

Abstract
Aims
In this study we examined three parenting dimensions (involvement, autonomy, and limit-setting) and three potential determinants (maternal addiction, low SES and its correlates, and mothers’ perceptions of their children’s maladjustment) in order to disentangle features of parenting that are uniquely related to maternal addiction from those related to contextual determinants. We also examined conditional effects of low SES and its correlates on parenting.
Design
Based on a literature review and predictions arising from an ecological model of parenting, we expected that maternal addiction would be related with problems in parental involvement, but that the other parenting dimensions would be related with mothers’ perceptions of children’s maladjustment and low SES. Accordingly, we examined variance in each parenting dimensions accounted for by each of the three determinants, respectively.
Participants
Subjects included 120 (69 opiate-addicted and 51 SES-matched comparison) mothers with children under 16 years of age.
Measurements
Children’s maladaptive behavior was assessed with the Behavioral Assessment System for Children, and parental adjustment with the Parent Child Relationship Inventory.
Findings
Direct effect predictions were confirmed and two conditional effects involving single status and family size were also found.
Conclusions
Although many parenting problems have previously been attributed to maternal addiction, only parental involvement is directly related to being an addict; other parenting dimensions may be better explained by contextual factors.
Introduction
Addicted women’s parenting, in contrast with the parenting of non-addicted women, has been characterized in previous research by a wide range of deficits, including neglect, physical and emotional abuse, excessive control and punishment, inconsistent discipline and lack of emotional involvement (Mayes, 1995). Few studies, however, have simultaneously examined other factors associated with maternal addiction and parenting that might also contribute to addicted mothers’ parenting behaviors. An ecological model of parenting (Belsky, 1993) would suggest that addicted mothers’ parenting is also influenced by contextual factors such as low SES and children’s maladaptive behavior. To determine aspects of addicted women’s parenting that are uniquely attributed to their drug abuse versus those aspects attributable to contextual factors, we conducted a study of opiate-addicted mothers and demographically matched non-addicted comparison mothers. Guided by extant literature reviewed below, we focused on three dimensions of parenting—involvement, autonomy, and limit-setting—and on two potential contextual determinants of parental maladjustment—low SES and mothers’ perceptions of their children’s maladaptive behavior. We also examined conditional socio-demographic effects expected to influence the relationship between maternal addiction and parenting.
Rationale for direct effects
Maternal drug addiction has been unequivocally linked with parenting deficits. Parents who are identified as abusing and/or neglecting their children often have concurrent substance abuse problems (Murphy et al., 1991; Kelleher et al., 1994; Chaffin, Kelleher & Hollenberg, 1996; Hampton, Senatore & Gullotta, 1998). Parenting styles among opiate- and cocaine-addicted mothers often parallel dimensions of abuse and neglect, vacillating between authoritarian over-control and excessive permissiveness. The authoritarian style (Baumrind, 1971) has been characterized by over-involvement, harsh verbal criticism, extensive punishment, controlling approaches to discipline and exclusion of parenting support from other adults (Bauman & Dougherty, 1983; Deren, 1986; Mayes, 1995; Luthar & Suchman, 1999). The neglectful stance has been characterized by withdrawal, ambivalence, limited involvement and engagement, insecure attachment and diminished responsiveness (Davis, 1990; Mayes, 1995; Harden, 1998). Neglect has also recently emerged as the most prominent form of child maltreatment among mothers abusing illicit drugs (Chaffin et al., 1996; Egami et al., 1996; Harden, 1998; Besinger et al., 1999). Opiate-addicted mothers, in particular, have been described as less emotionally involved (Hans, 1992) and responsive (Bernstein et al., 1984) with infants and more provocative and threatening with school-aged children (Bauman & Dougherty, 1983).
Problems with inconsistent limit setting attributed to maternal addiction may actually be attributable to mothers’ perceptions of their children’s maladaptive behavior. The reciprocal relationship between parents’ perceptions of their children’s maladjustment (externalizing in particular) and discipline problems has been well documented in studies involving school-aged children (Cummings & Davies, 1994; Peterson et al., 1994; Eisenberg et al., 1999) and adolescents (Ge, 1995; Stice & Barrera, 1995).
The authoritarian and controlling parental stance attributed to maternal addiction may also be attributable to an opiate-addicted mothers’ concomitant membership in low socio-economic strata. Literature comparing low and high SES parents has clearly linked low SES with higher incidence rates of child abuse and more authoritarian, controlling, punitive and restrictive parenting styles (for a review, see Hoff-Ginsberg & Tardif, 1995; Sedlak & Broadhurst, 1996).
The few studies that have attempted to disentangle the effects of parental substance abuse from SES have yielded disparate results: Based on data from the National Institute of Mental Health (NIMH) Epidemiologic Catchment Area study, Chaffin and colleagues (1996) reported that, when parental substance abuse was held constant, links between low SES and child maltreatment disappeared entirely. Also based on data from the NIMH study, Egami and colleagues (1996) found that, after controlling for socio-demographic and psychiatric variables, illicit drug disorders were related to neglect but not abuse. In a third study, comparing mother–infant interactions of methadone-maintained versus comparison mothers, Bernstein and colleagues (1984) found that low SES and psychological characteristics of parents were better predictors of poor parenting interactions than opiate abuse alone.
