

Abstract
The timing and appropriateness of surgical treatment of sigmoid diverticular disease remain a topic of controversy. We have reviewed the current literature on this topic, focusing on issues related to the indications and types of surgery. Current evidence would suggest that elective surgery for diverticulitis can be avoided in patients with uncomplicated disease, regardless of the number of recurrent episodes. Furthermore, the need for elective surgey should not be influenced by the age of the patient. Operation should be undertaken in patients with severe attacks, as determined by their clinical and radiological evaluation.
Keywords: Sigmoid diverticulitis, Surgical management, Diagnosis, Elective surgery
Magnitude of the Problem
Diverticular disease, either diverticulosis or diverticulitis, was regarded as a surgical curiosity in the 19th surgery, but over the past 100 years, its prevalence in Western countries has increased dramatically. In the US, an individual’s risk for developing diverticular disease approaches 50% by age 60.1 Diverticulitis, defined as inflammation and infection related to diverticula, occurs in 20 to 30% of patients with diverticulosis and is one of the most common indications for gastrointestinal tract-related hospitalizations. One in four of these patients presenting with diverticulitis will require an emergency operation because of perforation, peritonitis, or systemic complications. At present, diverticulitis is the associated diagnosis for one third of all colostomies and/or colon resections.2 As such, diverticulitis is one of the five most costly gastrointestinal disorders affecting the US population.3
Etiology
Colonic diverticula tend to develop in the areas of weakness in the colonic wall, most frequently at the sites of penetration of the wall by blood vessels.4 These outpouchings of mucosa and peritoneum are of the pulsion type and are thought to be caused by an increase in the intraluminal pressure within the colonic wall in affected individuals (Fig. 1).
Figure 1.
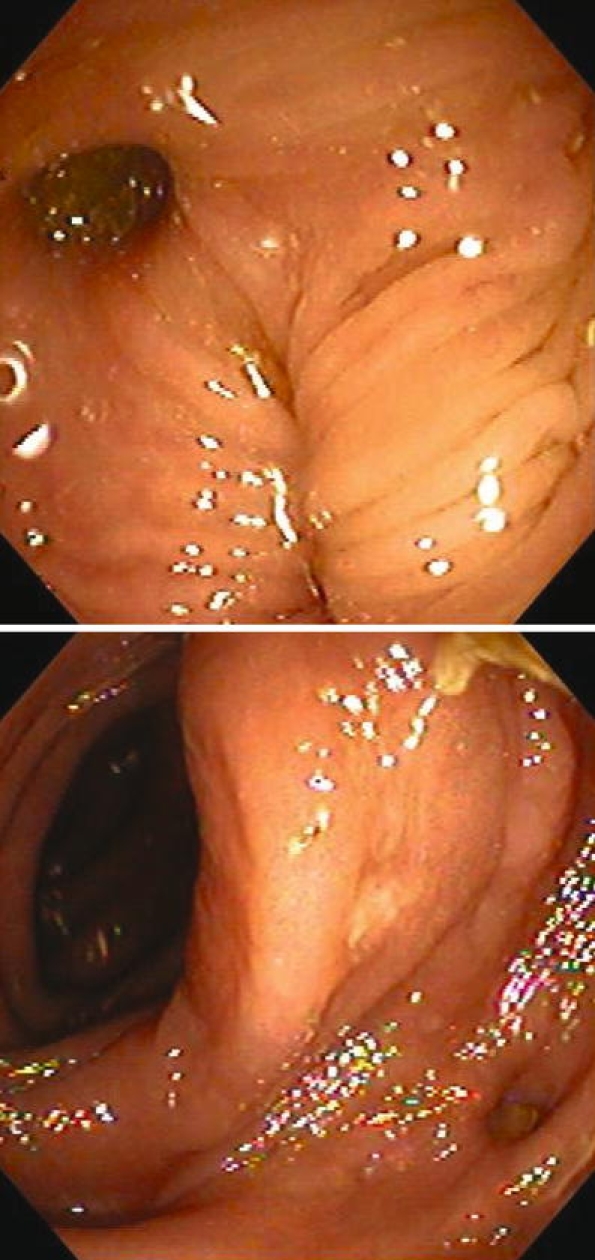
Endoscopic images of diverticuli. Colonoscopy can be rather difficult when several diverticula are encountered because of increased colonic tortuosity and lack of distensibility.
