

Abstract
It is well documented that children with a Fontan circulation have a reduced exercise capacity. One of the modalities to improve exercise capacity might be exercise training. We performed a systematic literature review on the effects of exercise training in patients with a Fontan circulation. Six published studies were included that reported on the effects of exercise training in 40 patients. All studies had a small sample size and/or did not include a control group.
Based on the six published studies we can conclude that children who have undergone a Fontan operation and who are in a stable haemodynamic condition can safely participate in an exercise training programme and that exercise training results in an improved exercise capacity. However, more research is needed to establish the optimal exercise mode, dose-response relation, and the effects of exercise training on cardiac function, peripheral muscle function, physical activity, and health-related quality of life. (Neth Heart J 2007;15:142-7.)
Keywords: Exercise training in Fontan patients; Fontan circulation; child, exercise (capacity) (training); oxygen (maximal uptake); physical fitness
Congenital heart defects have a reported incidence of 4 to 8 per 1000 live births and encompass a broad spectrum of disorders.1 Two percent of these children have a single functioning ventricle. Single ventricle hearts comprise a heterogeneous group of defects which are not suited for a two ventricle repair. In 1971 Fontan et al.2 described a surgical procedure to palliate such hearts by separating the systemic and pulmonary venous return. This was introduced to obtain normal oxygenation and to avoid volume overloading. The ‘Fontan circulation’ procedure connects the systemic venous return to the pulmonary arteries without the interposition of an adequate ventricle and all shunts at the venous, atrial, ventricular and arterial level are interrupted.3
Patients with a Fontan circulation possess a unique physiological response to exercise. Although there is wide range in peak oxygen uptake (VO2peak) during exercise between patients,4 all patients have a reduced VO2peak,4 compared with healthy controls.
According to Fick’s equation, VO2peak is the product of cardiac output (stroke volume x heart rate) and peripheral O2 extraction.5 As can be appreciated from figure 1, the reduced VO2peak can be caused by a combination of several factors. Previous studies have indicated that chronotropic incompetence may partly explain the diminished VO2peak in Fontan patients.4 Moreover cardiac stroke volume might also be a limiting factor for these patients, as has been found previously.6,7 The reduced stroke volume might be explained by a limited diastolic return to the systemic ventricle,8 or by a chronic volume overload,9 or impaired function (diminished contractile response and impaired diastolic filling).10
Figure 1.
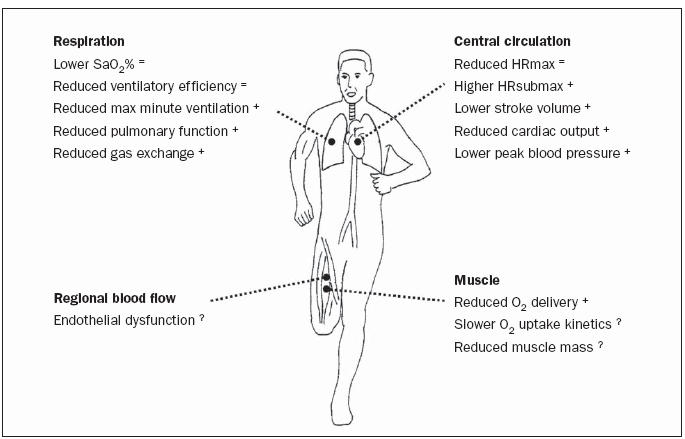
Limitations of VO2peak in patients with a Fontan circulation and the effects of exercise training. SaO2%=arterial oxygen saturation, Hrmax=maximal heart rate, Hrsubmax=heart rate during submaximal exercise, + indicates improvement after exercise training, = indicates no change after exercise training, ?=no data available.