Rationale for conditional effects
In addition to direct effects, we were also interested in examining possible conditional effects of socio-demographic factors that might moderate the relationship between maternal addiction and parenting. Conditional effects involving low SES, minority status and single parenthood have previously been identified across a wide range of parenting and child domains (see Luthar, 1999 for a review). Moreover, previous findings that children of substance-abusing minority mothers fare better than children of Caucasian mothers on externalizing behavior indices (Luthar et al., 1998) indicate that socio-demographic risk factors can confer vulnerability differently for clinical versus normal populations. In other words, factors that previously conferred advantage for “normal” populations of women may confer greater risk for addicted mothers, depending upon their implications for the women’s everyday lives. Based on previous findings that socio-demographic factors such as ethnicity, marital status (Weinraub & Gringlas, 1995) and family size (Luthar, 1999) confer vulnerability differently for mothers-at-risk versus comparison mothers, and given the prevalence of multiple socio-demographic stressors in addicted women’s lives (Mayes, 1995; Harden, 1998; Luthar & Suchman, 1999), we expected that socio-demographic factors would confer vulnerability differently for addicted mothers versus comparison mothers.
Theoretical framework and predictions
Ecological views of parenting (Bronfenbrenner, 1979) have recognized it as a series of interdependent processes (i.e. behavior management, relational quality, parental motivation) (Dishion & McMahon, 1998) that are influenced by psychological, demographic and cultural factors (Belsky, 1993; Lerner et al., 1995). This perspective lends itself readily to examining how dimensions of parenting might be differentially influenced by addiction, concomitant socio-demographic factors, and children’s behavior.
Based on previous work and ecological views of parenting, we expected that (a) maternal addiction would account for a significant proportion of the variance in problems of parental involvement, (b) low SES would account for a significant proportion of the variance in autonomy restriction and (c) perceptions of children’s maladaptive behavior would account for a significant proportion of the variance in limit setting problems. We also expected that minority status would serve as a protective factor whereas single parenthood and large family size would confer disadvantage for addicted mothers’ parenting.
Methods
Sample
Three objectives guided recruitment for this study. First, we sought to maintain relative homogeneity within the substance abuse dimension and therefore limited the sample of substance-abusing mothers to those enrolled in methadone treatment. This approach also allowed us to ensure that mothers were actively contending with drug abuse problems, manifested by their enrollment in treatment. Second, to ensure comparable SES with addicted mothers, we sought to oversample for low and middle SES among non-addicted mothers. Third, because parenting problems among drug-abusing mothers have been documented with both young children as well as older ones (Mayes, 1995; Harden, 1998; McMahon & Luthar, 1998) we sought diversity in terms of age and gender of the mothers’ children. To accomplish these objectives we recruited mothers with children under 16 years of age at three sites; mothers comprising the methadone sample were recruited from methadone clinics, and comparison mothers were recruited from a primary health care facility serving mostly lower SES women and from university administrative offices. Our sample consisted of 120 mothers, 69 methadone enrollees and 51 non-addicted comparison mothers. All mothers were asked to randomly select one “target” child less than 16 years of age to be the focus of her assessments.
Demographic characteristics for the total sample and for each group are presented in Table 1. The two groups were largely similar, with two exceptions: the methadone sample had more single and fewer minority mothers than the comparison sample. Most methadone mothers identified heroin and/or opiate use as their primary drug problem.
Table 1.
Socio-demographic characteristics, predictor and outcome measure means and standard deviations
| Comparison (n = 51) (percentages) | Addicted (n = 69) (percentages) | Total (n = 120) (percentages) | ||||
|---|---|---|---|---|---|---|
| Low SESa | 49.0 | 66.7 | 56.7 | |||
| Large familyb | 25.5 | 30.4 | 27.0 | |||
| Singlec | 49.0 | 78.3* | 62.0 | |||
| Minorityd | 66.7 | 33.3** | 47.0 | |||
| Target children | ||||||
| Male | 54.2 | 46.9 | 50.0 | |||
| Under 6 years | 12.5 | 18.8 | 16.0 | |||
| 6–11 years | 50.0 | 43.8 | 46.0 | |||
| 12–16 years | 37.5 | 37.5 | 37.6 | |||
| Primary drug problem | ||||||
| Heroin/opiates | – | 83.9 | – | |||
| Cocaine | – | 11.8 | – | |||
| Polydrug | – | 2.9 | – | |||
| Dual addiction | – | 1.4 | – | |||
| Mean | SD | Mean | SD | Mean | SD | |
|
| ||||||
| Mother’s age | 34.9 | 7.0 | 35.3 | 5.7 | 35.1 | 6.2 |
| Target children’s age | 10.0 | 3.9 | 9.6 | 4.6 | 9.8 | 4.3 |
| Childrene | 2.4 | 1.2 | 2.5 | 1.2 | 2.0 | 1.2 |
| Involvementf | 46.0 | 10.2 | 50.6 | 9.8 | 49.6 | 10.3 |
| Limit setting | 47.7 | 10.4 | 46.3 | 9.4 | 46.9 | 9.8 |
| Autonomy | 44.2 | 9.8 | 40.4 | 8.8 | 42.0 | 9.4 |
| Externalizing | 56.0 | 13.5 | 54.4 | 17.6 | 55.2 | 15.7 |
Corresponds to Hollingshead 2-Factor Class Levels IV and V,
More than three children in mother’s custody,
never married or separated/divorced,
African American or Hispanic origin,
number of children in mother’s custody,
italicized values represent T scores; values for Involvement represent the mean of the involvement and communication subscale T-Scores from the PCRI.
p < 0.10;
p < 0.05;
p < 0.01;
p < 0.001 (chi-square, t-tests).