It is thought that a low intake of dietary fiber and resultant decrease in stool bulk predisposes those in Western societies to an elevation in colonic pressure. Some authors attribute the high rate of diverticular disease to the development of the roller mills during the last half of the 19th century, causing the grains to be crushed so effectively as to nearly eliminate all of the cellulose from the Western diet.5 Despite significant supporting evidence for fiber and its role in the development of diverticulosis, no study to date has demonstrated that a high fiber diet can reverse this process or reduce the incidence of complications in cases of established diverticulosis.6
In addition to dietary intake, other factors have been implicated in the development of diverticular disease. Most studies report that diverticular disease is more common in the elderly, especially elderly women, and in patients who smoke cigarettes or drink alcohol.7 Sigmoid colon specimens from patients with diverticulosis have been found to have increased in vitro sensitivity to acetylcholine, as well as reduced smooth muscle choline acetyltransferase activity and upregulation of smooth muscle muscarinic M3 receptors.8 The significance of these biochemical characteristics still needs to be elucidated, but the differences suggest that there are underlying physiological abnormalities that may predispose to the development and progression of diverticular disease.
Clinical Presentation and Evaluation
The clinical presentations of diverticular disease range from asymptomatic diverticulosis, diverticulosis with periodic spasmodic abdominal pain and bloating, diverticulosis with hemorrhage, and finally, diverticulitis. Although diverticula can occur in any portion of the colon, this review will only focus on sigmoid diverticulitis, by far, the most common site for this disease process.
Most patients with diverticulitis present with symptoms of left lower quadrant abdominal pain, fever, and leukocytosis (Table 1). Additional symptoms of acute sigmoid diverticulitis may include nausea, vomiting, change in bowel habits, urinary frequency, and/or dysuria.1 In cases of clear-cut diverticulitis based upon the clinical picture, one can manage the patient without any imaging studies. In many cases, especially in those with severe symptoms and potential complicated diverticulitis, computed tomography (CT) scanning should probably be performed. The value of CT scanning is the ability to confirm the diagnosis and confidently stratify the severity of the disease process, differentiating mild, localized inflammation from advanced inflammation with abscess formation and/or distant extension.
Table 1.
Clinical Symptoms of Diverticulitis
| Symptoms | Frequency (%) |
|---|---|
| Left lower quadrant pain | 93–100 |
| Leucocytosis | 69–83 |
| Fever | 57–100 |
| Nausea | 10–30 |
| Vomiting | 15–25 |
| Constipation | 10–30 |
| Diarrhea | 5–15 |
| Dysuria | 5–20 |
| Urinary frequency | 6–25 |
Before the advent of CT, the contrast enema was the primary tool in the evaluation of colonic diverticular disease. However, CT scans have largely replaced barium enema as the preferred imaging modality to evaluate patients with suspected diverticulitis. The use of CT scanning has been justified by several studies from the radiological literature, demonstrating a high sensitivity (97%) and specificity (100%) for diverticulitis (Fig. 2). Contrast enema, on the other hand, has a sensitivity of only 82% and a specificity of 81% for diverticulitis.9
Figure 2.