At rest and up to submaximal levels of exercise, arterial blood pressure is relatively well-maintained in Fontan patients, partly due to increased systemic arterial resistance.7 Peak blood pressure, however, is usually lower than in healthy subjects because of an impaired increase in cardiac output at peak exercise.11
Peak minute ventilation (VE) during exercise is decreased in Fontan patients and is also related to VO2peak and might be explained by a low pulmonaryblood flow.12-14 In patients with a Fontan circulation the non-pulsatile pulmonary blood flow might lead to a deterioration in gas exchange in the lungs.13 Moreover, an increased pulmonary vascular resistance, which is observed in congenital heart disease, might contribute to a reduced pulmonary blood flow, and hence a reduced cardiac output and impaired gas exchange.15
In a recent study we found that ventilatory efficiency (VE/VCO2; an index of dead space ventilation) was significantly negatively correlated with VO2peak.12 Ventilation/perfusion mismatching has been identified as a major factor contributing to an increase in physiological dead space in Fontan patients.16 Moreover, patients with a Fontan circulation have small lungs,13 requiring a higher breathing frequency to obtain a certain minute ventilation. A reduced pulmonary function has been shown to be related with VO2peak in patients with a Fontan circulation.14
A reduction in SaO2% is frequently observed during exercise, showing the reduced arterial oxygen saturation and hence limitations in oxygen transport.4 Since patients with a Fontan circulation have a larger arteriovenous O2 difference during exercise (to compensate the reduced cardiac output),7 a reduced SaO2% contributes further to a limitation in VO2peak.
Moreover, recent studies have suggested skeletal muscle impairment in patients with a congenital heart disease.17 Inai et al. found a reduced muscle blood flow during exercise in children with a Fontan circulation as measured with near-infrared spectroscopy.18 Mertens et al. reported slower oxygen uptake kinetics in patients with a Fontan circulation, reflecting the impaired oxygen delivery at the working muscles.19 Moreover, compared with healthy peers, a reduced body mass is frequently observed in patients with congenital heart disease.20 A lower muscle mass also contributes to a lower oxygen utilisation during exercise and a lower VO2peak.21
Patients with a Fontan circulation who are in good condition are advised to participate in regular lowintensity aerobic exercise to increase their physical fitness.22 However, in another study the combination of strength and aerobic exercises was advocated.23 These differences in exercise programming highlight the need for a better understanding of the trainability in Fontan patients and the need for practical exercise guidelines.
The significant reduction in exercise capacity in Fontan patients compared with healthy peers is worrisome, as health outcome and survival may be directly related to exercise capacity.24 As exercise capacity is an important predictor of health outcome and survival in adult patients with cardiovascular disease,24 children with pulmonary diseases,25 as well as in healthy subjects, 24,26 the purpose of this systematic review is to summarise the effects of exercise training in patients with a Fontan circulation and to provide practical guidelines concerning exercise counselling for the practitioner.
Search strategy
Literature was selected from 1966 until November 2006 using Medline, Embase and Sportdiscus databases. Search terms were “physical fitness”, “exercise training”, “cardiac rehabilitation”, “exercise”, “exercise capacity”, “exercise tolerance”, “Fontan” and “univentricular”. References of the selected publications were tracked to find additional publications on this subject. Inclusion criteria consisted of studies with at least a three-week training period and a minimum of six training sessions.
Experimental findings
Six studies were identified in the literature, one of which was a case report. Two of the studies included children with congenital heart diseases other than Fontan circulation.27-29 The characteristics of the six studies are displayed in table 1.
Table 1.