Measures
Substance abuse
To ensure that the comparison group did not include women with substance abuse disorders, women recruited into the comparison group were assessed for substance abuse in two stages: first, we administered the Drug Use History subscale items from the Addiction Severity Index (ASI: McLellan et al., 1990). The 10 items on this subscale each pertain to a specific drug (e.g. alcohol, cocaine, heroin) and ask about the frequency, amount and duration (onset and offset) of substance use during the past 30 days as well as over the respondent’s life-time. For those women who reported any drug use since a child’s birth, we then determined whether they met the Structured Clinical Interview for DSM-III-R (Spitzer et al., 1988) diagnostic criteria for drug abuse and/or dependence during this period. A total of four mothers from the community sample met criteria for a substance abuse disorder since the birth of a child and were therefore excluded from the sample. The Drug Use History subscale from the ASI was also administered to mothers in the addicted sample in order to assess homogeneity of current drug problems.
Child maladjustment
Mothers’ reports of their children’s problematic behaviors were assessed with the Externalizing composite score from the Parent Rating Scale (PRS) of the Behavioral Assessment System for Children (BASC: Reynolds & Kamphaus, 1992). Separate PRS forms are available for different age groups of children: the Preschool (ages 4–5), Child (ages 6–11) and Adolescent (ages 12–18) versions, with 131, 138 and 126 items, respectively, all rated on four-point scales. In order to accommodate different PRS forms, raw scores were converted to T scores that were based on respective age- and gender-based normative samples (Reynolds & Kamphaus, 1992). Excellent psychometric properties for the BASC have been documented (Reynolds & Kamphaus, 1992). Within this sample, Cronbach’s alpha coefficients for the Externalizing composite across the three forms ranged between 0.73 and 0.93 with a median of 0.80.
Socio-demographic indicators
The Hollingshead Two-Factor Index of Social Position (Hollingshead & Redlich, 1958) was used to determine SES. Minority status (African-American and Hispanic ethnicity), marital status (never-married/divorced versus married/living with partner), and family size (“large” indicating more than three children in the mother’s custody) were determined via the demographic interview.
Parenting
The Parent–Child Relationship Inventory (PCRI: Gerard, 1994) is a 78-item self-report measure rated on a four-point scale that measures parents’ perceptions about their relationships with their children. Four of the seven PCRI subscales focus on parenting behaviors and were directly relevant to the objectives of this study; they included Communication (capacity to talk with and “get through” to children), Involvement (expressed interest in children’s activities), Limit Setting (ability to provide appropriate discipline) and Autonomy (ability to promote a child’s independence). Raw scores were converted to T scores based on a normative female sample (Gerard, 1994). With the exception of the Autonomy subscale, T scores below 40 represent problems of clinical significance. The Autonomy subscale is comprised of 10 items falling within two theoretical domains: the first reflects protective parental functions (i.e. “parents should be careful about whom they allow their children to have as friends”) and the second reflects emotional separation (i.e. “I miss the close relationship I had with my child when s/he was younger”). Thus, higher scores indicate more protective parenting strategies along with separation difficulties.
Reports of the PCRI’s psychometric characteristics (Gerard, 1994; Heinze & Grisso, 1996) have demonstrated adequate psychometric properties. Tests of internal consistency of all subscales have yielded Cronbach’s alphas above 0.70 with a median value of 0.82 (Gerard, 1994). Gerard and colleagues (1994) have also demonstrated good short-term (mean scale autocorrelation = 0.81) and long-term (mean scale autocorrelation = 0.55) temporal stability. The PCRI has demonstrated good predictive validity based on its moderate correlations with the Personality Inventory for Children (Wirt et al., 1990; Gerard, 1994) and with the Parental Acceptance—Rejection Questionnaire (Luthar & Suchman, 2000; Rohner, 1991). For this sample of mothers, Cronbach’s alpha coefficients for the four subscales were 0.81 for Involvement, 0.74 for Communication, 0.85 for Limit Setting and 0.67 for Autonomy. Further details on the PCRI’s psychometric properties are reported by Gerard (1994) and Heinze & Grisso (1996).
Procedure
Recruitment flyers were posted at each of the three sites. The flyers were addressed to mothers with children under 16 years of age, and included an invitation to participate in “a study about mothers and children” in exchange for a $20 payment. Mothers were directed to call the research assistant conducting the interviews. Participants were assessed in individual interviews lasting approximately 1.5 hours each, during which they answered questions pertaining to their demographic status and drug use history, and completed parenting and child maladjustment questionnaires.
Results
Data reduction and descriptive data
To minimize the likelihood of Type I errors, the Communication and Involvement subscales from the PCRI, which were empirically and conceptually related (r = 0.62), were summed to form a composite Parental Involvement index (Cronbach’s alpha = 0.88).
Means and standard deviations of all variables in the study are presented separately by group in Table 1. The two groups did not differ significantly on any of the child or parenting measures. Intercorrelations among variables (Table 2) were generally in expected directions. Children’s age was correlated with Involvement; children’s gender did not correlate with any of the parenting dimensions and was therefore excluded from subsequent analyses. Children’s externalizing behavior was correlated with Involvement and Limit Setting. Maternal addiction was correlated with Involvement and Autonomy. Low SES was correlated with Limit setting and Autonomy.
Table 2.