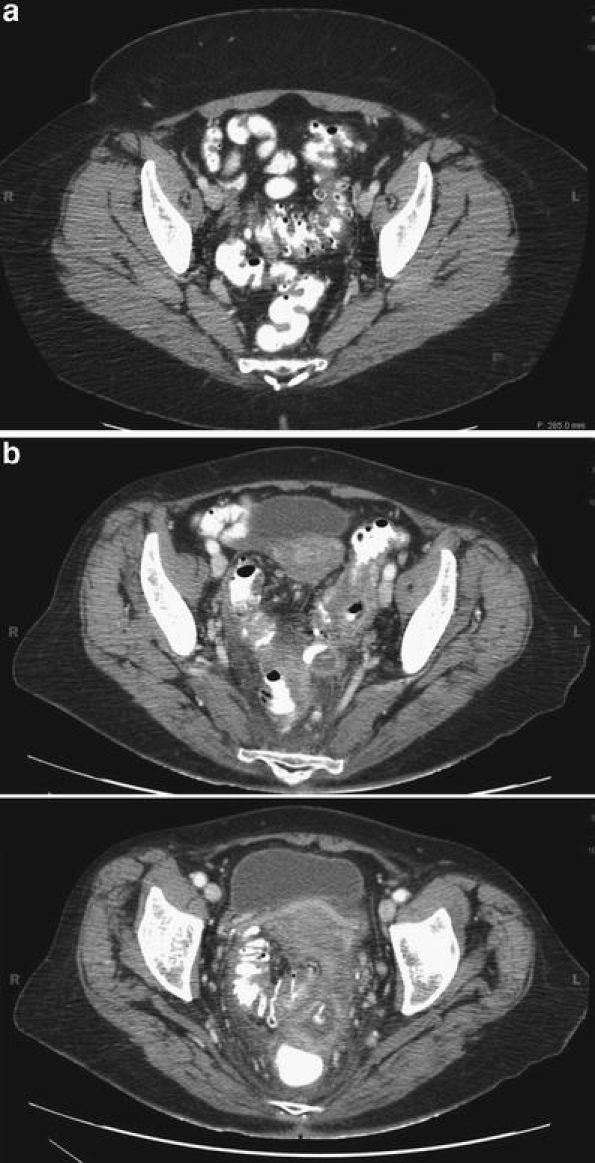
a Computed tomography scan images of a patient who presented with uncomplicated diverticulitis that was subsequently treated successfully with antibiotics. Note the thickening of the sigmoid colon, yet the lack of any extraluminal fluid or air. b Computed tomography scan images of a patient who presented with complicated diverticulitis and an extraluminal fluid collection that did not resolve with attempted CT-guided drainage an required an eventual sigmoid colectomy.
Classification
There are two commonly utilized classifications of diverticulitis. The European Association for Endoscopic Surgeons developed a classification scheme based upon the severity of its clinical presentation.10 In this system, diverticulitis is divided into symptomatic uncomplicated disease, recurrent symptomatic disease, and complicated disease (Table 2).
Table 2.
Clinical Classification of Diverticulitis (Adapted from Kohler et al. 10)
| Grade | Clinical Description | Symptoms |
|---|---|---|
| I | Symptomatic uncomplicated disease | Fever, crampy abdominal pain, CT evidence of diverticulitis |
| II | Recurrent symptomatic disease | Recurrence of above |
| III | Complicated disease | Hemorrhage |
| Abscess | ||
| Phlegmon | ||
| Perforation | ||
| Purulent and fecal peritonitis | ||
| Stricture | ||
| Fistula | ||
| Obstruction |
Another classification system was developed by Hinchey et al.11 and is used to describe the stages of complicated diverticulitis (Table 3). This scheme allows for good communication among surgeons when it comes to describing the various degrees of diverticular perforation, ranging from a localized perforation with a small abscess to generalized fecal peritonitis. Clearly, the proper surgical approach will vary depending upon the Hinchey stage.
Table 3.
Hinchey Classification of Complicated Diverticulitis (Adapted from Hinchey et al.11)
| Stage | Description |
|---|---|
| I | Pericolic or mesenteric abscess |
| II | Walled off pelvic abscess |
| III | Generalized purulent peritonitis |
| IV | Generalized fecal peritonitis |
We will refer to both of these classifications when discussing the appropriate management of this disease. Yet another classification, developed by Ambrosetti et al.12, is based upon the CT findings. The criteria of Ambrosetti et al. are being increasingly utilized to stratify patients into optimal pathways for management (Table 4). Thus, patients with mild disease are likely to be successfully managed with intravenous antibiotics, whereas percutaneous drainage and surgery is generally indicated for cases of complicated diverticulitis.
Table 4.
