp Car Crash Conference; San Antonio, TX. 2001. pp. 101–141. [DOI] [PubMed] [Google Scholar]
- Kuppa S, Eppinger F, Maltese M, Naik R, Yoganandan N, Pintar F, Saul R, McFadden J. Assessment of thoracic injury criteria for side impact. IRCOBI; Montpellier, France: 2000. pp. 131–146. [Google Scholar]
- Kuppa S, Eppinger F, McKoy F, Nguyen T, Pintar F, Yoganandan N. Development of side impact thoracic injury and their application to the modified ES-2 dummy with rib extension (ES-2re) Stapp Car Crash Journal. 2003;47:189–210. doi: 10.4271/2003-22-0010. [DOI] [PubMed] [Google Scholar]
- Lestina D, Gloyns P, Rattenbury S. Fatally injured occupants in side impact crashes. IRCOBI; Berlin, Germany: 1991. [Google Scholar]
- Lindahl O, Lindgren A. Cortical bone in man II: Variation in tensile strength with age and sex. Acta Orthopaedica Scandinavica. 1967;38:141–147. doi: 10.3109/17453676708989628. [DOI] [PubMed] [Google Scholar]
- Lindsey D, Kim M, Hannibal M, Alamin T. The monotonic and fatigue properties of osteoporotic thoracic vertebral bodies. Spine. 2005;30:645–649. doi: 10.1097/01.brs.0000155411.69149.49. [DOI] [PubMed] [Google Scholar]
- Lund AK. Recommended procedures for evaluating occupant injury risk from deploying side airbags. International Standard Organization. 2000 [Google Scholar]
- Lupton F. Aging and Driving Symposium. AAAM; Southfield, MI: 2001. The 3rd age suit. [Google Scholar]
- Lyman S, Ferguson S, Braver E, Williams A. Older driver involvements in police reported crashes and fatal crashes: trends and projections. Injury Prevention. 2002;8:116–120. doi: 10.1136/ip.8.2.116. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Maiman D, Yoganandan N, Pintar F. Preinjury cervical alignment affects spine trauma. Journal of Neurosurgery. Spine. 2002;97:57–62. doi: 10.3171/spi.2002.97.1.0057. [DOI] [PubMed] [Google Scholar]
- Maltese M, Eppinger R, Rhule H, Donnelly B, Pintar F, Yoganandan N. Response corridors of human surrogates in lateral impacts. Stapp Car Crash Journal. 2002;46:321–351. doi: 10.4271/2002-22-0017. [DOI] [PubMed] [Google Scholar]
- Marcus J, Morgan R, Eppinger R, Kalleris D, Mattern R, Schmidt G. Human response to injury from lateral impact; Stapp Car Crash Conference; Bron, France. 1983. [Google Scholar]
- McCalden R, McGeough J, Barker M, Court-Brown C. Age-related changes in the tensile properties of cortical bone. Journal of Bone and Joint Surgery—American. 1993;75A:1193–1205. doi: 10.2106/00004623-199308000-00009. [DOI] [PubMed] [Google Scholar]
- McCoy G, Johnston R, Duthie R. Injury to the elderly in road traffic accidents. Journal of Trauma. 1989;29:494–497. doi: 10.1097/00005373-198904000-00013. [DOI] [PubMed] [Google Scholar]
- McGwin G, Metzger J, Porterfield J, Moran S, Rue L. Association between side air bags and risk of injury in motor vehicle collisions with near-side impact. Journal of Trauma. 2003;55:430–436. doi: 10.1097/01.TA.0000083478.98648.C8. [DOI] [PubMed] [Google Scholar]
- Melvin J. Biomechanics of lateral thoracic injury. In: Backaitis S, editor. Biomechanics of Impact Injury and Injury Tolerances of the Thorax–Shoulder Complex. SAE, Inc.; Warrendale, PA: 1994. pp. 837–842. [Google Scholar]
- Melvin JW, Stalnaker RL, Roberts VL. Impact injury mechanisms in abdominal organs. Stapp Car Crash Conference; Oklahoma City, OK. 1973. pp. 115–126. [Google Scholar]
- Melvin J, Robbins D, Stalnaker R. Side impact response and injury; Sixth International Tech Conference on Experimental Safety Vehicles.1976. pp. 681–689. [Google Scholar]