Characteristics of the exercise training studies.
| Author | Age | Patients (n) | Type of exercise | Training duration | Frequency | Intensity | Time |
|---|---|---|---|---|---|---|---|
| McCall & Humphrey30 | 18 | 1 | Aerobic (bicycle, treadmill) Resistance | 22 weeks 22 weeks | 2-3/week 2-3/week | 50-70% VO2peak 12-15 repetitions, light exercises | 20-30 min |
| Minamisawa et al.31 | 19±4 | 11 | 8-12 weeks | 2-3/week | 60-80% HRpeak | 20-30 min | |
| Opocher et al.34 | 8.7±0.6 | 10 | Aerobic (cycling) | 8 months | 2/week | 50-70% VO2peak | 30-45 min |
| Rhodes et al.28 | 11.9±2.1 | 11 Fontan, 5 other CHD | Aerobic | 12 weeks | 2/week* | 55-58% VO2peak | 60 min |
| Resistance | 2/week | Light resistance | |||||
| Moalla et al.27,29 | 13.0±1.4 | 2 Fontan, 8 other CHD | Aerobic (cycling) | 12 | 3/week | 62% VO2peak | 45 min |
| Brassard et al.23 | 16±5 | 5 | Aerobic Resistance | 8 weeks | 3/week | 50-80% VO2peak 12-15 repetitions | 20-30 min |
* Patients were encouraged to exercise an additional twice a week at home. CHD=congenital heart disease, VO2peak= peak oxygen uptake, HR peak=peak heart rate.
McCall and Humphrey were the first to document training effects of a formal exercise programme in a single patient with a Fontan circulation.30 The patient attended cardiopulmonary training sessions two to three times a week for 22 weeks at a moderate intensity. Training sessions consisted of a combination of cardiovascular exercise, both treadmill and stationary cycle, and light resistance training with weights (table 1). The patient was unable to complete formal exercise testing prior to the training programme; however, formal exercise testing was successfully conducted on the patient following the exercise training programme. As expected, exercise capacity was still much lower than normal values after the training programme.
Minamisawa et al.31 studied exercise programmes in 11 patients with Fontan circulation, each subject entered an exercise programme that was individually prescribed. The exercise programme consisted of three supervised training sessions in the first three weeks of the programme; thereafter the training was continued using home-based exercise training sessions. The exercise training was performed two to three days a week for two to three months. Patients underwent fast walking or jogging for 20 to 30 minutes at a moderate intensity (table 1). After the training programme, there was a significant improvement in peak oxygen uptake (VO2peak; table 2); however, the improvement was lower when compared with the results of the other studies. Lower VO2peak values obtained in the Minamisawa study might be explained by the use of a bicycle ergometer test to evaluate a running-based exercise training programme. Training effects are exercise mode specific with only a small transfer effect to other exercise modalities.32,33
Table 2.
Outcome instruments used and reported results of exercise training.
| Study | Outcome measure | Results |
|---|---|---|
| McCall & Humphrey30 | Exercise capacity (treadmill exercise test) | Improvement in exercise capacity |
| Minamisawa et al.31 | Exercise capacity (bicycle ergometer) | 7% improvement in VO2peak |
| Opocher et al.34 | Exercise capacity (treadmill exercise test) | 19% improvement in VO2peak |
| Rhodes et al.28 | Exercise capacity (bicycle ergometer) | 22% improvement in VO2peak |
| Rhodes et al.28 | Pulmonary function | 7% improvement in FEV1 |
| Moalla et al.27,29 | Exercise capacity (bicycle ergometer) | 8.1% improvement in VO2peak |
| Moalla et al.27 | Six-minute walk | 13% improvement in walking distance |
| Moalla et al.29 | Oxygenation respiratory muscles (NIRS) | 28% improvement in respiratory muscle oxygenation |
| Moalla et al.29 | Pulmonary function | Nonsignificant improvements in FEV1 (7.5%), FVC (6.2%), |
| TLC (4.2) and MVV (5.7%) | ||
| Brassard et al.23 | Exercise capacity (bicycle ergometer test) | No significant improvement in VO2peak |
| Brassard et al.23 | Muscle strength | No significant improvement in MVC |
| Brassard et al.23 | Blood pressure | Significant improvement in ergoreflex |
NIRS=near infrared spectroscopy, FEV1=forced expiratory volume in 1 second, FVC=forced vital capacity, TLC=total lung capacity, MVV=maximum voluntary ventilation, MVC=maximum voluntary contraction.