Ambrosetti’s CT Staging of Diverticulitis (Adapted from Ambrosetti et al.12)
| Mild Diverticulitis | Severe Diverticulitis |
|---|---|
| Localized sigmoid wall thickening (<5 mm) | Abscess |
| Inflammation of pericolic fat | Extraluminal air |
| Extraluminal contrast |
Management of Complicated Diverticulitis
Surgical intervention is rarely indicated in cases of acute diverticulitis because most of these cases will resolve with appropriate antibiotic management. Operations are reserved for cases of complicated diverticulitis, i.e., patients with perforation and peritonitis, abscess formation, fistula, or obstruction. Although this may seem clear-cut, decisions regarding if and when to operate patients with diverticulitis remain a topic of significant debate.
Operation is clearly indicated when the patient presents with perforation and diffuse peritonitis, whether it is purulent or feculent (Hinchey stages III and IV). However, the ideal surgical procedure in such cases of perforation remains a matter of debate. The possible operations advocated range from a simple washout of the abdomen with drainage, as described in a few case reports from Scotland and France, to primary resection with a Hartmann pouch, primary resection with anastomosis, diverting ileostomy, and finally, a primary resection with anastomosis and no temporary stoma. Of these,1,13,14 American surgeons are most likely to perform the Hartmann procedure, which has been advocated as the standard of care for perforated diverticulitis.1 The Hartmann’s resection has proven to be a safe and effective approach, and is based upon the idea that an anastomosis in the setting of acute infection/inflammation is dangerous and associated with a high rate of suture line breakdown.
A simple washout without resection would not be considered an appropriate approach because ongoing infection/inflammation of the involved bowel is likely to occur. There is a paucity of data to support a minimalist, simple washout approach; there are only 18 case reports in the literature describing the technique and its results.13,14 On the other hand, the practice of routine stomas in operations for acute diverticulitis may not be justified. Belmonte et al.15 looked at 277 consecutive patients treated for acute diverticular disease at the University of Minnesota, both urgently and electively. Of these, 88% had a primary anastomosis, most of them without diversion. They found that primary anastomosis was quite safe, with an overall 4% leak rate. Interestingly, none of these leaks were in their subset of patients with Hinchey stage IV diverticulitis, a group that comprised 9% of their total study population.
A systematic literature review of 50 studies comparing a Hartmann’s procedure to a primary resection with anastomosis for perforated diverticulitis found 569 reported cases of primary anastomoses. The reported mortality and morbidity in the patients with an anastomosis was the same as in the patients who underwent the Hartmann’s procedure.16 These data suggest that in a select group of patients undergoing surgery in the acute stage of diverticulitis, an anastomosis is probably safe, even in the milieu of feculent peritonitis.
These data are intriguing, but must be viewed with caution, especially in the case of a very sick or toxic patient with multiorgan system failure and/or shock. In the absence of randomized controlled studies, we still recommend the Hartmann’s procedure in patients with significant purulent or feculent peritonitis, and those patients with any instability related to the systemic effects of sepsis. However, in a patient who is clinically stable, a primary anastomosis at the first operation can be performed even in the setting of perforation (Fig. 3).
Figure 3.

Gross specimen of the sigmoid colon that was resected from a patient who presented with freely perforated diverticulitis (Hinchey III). Proximal margin extends to the area where the diverticuli end, and the distal margin is at the rectum.
Mention should be made of the meticulous surgical technique that must be used in this situation. The splenic flexure of the colon may need to be mobilized to ensure a tension-free anastomosis. One should imagine the rectum collapsing back into the pelvis with the patient standing upright when deciding on whether the bowel ends are truly free of tension. The margins of resection must be clearly viable with regard to vascularity. Finally, it may be best to avoid the crossed staple lines inherent to the double-stapled technique. Either a double pursestring technique with a stapled end-to-end anastomosis or a standard handsewn anastomosis are preferred when operating in an inflamed milieu.