- Moore R, Sedgley I, Sabey B. Ages of car drivers involved in accidents with special reference to junctions. Transport and Road Research Laboratory; Berkshire, UK: 1982. [Google Scholar]
- Morgan R, Marcus J, Eppinger R. Side impact: the biofidelity of NHTSA's proposed ATD and efficacy of TTI; Stapp Car Crash Conference; San Diego, CA. 1986. pp. 27–40. [Google Scholar]
- Mosekilde L, Mosekilde L. Normal vertebral body size and compressive strength: relations to age and to vertebral and iliac trabecular bone compressive strength. Bone. 1986;7:207–212. doi: 10.1016/8756-3282(86)90019-0. [DOI] [PubMed] [Google Scholar]
- Mourant R. Driving performance of the elderly. Accident Analysis & Prevention. 1979;11:247–253. [Google Scholar]
- NCSA . Traffic Safety Facts 2001. National Center for Statistics & Analysis, National Highway Traffic Safety Administration; Washington, DC: 2001. [Google Scholar]
- NHTSA Buying a Safer Car. 2002a http://www.nhtsa.dot.gov/ncap/
- NHTSA . FMVSS—Federal Motor Vehicle Safety Standards. National Highway Traffic Safety Administration; Washington, DC: 2002b. Code of Federal Regulations, Title 49, Part 571. [Google Scholar]
- NHTSA Side Air Bags. 2002c http://www.nhtsa.dot.gov/ncap/
- NHTSA . Department of Transportation; 2005. www.nhtsa.dot.gov. [Google Scholar]
- Nusholtz GS, Alem N, Melvin JW. Impact response and injury to the pelvis; Stapp Car Crash Conference; Ann Arobor, MI. 1982. pp. 103–142. [Google Scholar]
- Pintar FA, Yoganandan N, Voo LM, Cusick JF, Maiman DJ, Sances A., Jr. Dynamic characteristics of the human cervical spine. SAE Transactions. 1995;104:3087–3094. [Google Scholar]
- Pintar FA, Yoganandan N, Sances A, Jr., Eppinger RH. Instrumentation of human surrogates for side impact; Stapp Car Crash Conference; Albuquerque, NM. 1996. pp. 29–42. [Google Scholar]
- Pintar FA, Yoganandan N, Hines MH, Maltese MR, McFadden J, Saul R, Eppinger R, Khaewpong N, Kleinberger M. Chestband analysis of human tolerance to side impact; Stapp Car Crash Conference; Lake Buena Vista, FL. 1997. pp. 63–74. [Google Scholar]
- Pintar F, Voo L, Yoganandan N. The mechanisms of hyperflexion cervical spine injury. IRCOBI; Goteborg, Sweden: 1998a. pp. 349–363. [Google Scholar]
- Pintar FA, Yoganandan N, Voo L. Effect of age and loading rate on human cervical spine injury threshold. Spine. 1998b;23:1957–1962. doi: 10.1097/00007632-199809150-00007. [DOI] [PubMed] [Google Scholar]
- Pintar F, Yoganandan N, Maltese M, Samaha R, Eppinger R. Three-year-old child out-of-position side airbag studies; Stapp Car Crash Conference; San Diego, CA. 1999. pp. 25–38. [Google Scholar]
- Preusser D, Williams A, Ferguson S, Ulmer R, Weinstein H. Fatal crash risk for older drivers at intersections. Accident Analysis & Prevention. 1998;30:151–159. doi: 10.1016/s0001-4575(97)00090-0. [DOI] [PubMed] [Google Scholar]
- Pugh JW, Rose RM, Radin EL. A structural model for the mechanical behavior of trabecular bone. Journal of Biomechanics. 1972;6:657–670. doi: 10.1016/0021-9290(73)90022-5. [DOI] [PubMed] [Google Scholar]
- Read K. Aging and Driving Symposium. AAAM; Southfield, MI: 2001. On the road again..psychosocial factors and injury outcomes of motor vehicle occupants over 60. [Google Scholar]
- Reiff D, McGwin G, Rue L. Splenic injury in side impact motor vehicle collisions: effect of occupant restraints. Journal of Trauma. 2001;51:340–345. doi: 10.1097/00005373-200108000-00020. [DOI] [PubMed] [Google Scholar]
- Rho J, Hobatho M, Ashman R. Relations of mechanical properties to density and CT numbers in human bone. Medical Engineering & Physics. 1995;17:347–355. doi: 10.1016/1350-4533(95)97314-f. [DOI] [PubMed] [Google Scholar]