Simple correlations of variables
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | |
|---|---|---|---|---|---|---|---|---|---|---|
| 1. Child age | ||||||||||
| 2. Child gender | 0.14 | |||||||||
| 3. Children’s externalizing | 0.08 | 0.09 | ||||||||
| 4. Maternal addiction | −0.05 | 0.14 | 0.05 | |||||||
| 5. SES | 0.06 | 0.04 | 0.17 | 0.25** | ||||||
| 6. Minority status | 0.17 | 0.04 | 0.01 | −0.33** | 0.21* | |||||
| 7. Single parent | −0.01 | 0.07 | 0.10 | 0.31** | 0.20* | 0.09 | ||||
| 8. Family size | 0.17 | 0.00 | 0.16 | −0.14 | 0.12 | 0.12 | −0.19* | |||
| 9. Involvement | −0.30** | 0.02 | −0.27** | −0.23* | −0.16 | −0.01 | −0.04 | −0.12 | ||
| 10. Limit setting | −0.01 | 0.09 | −0.66** | −0.06 | −0.21* | −0.00 | −0.02 | −0.17 | 0.36** | |
| 11. Autonomy | 0.09 | −0.05 | −0.17 | −0.20* | −0.36** | −0.13 | 0.04 | 0.03 | 0.03 | 0.31** |
p < 0.05;
p < 0.001
Hierarchical regression analyses
In a series of hierarchical regressions conducted to test direct and conditional effects, children’s age (block 1) was entered first as a covariate, followed by externalizing behavior (block 2), socio-demographic factors (block 3), opiate addiction (block 4) and socio-demographic × addiction interaction terms (block 5). The entry order of socio-demographic factors in block 3 and interaction terms in block 5 was allowed to vary in order of decreasing tolerance (Tabachnick & Fidell, 1996) and variance change accounted for by each factor and interaction term was calculated based on semipartial correlations. Due to the small sample size, effect sizes (η2) were also computed to confirm strength of associations (Aiken & West, 1991). Based on criteria that included a conditioning index of less than 30 and at least two variance proportions above 0.50 for root numbers (Tabachnick & Fidell, 1996), multi-collinearity within the full model was ruled out.
Direct effects
As predicted (Table 3), after children’s age was taken into account, mothers’ views of their children’s externalizing behavior predicted significant variance in limit setting (R2 = 0.44; p < 0.001) with beta values indicating that greater externalizing problems were associated with higher severity of limit-setting problems. With age and children’s behaviors taken into account, SES predicted significant variance in Autonomy (R2 = 0.16; p < 0.001) with beta values indicating an association between lower SES and lower autonomy. After age, children’s behaviors and SES were entered into the model, maternal addiction explained unique variance in Involvement (R2 = 0.08; p < 0.01) and was also marginally linked with Autonomy (R2 = 0.03; p < 0.05), with beta values indicating associations between maternal addiction and declines in both parenting domains. Because we had predicted that only SES would be linked with Autonomy, we conducted three simple regressions (Baron & Kenny, 1986) to examine its role as a mediator in the maternal addiction—Autonomy link. After first establishing that opiate addiction predicted significant variance in SES (R2 = 0.06; p < 0.01) and in autonomy (R2 = 0.03; p < 0.10), we regressed autonomy on maternal addiction after accounting for SES variance. Results showed that addiction explained less unique variance in the latter model (R2 = 0.01; p= 0.33), confirming the mediating role of SES.
Table 3.
Hierarchical regression testing children’s externalizing behavior, socio-demographic (SD), maternal addiction (MA) and SD × MA interaction effects in relation to parenting
| Involvement
|
Limit setting
|
Autonomy
|
||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Criterion: | Step | β | R2Δ | η2 | β | R2Δ | η2 | β | R2Δ | η2 |
| Child’s age | 1 | −0.83 | 0.13*** | 0.13*** | 0.13 | 0.01 | 0.00 | −0.06 | 0.00 | 0.00 |
| Child’s externalizing | 2 | −0.12 | 0.05* | 0.06* | −0.27 | 0.44*** | 0.44*** | −0.04 | 0.02 | 0.02 |
| Socio-demographic factors | 3 | 0.64 | 0.01 | – | 0.86 | 0.02 | – | – | 0.18*** | – |
| SES | – | – | – | – | – | – | −0.11 | 0.16*** | 0.16*** | |
| Minority | – | – | – | – | – | – | −0.86 | 0.01 | 0.01 | |
| Single | – | – | – | – | – | – | 1.37 | 0.02 | 0.03 | |
| Family size | – | – | – | – | – | – | 0.13 | 0.00 | 0.00 | |
| Maternal addiction (MA) | 4 | −5.46 | 0.08** | 0.09** | −1.14 | 0.01 | 0.01 | −1.78 | 0.03* | 0.04** |
| Interaction effects | 5 | −10.46 | 0.10** | – | −0.79 | 0.01 | – | – | 0.15*** | – |
| MA × SES | −0.14 | 0.01 | 0.02 | – | – | – | 0.07 | 0.01 | 0.02 | |
| MA × minority | 2.56 | 0.01 | 0.00 | – | – | – | −2.97 | 0.01 | 0.01 | |
| MA × single | −10.46 | 0.07** | 0.11** | – | – | – | 5.07 | 0.06** | 0.06* | |
| MA × family size | 0.28 | 0.01 | 0.00 | – | – | – | 2.05 | 0.09** | 0.11** | |
| Total R2 | 0.27 | 0.49 | 0.37 | |||||||
p < 0.10;
p < 0.05;
p < 0.01;
p < 0.001.