Opocher et al.34 studied the effects of an eight-month training programme in ten children with a Fontan circulation. Supervised training sessions were held twice a week for the first three weeks (10 sessions) and then once a month for the next four months of the training programme (table 1). Home training sessions were held at each child’s home twice a week for 30 to 45 minutes. The exercise level during training was designed to range from low to moderate intensity (table 1).
A clinically significant increase in VO2peak was noted (table 2), as well as a decrease in the heart rate curve and an increased oxygen pulse (the ratio of oxygen uptake and heart rate) during submaximal exercise.
In a study by Rhodes et al.,28 16 children with congenital heart disease (11 Fontan patients, 5 with other congenital heart disease) performed an exercise test before and after a rehabilitation programme. The rehabilitation programme consisted of one hour of aerobic and light weight resistance exercise twice a week for 12 weeks (table 1). Patients were encouraged to exercise at a heart rate that was equivalent to their ventilatory anaerobic threshold measured during their baseline exercise test. They reported a significant increase in VO2peak (table 2) and other physiological parameters during exercise upon completion of the exercise rehabilitation programme. The peak exercise systolic blood pressure was not affected by the programme. However, the patients’ peak exercise diastolic blood pressure was significantly higher after rehabilitation. Also a rise in peak minute ventilation (22%) was reported, which resulted in an insignificant decline in the breathing reserve. Exercise rehabilitation had no effect on peak exercise oxygen saturation. The authors suggested that the improvements were related, at least in part, to an exercise-induced increase in muscle strength, muscle mass, and pumping capacity of the skeletal muscles.28
In a recent study by Brassard et al.23 five Fontan patients were enrolled in an eight-week trial of combined aerobic and resistance training programmes. Two patients exercised in hospital and three patients exercised at home. Aerobic training consisted of exercise on a cycle ergometer, 20 to 30 minutes/session, twice a week. The training programme was individually prescribed to allow the subjects to work progressively at 50 to 80% of their V02peak throughout the eight weeks (table 1). Resistance training exercises were also performed and consisted of an eight exercise circuit training programme without rest between the exercises (table 1). Brassard et al. included resistance exercise because they found a strongly significant correlation between muscle strength and VO2peak,23 suggesting a role for peripheral muscle strength as one of the causes of exercise intolerance. However, they did not find significant changes in VO2peak, VO2peak/kg and skeletal muscle strength after exercise training (table 2).
Moalla et al.27,29 also studied a training programme in children with congenital heart disease. The training programme was 12 weeks in duration with three exercise training sessions per week, 45 minutes per session (table 1). A six-minute walk test was used in this study to measure the outcome of the programme instead of using a maximal cycle ergometer test. After the training programme the mean distance walked improved significantly (+62 meters). An increase in ventilatory anaerobic threshold, VO2peak, heart rate and minute ventilationwere also reported. No significant difference for SaO2% were found before or after training.27
Discussion
The purpose of this review is to summarise the effects of exercise training in patients with a Fontan circulation. All six published studies showed that exercise training could improve exercise capacity in patients with a Fontan circulation. However, the included patients in the studies were patients with a stable haemodynamic condition. It is preferable to screen patients for abnormalities during an exercise test (e.g. exercise-induced arrhythmias, ST depression, hypertension, hypotension, cardiac chest pain, or systemic desaturation <80%) before they start participating in exercise training.28,35
In a recent publication, Rhodes et al. showed that the effects of exercise training on VO2peak and ventilatory anaerobic threshold could be sustained in the patients after a seven-month follow-up period.36 Moreover, they reported positive effects of exercise training on physical and psychosocial functioning of children with congenital heart disease.36
The improvements in exercise capacity (VO2peak) after exercise training could be explained by improvements on several factors. As described above, VO2peak is dependent on cardiac, pulmonary and muscular function. Improvements have been reported after exercise training for all three domains (figure 1); however, the effects of exercise training on muscular function in patients with a Fontan circulation are not yet well established.17
During submaximal exercise, heart rates of children with a Fontan circulation were decreased, whereas oxygen uptake did not change, increasing the oxygen pulse. An increased oxygen pulse is a reflection of an increased stroke volume and/or an increased peripheral oxygen extraction. Exercise training did not improve arterial oxygen saturation, or peak heart rate.