- Riggs BL. Population-based study of age and sex differences in bone volumetric density, size, geometry, and structure of different skeletal sites. Journal of Bone and Mineral Research. 2004;19:1945–1953. doi: 10.1359/JBMR.040916. [DOI] [PubMed] [Google Scholar]
- Robbins D, Lehman R, Augustyn K. Prediction of thoracic injuries as a function of occupant kinematics. In: Bachaitis S, editor. Biomechanics of Impact Injury and Injury Tolerances of the Thorax–Shoulder Complex. SAE, Inc.; Warrendale, PA: 1994. pp. 1109–1118. [Google Scholar]
- Rouhana S, Foster M. Lateral impact: analysis of the statistics in the NCSS; Stapp Car Crash Conference; Washington, DC. 1985. pp. 79–98. [Google Scholar]
- Schultz AB, Benson DR, Hirsch C. Force-deformation properties of human ribs. Journal of Biomechanics. 1974;7:303–309. doi: 10.1016/0021-9290(74)90023-2. [DOI] [PubMed] [Google Scholar]
- Scialfa C, Kline D, Lyman B, Kosnik W. Age differences in judgments of vehicle velocity and distance; 31st Human Factors Society Conference; New York, NY. 1987. [Google Scholar]
- Shorr R, Rodriguez Z, Indeck M, Crittdnden M, Hartunian S, Cowley R. Rib fractures in major trauma. Journal of Trauma. 1989;29:234–237. doi: 10.1097/00005373-198902000-00016. [DOI] [PubMed] [Google Scholar]
- Singer K, Edmonston S, Day R, Beidahl P, Price R. Prediction of thoracic and lumbar vertebral body compressive strength: correlations with bone mineral density and vertebral region. Bone. 1995;17:167–174. doi: 10.1016/s8756-3282(95)00165-4. [DOI] [PubMed] [Google Scholar]
- Stalnaker R, Tarriere C, Fayon A, Walfisch G, Balthazard M, Masset J. Modification of part 572 dummy for lateral impact according to biomechanical data; Stapp Car Crash Conference; San Diego, CA. 1979. pp. 843–872. [Google Scholar]
- Stemper B, Yoganandan N, Pintar F, Rao R. Reflex muscle contraction in the unaware occupant in whiplash injury. Spine. 2005;30:2794–2798. doi: 10.1097/01.brs.0000192178.46869.42. [DOI] [PubMed] [Google Scholar]
- Stutts J. Aging and Driving Symposium. AAAM; Southfield, MI: 2001. The epidemiology of the aging driver. [Google Scholar]
- Tarriere C, Walfisch G, Fayon A, Got C, Guillon F. Synthesis of human impact tolerance obtained from lateral impact simulations; Seventh International Tech Conference on Experimental Safety Vehicles; Washington, DC. 1979. pp. 359–373. [Google Scholar]
- Taylor M, Tracy K, Meyer W, Pasquale M, Napolitano L. Trauma in the elderly: Intensive care unit resource use and outcome. Journal of Trauma. 2002;53:407–414. doi: 10.1097/00005373-200209000-00001. [DOI] [PubMed] [Google Scholar]
- The Abbreviated Injury Scale (AIS) American Association for Automotive Medicine; Arlington Heights, IL: 1990. [Google Scholar]
- Thomas P, Bradford M. Side impact regulations-how do they relate to real world accidents?; 12th International Tech Conference on Experimental Safety Vehicles; Gothenborg, Sweden. 1989. pp. 919–929. [Google Scholar]
- Thomas P, Frampton R. Injury patterns in side collisions—a new look with reference to current test methods and injury criteria; Stapp Car Crash Conference; San Diego, CA. 1999. pp. 1–12. [Google Scholar]
- Vala M. Aging and Driving Symposium. AAAM; Southfield, MI: 2001. Designing vehicle interior for the mature drivers. [Google Scholar]
- Viano D. Biomechanical responses and injuries in blunt lateral impact; Stapp Car Crash Conference; Washington, DC. 1989. pp. 113–142. [Google Scholar]
- Viano D, Culver C, Evans L, Frick M, Scott R. Involvement of older drivers in multi-vehicle side impact crashes. AAAM; Baltimore, MD: 1989a. pp. 337–352. [DOI] [PubMed] [Google Scholar]