Conditional effects
The interaction block (block 5) explained unique variance in Involvement (R2 = 0.10; p < 0.01) and Autonomy (R2 = 0.15; p < 0.001). Examination of semi-partial correlations within each significant interaction block indicated that the Addiction × Single parent interaction explained significant variance in Involvement (R2 = 0.08; p < 0.01) and Autonomy (R2 = 0.06; p < 0.01) and the Addiction × Family Size interaction explained significant variance in Autonomy (R2 = 0.09; p < 0.01). Interaction patterns (Fig. 1–3) indicated that (a) being single conferred disadvantage for addicted mothers’ involvement (Fig. 1), and (b) cohabitation (Fig. 2) and having a small family (Fig. 3) were associated with lower levels of fostered autonomy among addicted women.
Figures 1–3.
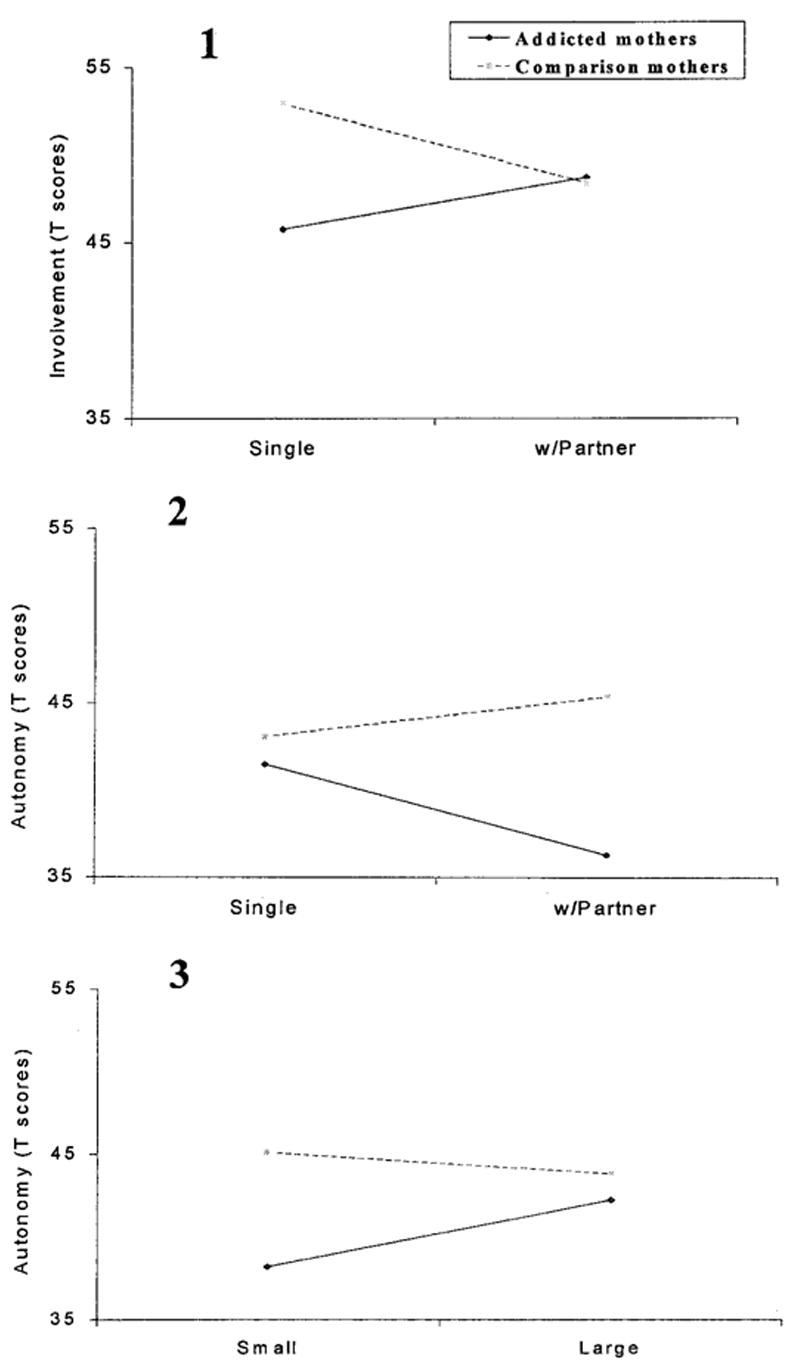
Socio-demographic × maternal addiction interaction effects.
Discussion
Although a multitude of parenting problems have previously been associated with maternal substance abuse, our results indicated that SES and mothers’ perceptions of their children’s maladaptive behavior may also play a significant role in opiate-addicted mothers’ parenting. Furthermore, socio-demographic factors (single marital status and family size) can significantly moderate the relationship between addiction and parenting. Before turning to the larger implications of these results, we discuss each finding in turn.
Direct effects
The link between maternal addiction and parental involvement is consistent with the previously demonstrated lack of involvement and initiative that characterize the parenting styles and behaviors of addicted parents. It also reflects what ethnographers have described as ambivalence among many heroin-addicted mothers about having and raising children (Rosenbaum, 1981; Taylor, 1993; Kearney, Harphy & Rosenbaum, 1994), and subsequent efforts to “farm out” children to neighbors and relatives to protect them from a disruptive, drug-using life-style (Kearney et al., 1994; Feig, 1998; Harden, 1998; Resnik, Gardner & Rogers, 1998). The association between maternal addiction and parental involvement also concurs with reported outcomes of parent training for methadone-maintained parents, showing that parental involvement is particularly refractory to change (Catalano et al., 1999). From a treatment perspective, these findings imply a need for concerted attention to mothers’ positive involvement with their children (see Luthar & Suchman, 2000), in addition to the dimensions of behavioral management that are more typically addressed (e.g. anger management and appropriate disciplinary techniques) in parent training.