Practical implications
Exercise training seems to improve cardiopulmonary fitness in patients with a Fontan circulation with a stable haemodynamic condition. The training programme should be preceded by a maximal exercise test to screen for possible contraindications for exercise training.35 The prescribed exercise intensity should be low to moderate (i.e. 50 to 80% of Vo2peak), the sessions should last between 20 and 45 minutes, and a training programme should last for at least two to three months. The additive effect of light resistance exercise is unclear. Exercise training programmes should be evaluated using mode specific ergometers (e.g. running-based programmes should be evaluated using a treadmill test).
Directions for further research
Studies of the effect of exercise training on patients with a Fontan circulation have only recently been performed. Only six small studies have been conducted that focus on outcomes of physical performance measures such as VO2peak and pulmonary function. One study incorporated a functional outcome measure, the six-minute walk test.27 To date, the effects of exercise training on perceived competence, self-esteem, physical activity and health-related quality of life have not been studied.
Studies with a more rigorous research design (i.e. larger sample size, control group, blinded observers, etc) and a longer follow-up are indicated. In addition, the effect of exercise training on peripheral muscle function needs further study.
Conclusion
Based on these six studies, training programmes in Fontan patients with a stable haemodynamic status are safe, result in improved aerobic capacity, ventilatory anaerobic threshold, and respiratory indices, and can be performed without adverse effects. No significant effects of exercise training on oxygen saturation and peak heart rate were reported in these studies. After training, exercise capacity was still significantly lower than those reported in healthy children. More research is needed to establish the optimal exercise mode, and the effects of exercise training on cardiac and peripheral muscle function, physical activity, and health-related quality of life.
References
- 1.Hoffman JI, Kaplan S. The incidence of congenital heart disease. J Am Coll Cardiol 2002;39:1890-900. [DOI] [PubMed] [Google Scholar]
- 2.Fontan F, Baudet E. Surgical repair of tricuspid atresia. Thorax 1971;26:240-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Gewillig M. Ventricular dysfunction of the functionally univentricular heart: management and outcomes. Cardiol Young 2005; 15(Suppl 3):31-4. [DOI] [PubMed] [Google Scholar]
- 4.Takken T, Tacken MHP, Blank AC, Hulzebos EH, Strengers JLM, Helders PJM. Exercise limitations in patients with a Fontan circulation: a review. J Cardiovasc Med (In Press). [DOI] [PubMed] [Google Scholar]
- 5.Fick A. Ueber die Messung des Blutquantums in den Herzventrikeln. Sitx. der Physik-Med. Ges. Wurzburg 1870;2:16 [Google Scholar]
- 6.Rhodes J, Garofano RP, Bowman FO Jr, Grant GP, Bierman FZ, Gersony WM. Effect of right ventricular anatomy on the cardiopulmonary response to exercise. Implications for the Fontan procedure. Circulation 1990;81:1811-7. [DOI] [PubMed] [Google Scholar]