- Viano D, Lau I, Asbury C, King A, Begeman P. Biomechanics of the human chest, abdomen, and pelvis in lateral impact. Accident Analysis & Prevention. 1989b;21:553–574. doi: 10.1016/0001-4575(89)90070-5. [DOI] [PubMed] [Google Scholar]
- Viano D, Lau I, Asbury C, King A, Begeman P. Biomechanics of the human chest, abdomen, and pelvis in lateral impacts. 33rd Association for Advancement of Auto Medicine; Baltimore, MD: 1989c. [DOI] [PubMed] [Google Scholar]
- Walfisch G, Fayon A, Tarriere C, Rosey J, Guillon F, Got C, Patel A, Stalnaker R. Designing of a dummy's abdomen for detecting injuries in side impact collisons. IRCOBI; 1980. pp. 149–164. [Google Scholar]
- Wall J, Chatterji S, Jeffery J. Age related changes in the density and tensile strength of human femoral cortical gone. Calcified Tissue International. 1979;27:105–108. doi: 10.1007/BF02441170. [DOI] [PubMed] [Google Scholar]
- Warner C, Strother C, James M, Struble D, Egbert T. Crash protection in near-side impact-advantages of a supplemental inflatable restraint; International Congress and Exposition; Detroit, MI. 1989. pp. 85–97. [Google Scholar]
- Wilson CR. Bone-mineral content of the femoral neck and spine versus the radius or ulna. Journal of Bone and Joint Surgery. 1977;59A:665–669. [PubMed] [Google Scholar]
- Wismans J, Happee R, Dommelen J. Computational human body models. In: Gilchrist M, editor. Impact Biomechanics: from Fundamental Insights to Applications. Springer; The Netherlands: 2005. pp. 417–429. [Google Scholar]
- Yamada H. Strength of Biological Materials. Williams & Wilkins; Baltimore, MD: 1970. [Google Scholar]
- Yoganandan N, Pintar FA. Biomechanics of human thoracic ribs. Journal of Biomechanical Engineering. 1998;120:100–104. doi: 10.1115/1.2834288. [DOI] [PubMed] [Google Scholar]
- Yoganandan N, Pintar FA. Deflection, acceleration, and force corridors for small females in side impacts. Traffic Injury Prevention. 2005;6:1–8. doi: 10.1080/15389580500256888. [DOI] [PubMed] [Google Scholar]
- Yoganandan N, Skrade D, Pintar F, Reinartz J, Sances A. Thoracic deformation contours in a frontal impact; Stapp Car Crash Conference; San Diego, CA. 1991. pp. 47–63. [Google Scholar]
- Yoganandan N, Pintar FA, Reinartz J, Sances A. Human facial tolerance to steering wheel impact: a biomechanical study. Journal of Safety Research. 1993;24:77–85. [Google Scholar]
- Yoganandan N, Pintar FA, Skrade D, Chmiel W, Reinartz JM, Sances A. Thoracic biomechanics with air bag restraint. SAE Transactions. 1994a;102:2597–2607. [Google Scholar]
- Yoganandan N, Pintar FA, Skrade D, Sances A. Evaluation of thoracic trauma in frontal impact. International Conference on Enhanced Safety of Vehicles; Munich, Germany. 1994b. pp. 110–117. [Google Scholar]
- Yoganandan N, Morgan RM, Eppinger RH, Pintar FA, Skrade DA, Sances A. Thoracic deformation and velocity analysis in frontal impact. Journal of Biomechanical Engineering. 1995;117:48–52. doi: 10.1115/1.2792269. [DOI] [PubMed] [Google Scholar]
- Yoganandan N, Haffner M, Pintar FA. Facial injury: a review of biomechanical studies and test procedures for facial injury assessment. Journal of Biomechanics. 1996a;29:985–986. doi: 10.1016/0021-9290(95)00159-x. [DOI] [PubMed] [Google Scholar]
- Yoganandan N, Morgan RM, Eppinger RH, Pintar FA, Sances A, Williams A. Mechanism of thoracic injury in a frontal impact. Journal of Biomechanical Engineering. 1996b;118:595–597. doi: 10.1115/1.2796049. [DOI] [PubMed] [Google Scholar]