The link between low SES and restricted autonomy may be an adaptive response to living in environments where children’s exposure to violence, crime, drug addiction and health hazards is high (Luthar, 1999). Consistent and strong monitoring have proven to be more effective in reducing the likelihood of maladaptive behaviors among children living in low-income, potentially dangerous environments (Baldwin, Baldwin & Cole, 1990; McLoyd, 1990; Haapasalo & Tremblay, 1994; Jarrett, 1995; Luster & McAdoo, 1996; Apfel & Seitz, 1997; Simon & Burns, 1997).
Conditional effects
The conditional effects indicated that being single and having a large family conferred differential vulnerability for addicted versus comparison mothers. Specifically, being single conferred greater vulnerability for addicted mothers’ involvement whereas cohabitation and smaller family size conferred greater risk for restricted autonomy. For addicted mothers, cohabitation with partners and having fewer children may lead to more protective and enmeshed parenting styles. Overall, the nature of the conditional effects suggests that socio-demographic configurations of families affected by maternal drug addiction may confer vulnerability in unique ways that warrant further examinations.
Limitations and future directions
Several shortcomings limit the generalization of findings and can help to guide future research. The overall sample size was small. Most mothers in the addicted sample were Caucasian and seeking treatment for heroin and/or opiate use. Future studies involving larger samples of mothers with a wider range of active drug problems would help differentiate parenting dimensions associated with different drug disorders.
Mothers’ co-morbid psychopathology was not assessed. Recent findings that co-morbid psychopathology among addicted women is both directly (Beckwith et al., 1999) and indirectly (Hans, Bernstein & Henson, 1999) associated with their parenting indicate the importance of testing maternal psychopathology in contextual models in the future.
Although the accuracy of maternal reports was not cross-validated, there was no evidence of marked underreporting of parenting problems by addicted mothers. The validity of self-report data collected from substance-abusing mothers has often been considered dubious due to widely held expectations that they will deny parenting problems (Mayes, 1995). In this study, in addition to conducting replicatory analyses with control for social desirability, we examined the frequency with which clinically significant parenting problems were reported by addicted versus non-addicted mothers and found that addicted mothers reported significantly more problems than comparison mothers in two of the three parenting dimensions1.
The cross-sectional design precludes causal interpretations. Although their cost-effectiveness has been questioned, prospective studies that track the onset of substance abuse disorders, co-morbid psychiatric disorders, children’s mal-adjustment and socio-demographic indices might help identify causal factors and processes related to poor parenting and child outcomes.
Limitations notwithstanding, this study yielded several substantive insights regarding maternal drug abuse and dimensions of parenting. In instances of maternal drug addiction, the mothers’ substance abuse has typically been viewed as the primary if not sole “cause” of serious, across-the-board parenting deficits. Our findings show that socio-demographic risks and children’s maladaptive behavior can contribute at least as much, if not more, than maternal addiction, per se, to parenting problems. Furthermore, whereas addicted women certainly experience grave difficulties in some parenting domains, they are not necessarily seriously impaired in all aspects of how they relate to their children. In future research, there is a pressing need for more studies which concurrently examine contextual factors (including poverty, transience, vocational instability) along with psychosocial variables (including mothers’ relational stability, trauma exposure, loss and children’s maladjustment) that can conjointly influence the effectiveness of addicted mothers’ behaviors across different parenting domains.
Acknowledgments
Preparation of this manuscript was supported by R01-DA11498. We gratefully acknowledge Bruce Rounsaville for his ongoing mentorship and thoughtful comments on earlier drafts of this manuscript. Thanks are also due to Thomas McMahon and Linda Mayes for their contributions to the design of this work, and to Kimberly Doyle, Lara Shugar, Michelle Altomare, and members of the Child and Family Research Group at the Yale Substance Abuse Center for their assistance with data collection and manuscript preparation.
Footnotes
Chi-square analyses indicated the following values: Involvement (F = 4.0, p < 0.01); Autonomy (F = 2.5, p < 0.05); Limit Setting (F = 0.02, p = 0.87).