- 7.Stromvall Larsson E, Eriksson BO. Haemodynamic adaptation during exercise in fontan patients at a long-term follow-up. Scand Cardiovasc J 2003;37:107-12. [DOI] [PubMed] [Google Scholar]
- 8.Cortes RG, Satomi G, Yoshigi M, Momma K. Maximal hemodynamic response after the Fontan procedure: Doppler evaluation during the treadmill test. Pediatr Cardiol 1994;15:170-7. [DOI] [PubMed] [Google Scholar]
- 9.Driscoll DJ, Danielson GK, Puga FJ, Schaff HV, Heise CT, Staats BA. Exercise tolerance and cardiorespiratory response to exercise after the Fontan operation for tricuspid atresia or functional single ventricle. J Am Coll Cardiol 1986;7:1087-94. [DOI] [PubMed] [Google Scholar]
- 10.Senzaki H, Masutani S, Ishido H, Taketazu M, Kobayashi T, Sasaki N, et al. Cardiac rest and reserve function in patients with Fontan circulation. J Am Coll Cardiol 2006;47:2528-35. [DOI] [PubMed] [Google Scholar]
- 11.Ohuchi H. Cardiopulmonary response to exercise in patients with the Fontan circulation. Cardiol Young 2005;15(Suppl 3):39-44. [DOI] [PubMed] [Google Scholar]
- 12.Takken T, Tacken MHP, Blank AC, Hulzebos HJ, P.J.M. H, Strengers JLM. Comparative Exercise Physiology in Pediatric Patients with Congenital Heart Disease: Fontan versus Tetralogy of Fallot. (Submitted) [Google Scholar]
- 13.Stromvall-Larsson ES, Eriksson BO, Sixt R. Decreased lung function and exercise capacity in Fontan patients. A long-term follow-up. Scand Cardiovasc J 2003;37:58-63. [DOI] [PubMed] [Google Scholar]
- 14.Matthews IL, Fredriksen PM, Bjornstad PG, Thaulow E, Gronn M. Reduced pulmonary function in children with the Fontan circulation affects their exercise capacity. Cardiol Young 2006;16:261-7. [DOI] [PubMed] [Google Scholar]
- 15.Schulze-Neick I, Hartenstein P, Li J, Stiller B, Nagdyman N, Hubler M, et al. Intravenous sildenafil is a potent pulmonary vasodilator in children with congenital heart disease. Circulation 2003; 108(Suppl 1):II167-73. [DOI] [PubMed] [Google Scholar]
- 16.Grant GP, Mansell AL, Garofano RP, Hayes CJ, Bowman FO, Jr, Gersony WM. Cardiorespiratory response to exercise after the Fontan procedure for tricuspid atresia. Pediatr Res 1988;24:1-5. [DOI] [PubMed] [Google Scholar]
- 17.Brassard P, Bedard E, Jobin J, Rodes-Cabau J, Poirier P. Exercise capacity and impact of exercise training in patients after a Fontan procedure: a review. Can J Cardiol 2006;22:489-95. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Inai K, Saita Y, Takeda S, Nakazawa M, Kimura H. Skeletal muscle hemodynamics and endothelial function in patients after Fontan operation. Am J Cardiol 2004;93:792-7. [DOI] [PubMed] [Google Scholar]
- 19.Mertens L, Reybrouck T, Eyskens B, Daenen W, Gewillig M. Slow kinetics of oxygen uptake in patients with a Fontan-type circulation. Pediatr Exerc Sci 2003;15:146-155. [Google Scholar]
- 20.Witzel C, Sreeram N, Coburger S, Schickendantz S, Brockmeier K, Schoenau E. Outcome of muscle and bone development in congenital heart disease. Eur J Pediatr 2006;165:168-74. [DOI] [PubMed] [Google Scholar]
- 21.Lewis SF, Taylor WF, Graham RM, Pettinger WA, Schutte JE, Blomqvist CG. Cardiovascular responses to exercise as functions of absolute and relative work load. J Appl Physiol 1983;54:1314-23. [DOI] [PubMed] [Google Scholar]