- Yoganandan N, Pintar FA, Boynton M, Begeman P, Prasad P, Kuppa S, Morgan RM, Eppinger RH. Dynamic axial tolerance of the human foot–ankle complex. SAE Transactions. 1996c;105:1887–1898. [Google Scholar]
- Yoganandan N, Pintar FA, Kumaresan S, Sances A, Haffner M. Response of human lower thorax to impact. AAAM; Vancouver, BC, Canada: 1996d. pp. 33–43. [Google Scholar]
- Yoganandan N, Boynton M, Pintar FA. Axial impact biomechanics of the human foot-ankle complex. Journal of Biomechanical Engineering. 1997a;119:433–437. doi: 10.1115/1.2798290. [DOI] [PubMed] [Google Scholar]
- Yoganandan N, Pintar FA, Kumaresan S, Haffner M, Kuppa S. Impact biomechanics of the human thorax–abdomen complex. International Journal of Crashworthiness. 1997b;2:219–228. [Google Scholar]
- Yoganandan N, Pintar F, Gennarelli T, Eppinger R, Voo L. Geometrical Effects on the Mechanism of Cervical Spine Injury due to Head Impact. IRCOBI; Barcelona, Spain: 1999a. pp. 261–270. [Google Scholar]
- Yoganandan N, Pintar F, Seipel R. Experimental production of extra- and intra-articular fractures of the oscalcis. Journal of Biomechanics. 1999b;33:745–749. doi: 10.1016/s0021-9290(00)00017-8. [DOI] [PubMed] [Google Scholar]
- Yoganandan N, Pintar F, Maltese M. Biomechanics of abdominal injuries. CRC Review of Biomedical Engineering. 2001a:489–569. doi: 10.1615/critrevbiomedeng.v29.i2.10. [DOI] [PubMed] [Google Scholar]
- Yoganandan N, Pintar FA, Gennarelli T, Maltese M, Eppinger R. Mechanisms and factors involved in hip injuries during frontal crashes. Stapp Car Crash Journal. 2001b;45:437–448. doi: 10.4271/2001-22-0020. [DOI] [PubMed] [Google Scholar]
- Yoganandan N, Pintar F, Maltese M, Eppinger R, Rhule H, Donnelly B. Biofidelity Evaluation of Recent Side Impact Dummies. IRCOBI; Munich, Germany: 2002. pp. 57–69. [Google Scholar]
- Yoganandan N, Pintar F, Gennarelli T. Evaluation of side impact injuries in vehicles equipped with side airbags. IRCOBI; Prague, Czech Republic: 2005a. pp. 97–108. [Google Scholar]
- Yoganandan N, Pintar F, Gennarelli T. Field data on head injuries in side airbag vehicles in lateral impact. AAAM. 2005b;49:171–184. [PMC free article] [PubMed] [Google Scholar]
- Yoganandan N, Pintar FA, Stemper B, Baisden J, Aktay R, Shender B, Paskoff G. Bone mineral density of human female cervical and lumbar spines from quantitative computed tomography. Spine. 2006;30 doi: 10.1097/01.brs.0000192684.12046.93. [DOI] [PubMed] [Google Scholar]
- Zaouk A, Eigen A, Digges K. Occupant injury patterns in side crashes; SAE World Congress; Detroit, MI. 2001. pp. 77–81. [Google Scholar]
- Zhang J, Fraser S, Lindsay J, Clarke K, Mao Y. Age-specific patterns of factors related to fatal motor vehicle traffic crashes. Public Health. 1998;112:289–295. doi: 10.1038/sj.ph.1900485. [DOI] [PubMed] [Google Scholar]
- Zhang J, Lindsay J, Clarke K, Robbins G, Mao Y. Factors affecting the severity of motor vehicle traffic crashes involving elderly drivers in Ontario. Accident Analysis & Prevention. 2000;32:117–125. doi: 10.1016/s0001-4575(99)00039-1. [DOI] [PubMed] [Google Scholar]
- Zhou Q, Rouhana SW, Melvin JW. Age effects on thoracic injury tolerance; Stapp Car Crash Conference; Albuquerque, NM. 1996. pp. 137–148. [Google Scholar]
- Zhu Y, Cavanaugh J, King A. Pelvic biomechanical response and padding benefits in side impact based on a cadaveric test series; Stapp Car Crash Conference; San Antonio, TX. 1993. pp. 223–233. [Google Scholar]
- Zioupos P, Currey J. Change in stiffness, strength, and tightness of human cortical bone with age. Bone. 1998;22:57–66. doi: 10.1016/s8756-3282(97)00228-7. [DOI] [PubMed] [Google Scholar]