References
- Aiken LS, West SG. Multiple Regression: testing and interpreting interactions. Thousand Oaks, CA: Sage; 1991. [Google Scholar]
- Apfel N, Seitz V. The firstborn sons of African-American teenage mothers: perspectives on risk and resilience. In: Luthar SS, Burack JA, Cicchetti D, Weisz JR, editors. Developmental Psychopathology: perspectives on adjustment, risk, and disorder. New York: Cambridge University Press; 1997. pp. 486–506. [Google Scholar]
- Baldwin AL, Baldwin C, Cole RE. Stress-resistant families and stress-resistant children. In: Rolf J, Masten AS, Cicchetti D, Nuechterlein KH, Weintraub S, editors. Risk and Protective Factors in the Development of Psychopathology. New York: Cambridge University Press; 1990. pp. 257–280. [Google Scholar]
- Baron RM, Kenny DA. The moderator–mediator variable distinction in social psychological research: conceptual, strategic, and statistical considerations. Journal of Personality and Social Psychology. 1986;51:1173–1182. doi: 10.1037//0022-3514.51.6.1173. [DOI] [PubMed] [Google Scholar]
- Bauman PS, Dougherty FE. Drug-addicated mothers’ parenting and their children’s development. International Journal of the Addictions. 1983;18:291–302. doi: 10.3109/10826088309039348. [DOI] [PubMed] [Google Scholar]
- Baumrind D. Current patterns of parental authority. Developmental Psychology Monograph. 1971;4:1–102. [Google Scholar]
- Beckwith L, Howard J, Espinosa M, Tyler R. Psychopathology, mother–child interaction, and infant development: substance-abusing mothers and their offspring. Development and Psychopathology. 1999;11:715–725. doi: 10.1017/s095457949900228x. [DOI] [PubMed] [Google Scholar]
- Belsky J. Etiology of child maltreatment: a developmental–ecological analysis. Psychological Bulletin. 1993;114:413–434. doi: 10.1037/0033-2909.114.3.413. [DOI] [PubMed] [Google Scholar]
- Bernstein V, Jeremy RJ, Hans SL, Marcus J. A longitudinal study of offspring born to methadone-maintained women: II. Dyadic interaction and infant behavior at four months. American Journal of Drug and Alcohol Abuse. 1984;10:161–193. doi: 10.3109/00952998409002779. [DOI] [PubMed] [Google Scholar]
- Besinger BA, Garland AF, Litrownik AJ, Landsverk JA. Caregiver substance abuse among maltreated children placed in out-of-home care. Child Welfare. 1999;LXXVIII:221–239. [PubMed] [Google Scholar]
- Bronfenbrenner U. The Ecology of Human Development. Cambridge, MA: Harvard University Press; 1979. [Google Scholar]
- Catalano RF, Gainey RR, Fleming CB, Haggerty KP, Johnson NO. An experimental intervention with families of substance abusers: one-year follow-up of the focus on families project. Addiction. 1999;94:241–254. doi: 10.1046/j.1360-0443.1999.9422418.x. [DOI] [PubMed] [Google Scholar]
- Chaffin M, Kelleher K, Hollenberg J. Onset of physical abuse and neglect: psychiatric, substance abuse, and social risk factors from prospective community data. Child Abuse and Neglect. 1996;20:191–203. doi: 10.1016/s0145-2134(95)00144-1. [DOI] [PubMed] [Google Scholar]
- Cummings EM, Davies PT. Maternal depression and child development. Journal of Child Psychology and Psychiatry and Allied Disciplines. 1994;35:73–112. doi: 10.1111/j.1469-7610.1994.tb01133.x. [DOI] [PubMed] [Google Scholar]
- Davis S. Chemical dependency in women: a description of its effects and outcome on adequate parenting. Journal of Substance Abuse Treatment. 1990;7:225–232. doi: 10.1016/0740-5472(90)90045-r. [DOI] [PubMed] [Google Scholar]
- Deren S. Children of substance abusers: a review of the literature. Journal of Substance Abuse Treatment. 1986;3:77–94. doi: 10.1016/0740-5472(86)90056-5. [DOI] [PubMed] [Google Scholar]
- Dishion TJ, Mcmahon RJ. Parental monitoring and the prevention of child and adolescent problem behavior: a conceptual and empirical formulation. Clinical Child and Family Psychology Review. 1998;1:61–75. doi: 10.1023/a:1021800432380. [DOI] [PubMed] [Google Scholar]
- Egami Y, Ford DE, Greenfield SF, Crum RM. Psychiatric pro le of sociodemographic characteristics of adults who report physically abusing or neglecting children. American Journal of Psychiatry. 1996;153:921–928. doi: 10.1176/ajp.153.7.921. [DOI] [PubMed] [Google Scholar]
- Eisenberg N, Fabes RA, Shepard SA, Guthrie IK, Murphy BC, Reiser M. Parental reactions to children’s negative emotions: longitudinal relations to quality of children’s social functioning. Child Development. 1999;70:513–534. doi: 10.1111/1467-8624.00037. [DOI] [PubMed] [Google Scholar]
- Feig L. Understanding the problem: the gap between substance abuse programs and child welfare services. In: Hamption RL, Senatore V, Gullotta TP, editors. Substance Abuse, Family Violence, and Child Welfare: Bridging perspectives: Vol. 10. Issues in children’s and families’ lives. Thousand Oaks, CA: Sage; 1998. pp. 62–95. [Google Scholar]
- Ge X, Conger RD, Lorenz FO, Shanahan M, Elder GH. Mutual influences in parent and adolescent psychological distress. Developmental Psychology. 1995;31:406–419. [Google Scholar]
- Gerard AB. Parent–Child Relationship Inventory (PCRI)Manual. Los Angeles, CA: Western Psychological Services; 1994. [Google Scholar]
- Haapasalo J, Tremblay RE. Physically aggressive boys from ages 6 to 12: family background, parenting behavior and prediction of delinquency. Journal of Consulting and Clinical Psychology. 1994;62:104–105. doi: 10.1037//0022-006x.62.5.1044. [DOI] [PubMed] [Google Scholar]
- Hampton RL, Senatore V, Gullotta TP, editors. Issues in Children’s and families’ lives. Vol. 10. Thousand Oaks, CA: Sage; 1998. Substance Abuse, Family Violence, and Child Welfare: bridging perspectives. [Google Scholar]