- 22.Picchio FM, Giardini A, Bonvicini M, Gargiulo G. Can a child who has been operated on for congenital heart disease participate in sport and in which kind of sport? J Cardiovasc Med (Hagerstown) 2006;7:234-8. [DOI] [PubMed] [Google Scholar]
- 23.Brassard P, Poirier P, Martin J, Noel M, Nadreau E, Houde C, et al. Impact of exercise training on muscle function and ergoreflex in Fontan patients: a pilot study. Int J Cardiol 2006;107:85-94. [DOI] [PubMed] [Google Scholar]
- 24.Myers J, Prakash M, Froelicher V, Do D, Partington S, Atwood JE. Exercise capacity and mortality among men referred for exercise testing. N Engl J Med 2002;346:793-801. [DOI] [PubMed] [Google Scholar]
- 25.Nixon PA, Orenstein DM, Kelsey SF, Doershuk CF. The prognostic value of exercise testing in patients with cystic fibrosis. N Engl J Med 1992;327:1785-8. [DOI] [PubMed] [Google Scholar]
- 26.Gulati M, Black HR, Shaw LJ, Arnsdorf MF, Merz CN, Lauer MS, et al. The prognostic value of a nomogram for exercise capacity in women. N Engl J Med 2005;353:468-75. [DOI] [PubMed] [Google Scholar]
- 27.Moalla W, Gauthier R, Maingourd Y, Ahmaidi S. Six-minute walking test to assess exercise tolerance and cardiorespiratory responses during training program in children with congenital heart disease. Int J Sports Med 2005;26:756-62. [DOI] [PubMed] [Google Scholar]
- 28.Rhodes J, Curran TJ, Camil L, Rabideau N, Fulton DR, Gauthier NS, et al. Impact of cardiac rehabilitation on the exercise function of children with serious congenital heart disease. Pediatrics 2005;116:1339-45. [DOI] [PubMed] [Google Scholar]
- 29.Moalla W, Maingourd Y, Gauthier RM, Cahalin LP, Tabka Z, Ahmaidi S. Effect of exercise training on respiratory muscle oxygenation in children with congenital heart disease. Eur J Cardiovasc Prev Rehabil 2006;13:604-11. [DOI] [PubMed] [Google Scholar]
- 30.McCall R, Humphrey R. Exercise training in a young adult late after a fontan procedure to repair single ventricle physiology. J Cardiopulm Rehabil 2001;21:227-30. [DOI] [PubMed] [Google Scholar]
- 31.Minamisawa S, Nakazawa M, Momma K, Imai Y, Satomi G. Effect of aerobic training on exercise performance in patients after the Fontan operation. Am J Cardiol 2001;88:695-8. [DOI] [PubMed] [Google Scholar]
- 32.Baquet G, van Praagh E, Berthoin S. Endurance training and aerobic fitness in young people. Sports Med 2003;33:1127-43. [DOI] [PubMed] [Google Scholar]
- 33.Stromme SB, Ingjer F, Meen HD. Assessment of maximal aerobic power in specifically trained athletes. J Appl Physiol 1977;42:833-7. [DOI] [PubMed] [Google Scholar]
- 34.Opocher F, Varnier M, Sanders SP, Tosoni A, Zaccaria M, Stellin G, et al. Effects of aerobic exercise training in children after the Fontan operation. Am J Cardiol 2005;95:150-2. [DOI] [PubMed] [Google Scholar]
- 35.Paridon SM, Alpert BS, Boas SR, Cabrera ME, Caldarera LL, Daniels SR, et al. Clinical stress testing in the pediatric age group: a statement from the American Heart Association Council on Cardiovascular Disease in the Young, Committee on Atherosclerosis, Hypertension, and Obesity in Youth. Circulation 2006;113:1905-20. [DOI] [PubMed] [Google Scholar]
- 36.Rhodes J, Curran TJ, Camil L, Rabideau N, Fulton DR, Gauthier NS, et al. Sustained effects of cardiac rehabilitation in children with serious congenital heart disease. Pediatrics 2006;118:e586-93 [DOI] [PubMed] [Google Scholar]