Preventive Surgery
The question of when to recommend elective, preventive surgery for patients with diverticulitis remains very controversial. Current American Society of Colon and Rectal Surgeons (ASCRS) guidelines suggest preemptive surgery for any patient who has had two attacks of acute diverticulitis, with the intention of preventing another attack that could present with perforation and would necessitate a stoma.1 This recommendation for surgery after the second episode of diverticulitis is based on the data published in 1969 by Parks17 showing that the mortality rate for each subsequent attack of diverticulitis increases from 4.7% during the first admission to 7.8% during each subsequent admission. Parks is also widely quoted for stating that each subsequent episode of diverticulitis is less likely to respond to medical therapy, with a 70% response after the first episode vs 6% response after the third episode.1 However, there are little data to support this concept of poor response to medical treatment in subsequent attacks of diverticulitis. Furthermore, the advent of CT scanning and better antibiotics has improved nonoperative management of these patients. In a modern series of 673 patients with diverticular disease, only 3% of patients required emergency operations during a follow up of 10 years.18 Another 10-year study of 366 patients showed that recurrence was not associated with an increased rate of either complications or less successful medical management.19
Looking at the issue from another angle, Somasekar et al.20 reviewed 108 patients admitted with complicated diverticulitis. Almost all of them (104) required emergency surgery. Interestingly, only 26% of these patients were previously diagnosed with diverticular disease and only three patients had been admitted in the past with a prior episode of acute diverticulitis. In other words, only 2.7% of patients in this group would have benefited from an elective resection. Complications would still have occurred in 92.6% of patients in whom these attacks happened de novo.
Thus, it appears that elective resection might have little impact on the incidence of patients requiring emergency procedures because most of these occur with the first attack of diverticulitis. Subsequent attacks of diverticulitis in the same patient seem to be akin to their previous ones, suggesting that specific patients are predisposed to a set pattern of diverticulitis, and once settled into this pattern they stay within it. The threat of the colostomy bag to a patient who has been successfully managed medically during two previous attacks may be unwarranted and misleading.
In addition, it is important to recognize that elective surgery for diverticulitis is not without complications. Bookey et al.21 demonstrated that elective diverticular disease resection is associated with higher rates of morbidity and mortality than elective colorectal carcinoma resection, with the mortality rate increasing from 0 to 15% with advancing age. Furthermore, colectomy is not a guaranteed cure for diverticulitis, with recurrence rates varying from 3 to 13%. These rates have improved, however, with the recognition that the chances of recurrence are fourfold higher if a colosigmoid anastomosis is performed, emphasizing the importance of resecting the entire sigmoid colon in an operation for diverticulitis.22
With these conflicting data in mind, we maintain that the patients with uncomplicated diverticulitis can be managed nonoperatively regardless of the number of recurrent episodes. Patients who develop complications, such as fistulas, obstruction, or nonresolving smoldering disease, are best managed with surgical resection. Elective surgery may also be offered to patients who have had two or more episodes of severe diverticulitis, as determined by their clinical presentation and CT grade. In addition, elective surgery may be justified in patients with limited access to medical care or in those who are concerned about the negative impact of repeated illnesses with regard to work productivity and/or psychosocial issues.
In elective or semielective circumstances, both open and laparoscopic sigmoid resection with a primary anastomosis have been considered as acceptable methods of treatment.23 Laparoscopy has been shown to be associated with an approximate 10% rate of conversion to open surgery. Interestingly, no direct relationship has been found between the number of attacks of diverticulitis or the timing after an acute attack with regard to complications or conversion rates with laparoscopic colectomy.24
Diverticulitis in Young Men
Many authors believe that diverticulitis is a more virulent disease in younger patients. As such, it has been argued that all patients younger than 50 should undergo elective colon resection after an initial attack of diverticulitis.1,25 This argument arose from studies in the pre-CT era, which were replete with data, indicating a high risk of surgical intervention in young patients eventually diagnosed with diverticulitis. Subsequent authors have argued that these earlier studies were flawed because of a significant rate of unnecessary laparotomies in the younger patients because of erroneous preoperative diagnoses of appendicitis.26 Vignati et al.27 were among the first to challenge the concept that diverticulitis in the young is a more virulent disease. These authors surveyed 40 patients under the age of 50 that where treated with intravenous antibiotics and bowel rest and found that at a 5- to 9-year follow-up, none of these patients required colostomies. One third of them did undergo surgery, but most of these procedures where either elective or, if urgent, still conducive to a successful primary anastomosis.
Guzzo et al.26 performed a retrospective review of 762 patients with diverticulitis treated at their institution from 1990–2000 and found that 76% of the patients under age 50 improved with antibiotics and did not require surgery during their first attack. These rates did not differ from the rates of surgery in the elderly patients. Of the patients treated nonoperatively, only four patients had a recurrence requiring surgery at a later time and only one needed a colostomy. Thirty-eight additional patients underwent preemptive elective surgery based upon their surgeon’s recommendation. One hundred fifty-five patients, 60% of the entire group, did not require surgery at all.26
A prospective study from Switzerland followed 118 patients who had their first attack of diverticulitis and found that recurrence rates in the younger patients were similar to those seen in the older patients, once stratified by their CT severity.28
Based upon these studies, we believe that young patients should generally be treated using the same criteria as older patients, and that the there is no justification for the routine recommendation for surgery after a single attack of diverticulitis in young patients. Elective preemptive surgery should be reserved for those who had at least two episodes of severe diverticulitis, and this decision should be supported by CT scan documentation of prior complicated disease.
Fistulas
As we succeed with the nonoperative treatment of acute diverticulitis, the incidence of fistulas appears to be increasing, reported to occur in approximately 12% of patients.29 Colovesical fistulas account for two thirds of the cases, followed by colovaginal, colocutaneous, and enterocolic cases.30 These patients can present a significant challenge to the surgeon. Some fistulas will close spontaneously as the inflammatory process resolves. Therefore, a selective approach should be used, in which operation is offered to those patients with persistent symptoms after 5–6 months after an acute attack. The most commonly reported symptoms in this group of patients include abdominal pain (43%), pneumaturia (43%), cystitis (40%), fecaluria (38%), diarrhea (15%), and hematuria (5%).31
In the operating room, the surgeon should expect a significant desmoplastic reaction and a contained abscess cavity in the area of fistulization. It may be prudent to place ureteral stents before the procedure, although most fistulas to the bladder will be at the dome and away from the trigone region, allowing relatively safe access for identification, dissection, and closure. Most of these cases should be amenable to resection with primary anastomosis, avoiding the need for a temporary stoma.32
In expert hands, a colectomy can be accomplished by either an open or laparoscopic approach.33 Some authors suggest that these procedures are best performed by surgeons whose main interest focuses on colon and rectal surgery. A study from McGill University comparing outcomes of surgery for diverticulitis-induced fistulas found that colorectal surgeons performed less diverting Hartmann’s and colostomies (5 vs 27%), and had a lower rate of complications, including wound infections and anastomotic leaks.31 It is not clear, however, whether the data from this small study of 121 patients are applicable to all surgeons in all centers.
Diverticulitis in the Immunocompromised Patient
Diverticulitis in immunocompromised patients can be virulent because there is an increased likelihood of free perforation and fecal peritonitis. In addition, the clinical presentation of these patients often underestimates the severity of their disease.34 Marked differences have also been noted in the response of these patients to medical treatment. In the nonimmunocompromised group one should expect that 75% of patients will respond to antibiotics. In contrast, a very large percentage of immunocompromised patients will fail standard, nonoperative treatment.35 As such, most of these patients require urgent surgical intervention, and this is associated with a significantly higher mortality rate: 39 vs 2% in noncompromised patients.35 Given these data, most authors and the ASCRS recommend elective sigmoid resection after the first episode of diverticulitis in immunocompromised patients.1,34–36
Conclusion
The management of patients with sigmoid diverticulitis is still evolving. We should continue to constantly reassess the surgical dogma regarding the appropriate treatment of this common disease entity. Clearly, a randomized controlled study comparing the Hartmann’s procedure to primary anastomosis in the setting of perforated diverticulitis would be worthwhile. It is becoming increasingly clear that mandatory operations may not be warranted in young patients or those with two episodes of diverticulitis. As in other areas of clinical surgery, we must tailor our treatment to the specific situation for each individual patient.
References
- 1.Wong WD, Wexner SD, Lowry A, et al. Practice parameters for the treatment of sigmoid diverticulitis-supporting documentation. The Standards Task Force. The American Society of Colon and Rectal Surgeons. Dis Colon Rectum 2000;43:290–297. [DOI] [PubMed]
- 2.Salem L, Flum DR. Primary anastomosis or Hartmann’s procedure for patients with diverticular peritonitis? A systematic review. Dis Colon Rectum 2004;47:1953–1964. [DOI] [PubMed]
- 3.American Gastroenterological Association. The Burden of Gastrointestinal Diseases. Bethesda, MD: American Gastroenterological Association, 2001.
- 4.Stollman L, Raskin J. Diverticular disease of the colon. J Clin Gastroenterol 1999;29:241–252. [DOI] [PubMed]
- 5.Painter NS, Burkitt DP. Diverticular disease of the colon: a deficiency disease of Western civilization. BMJ 1971;1:450. [DOI] [PMC free article] [PubMed]
- 6.Ornstein MH, Littlewood ER, Baird IM, Fowler J, Cox AG. Are fiber supplements really necessary in diverticular disease of the colon? A controlled clinical trial. Br Med J 1981;282:1353–1356. [DOI] [PMC free article] [PubMed]
- 7.Papagrigoriades S, Macey L, Bourantas N, Rennie JA. Smoking may be associated with complications in diverticular disease. Br J Surg 1999;86:923. [DOI] [PubMed]
- 8.Golder M, Burleigh DE, Belai A, et al. Smooth muscle cholinergic denervation hypersensitivity in diverticular disease. Lancet 2003;361:1945–1951. [DOI] [PubMed]
- 9.Lawrimore T, Rhea J. Computed tomography evaluation of diverticulitis. J Intensive Care Med 2004;19(4):194–204. [DOI] [PubMed]
- 10.Kohler L, Sauerland S, Neugebauer E, et al. E.A.E.S. consensus statement: diagnosis and treatment of diverticular disease. Results of a consensus conference. Surg Endosc 1999;13:430–436. [DOI] [PubMed]
- 11.Hinchey EJ, Schaal PGH, Richards GK. Treatment of perforated diverticular disease of the colon. Adv Surg 1978;12:85–109. [PubMed]
- 12.Ambrosetti P, Jenny A, Becker C, Terrier F, Morel P. Acute left colonic diverticulosis: compared performance of computed tomography and water-soluble contrast enema. Prospective evaluation of 420 patients. Dis Colon Rectum 2000;43:1363–1367. [DOI] [PubMed]
- 13.O’Sullivan GC, Murphy D, O’Brien M, Ireland A. Laparoscopic management of generalized peritonitis due to perforated colonic diverticula. Am J Surg 1996;171:432–434. [DOI] [PubMed]
- 14.Rizk N, Barat C, Faranda C, Catheline JM, Champault G. Traitement laparoscopique des peritonitis generalisees par perforation diverticulaire du colon sigmoide. A propos de dix cas. Chirurgie 1998;123:358–362. [DOI] [PubMed]
- 15.Belmonte C, Klas JV, Perez JJ, Wong WD, Rothenberger DA, Goldberg SM, Madoff RD. The Hartmann procedure: first choice or last resort in diverticular disease? Arch Surg 1996;131(6):612–617. [DOI] [PubMed]
- 16.Salem L, Flum DR. Primary anastomosis or Hartmann’s procedure for patients with diverticular peritonitis? A systematic review. Dis Colon Rectum 2004;47(11);1953–1964. [DOI] [PubMed]
- 17.Parks TG. Natural history of diverticular disease of the colon: a review of 521 cases. BMJ 1969;4:639–642. [DOI] [PMC free article] [PubMed]
- 18.Alexander J, Karl RC, Skinner DB. Results of changing trends in the surgical management of complications of diverticular disease. Surgery 1983;94:683–690. [PubMed]
- 19.Makela J, Vuolio S, Kiviniemi H, Laitinen S. Natural history of diverticular disease. When to operate? Dis Colon Rectum 1998;41(12):1523–1528. [DOI] [PubMed]
- 20.Somasekar K, Foster ME, Haray PN. The natural history of diverticular disease: is there a role for elective colectomy? J R Coll Surg Edinb 2002;47(2):481–484. [PubMed]
- 21.Bookey EL, Chapius PH, Pheils MT. Elective resection for diverticular disease and carcinoma. Comparison of postoperative morbidity and mortality. Dis Colon Rectum 1981;24:181–18. [DOI] [PubMed]
- 22.Thaler K, Baig MK, Berho M, Weiss E, Nogueras JJ, Arnaud JP, Wexner SD, Bergamaschi R. Determinants of recurrence after sigmoid resection for uncomplicated diverticulitis. Dis Colon Rectum 2003;46(3):385–388. [DOI] [PubMed]
- 23.Jacobs M, Verdeja JC, Goldstein HS. Minimally invasive colon resection (laparoscopic colectomy). Surg Laparosc Endosc 1991;1:144–150. [PubMed]
- 24.Natarjan S, Ewings EL, Vega RJ. Laparoscopic sigmoid colectomy after acute diverticulitis: when to operate? Surgery 2004;136:725–730. [DOI] [PubMed]
- 25.Eusebio EB, Eisenberg MM. Natural history of diverticular disease of the colon in young patients. Am J Surg 1973;125:308–311. [DOI] [PubMed]
- 26.Guzzo J, Hyman N. Diverticulitis in young patients: Is resection after a single attack always warranted? Dis Colon Rectum 2004;47:1187–1191. [DOI] [PubMed]
- 27.Vignati, PV, Welch JP, Cohen JL. Long-term management of diverticulitis in young patients. Dis Colon Rectum 1995;38(6):627–629. [DOI] [PubMed]
- 28.Chateums RC, Ambrosetti P, Ludwig A, Mermillod B, Morel Ph, Soravia C. Long term follow up after first acute episode of sigmoid diverticulitis: is surgery mandatory? A prospective study of 118 patients. Dis Colon Rectum 2002;45(7):962–966. [DOI] [PubMed]
- 29.Novak L, Hyman N. Surgery for complicated diverticulitis. Semin Colon Rectal Surg 2000;11(4):214–217.
- 30.Bahadursingh A, Virgo K, Kaminski D, Longo W. Spectrum of disease and outcome of complicated diverticular disease. Am J Surg 2003;186:696–701. [DOI] [PubMed]
- 31.Di Carlo A, Andtbacka R, Shrier I, Belliveau P, Trudel J, Stein B, Gordon P, Vasilevsky C. The value of specialization–is there an outcome difference in the management of fistulas complicating diverticulitis. Dis Colon Rectum 2001;44(10):1456–1463. [DOI] [PubMed]
- 32.Woods RJ, Lavery IC, Fazio VW, Jagelman DG, Weakley FL. Internal fistulas in diverticular disease. Dis Colon Rectum 1988;31:591–596. [DOI] [PubMed]
- 33.Bartus C, Lipof T, Shahbaz Sarwar C, Vignati P, Johnson K, Sardella W, Cohen J. Colovesical fistula: not a contraindication to elective laparoscopic colectomy. Dis Colon Rectum 2005;48(2):233–236. [DOI] [PubMed]
- 34.Detry O, Defraigne J, Meurisse M. Acute diverticulitis in heart transplant recipients. Transpl Int 1996;9:376–379. [DOI] [PubMed]
- 35.Perkins JD, Shield CF, Chang FC, Farha GJ. Acute diverticulitis. Comparison of treatment in immunocompromised and nonimmunocompromised patients. Am J Surg 1984;148:745–748. [DOI] [PubMed]
- 36.Efron JE, Nogueras JJ. Controversies in diverticular disease. Indications for surgery and surgical options. Semin Colon Rectal Surg 2000;11(4):206–213.