- Hans SL. Maternal opioid use and child development. In: Zagon IS, Slotkin TA, editors. Maternal Substance Abuse and the Developing Nervous System. Boston: Academic Press; 1992. pp. 177–214. [Google Scholar]
- Hans SL, Bernstein VJ, Henson LG. The role of psychopathology in the parenting of drug-dependent women. Development and Psychopathology. 1999;11:957–977. doi: 10.1017/s0954579499002400. [DOI] [PubMed] [Google Scholar]
- Harden BJ. Building bridges for children: addressing the consequences of exposure to drugs and to the child welfare system. In: Hampton RL, Senatore V, Gullotta TP, editors. Substance Abuse, Family Violence, and Child Welfare: bridging perspectives. Vol. 10. Thousand Oaks, CA: Sage; 1998. pp. 18–61. Issues in children’s and families’ lives. [Google Scholar]
- Heinze MC, Grisso T. Review of instruments assessing parenting competencies used in child custody evaluations. Behavioral Sciences and the Law. 1996;14:293–313. [Google Scholar]
- Hoff-Ginsberg E, Tardif T. Socioeconomic status and parenting. In: Bornstein M, editor. Handbook of Parenting: Vol. 2 Biology and ecology of parenting. Mahwah, NJ: Lawrence Erlbaum; 1995. pp. 161–188. [Google Scholar]
- Hollingshead AB, Redlich FC. Social Class and Mental Illness. New York: Wiley; 1958. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jarrett RL. Growing up poor: the family experiences of socially mobile youth in low-income African-American neighborhoods. Journal of Adolescent Research. 1995;10:111–135. [Google Scholar]
- Kearney MH, Murphy S, Rosenbaum M. Mothering on crack cocaine: a grounded theory analysis. Social Science and Medicine. 1994;38:351–361. doi: 10.1016/0277-9536(94)90405-7. [DOI] [PubMed] [Google Scholar]
- Kelleher K, Chaffin M, Hollenberg J, Fischer E. Alcohol and drug disorders among physically abusive and neglectful parents in a community-based sample. American Journal of Public Health. 1994;84:1586–1590. doi: 10.2105/ajph.84.10.1586. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lerner RM, Castellino DR, Terry PA, Villarruel FA, McKinney MH. Developmental contextual perspective on parenting. In: Bornstein MH, editor. Handbook of Parenting. Vol. 4. Mahway, NJ: Lawrence Erlbaum Associates; 1995. pp. 285–309. Applied and practical parenting. [Google Scholar]
- Luster T, McAdoo HP. Family and child influences on educational attainment: a secondary analysis of the High/Scope Perry Preschool data. Developmental Psychology. 1996;32:26–39. [Google Scholar]
- Luthar SS. Poverty and Children’s Adjustment: developmental clinical psychology and psychiatry. Vol. 41. Thousand Oaks, CA: Sage; 1999. [Google Scholar]
- Luthar SS, Cushing G, Merikangas K, Rounsaville BJ. Multiple jeopardy: risk/protective factors among addicted mothers’ offspring. Development and Psychopathology. 1998;10:117–136. doi: 10.1017/s0954579498001333. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Luthar SS, Suchman NE. Developmentally informed parenting interventions: the Relational Psychotherapy Mothers’ Group. In: Cicchetti D, Toth SL, editors. Rochester Symposium on Developmental Psychopathology. Vol. 9. Rochester, NY: University of Rochester Press; 1999. pp. 271–309. Developmental approaches to prevention and intervention. [Google Scholar]
- Luthar SS, Suchman NE. Relational Psychotherapy Mothers’ Group: a developmentally informed intervention for at-risk mothers. Development and Psychopathology. 2000;12:235–253. doi: 10.1017/s0954579400002078. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mayes L. Substance abuse and parenting. In: Bornstein M, editor. Handbook of Parenting. Applied and practical parenting. Vol. 4. Mahwah, NJ: Lawrence Erlbaum; 1995. pp. 101–125. [Google Scholar]
- McLellan AT, Gargi P, Bragg A, Cacciola J, Fureman B, Incmikoski R. Addiction Severity Index: administration manual. Philadelphia: University of Pennsylvania—Veterans Administration Center for Studies of Addiction; 1990. [Google Scholar]
- McLoyd VC. The impact of economic hardship on black families and children: psychological distress, parenting, and socioemotional development. Child Development. 1990;61:311–346. doi: 10.1111/j.1467-8624.1990.tb02781.x. [DOI] [PubMed] [Google Scholar]
- McMahon TJ, Luthar SS. Bridging the gap for children as their parents enter substance abuse treatment. In: Hampton RL, Senatore V, Gullotta TP, editors. Substance Abuse, Family Violence, and Child Welfare: bridging perspectives. Vol. 10. Thousand Oaks, CA: Sage; 1998. pp. 143–187. Issues in children’s and families’ lives. [Google Scholar]
- Murphy JM, Jellinek M, Quinn D, Smith G, Poitrast FG, Goshko M. Substance abuse and serious child mistreatment: prevalence, risk, and outcome in a court sample. Child Abuse and Neglect. 1991;15:197–211. doi: 10.1016/0145-2134(91)90065-l. [DOI] [PubMed] [Google Scholar]
- The National Center on Addiction and Substance Abuse (NCASA) Substance Abuse and the American Woman. New York: NCASA; 1996. [Google Scholar]
- Peterson L, Ewigman B, Vandiver T. Role of parental anger in low-income women: discipline strategy, perceptions of behavior problems, and the need for control. Journal of Clinical Child Psychology. 1994;23:435–443. [Google Scholar]
- Resnik H, Gardner SE, Rogers CM. Child welfare and substance abuse: premises, programs and policies. In: Hampton RL, Senatore V, Gullotta TP, editors. Substance Abuse, Family Violence, and Child Welfare: bridging perspectives. Vol. 10. Thousand Oaks, CA: Sage; 1998. pp. 96–123. Issues in children’s and families’ lives. [Google Scholar]
- Reynolds CR, Kamphaus RW. Behavioral Assessment System for Children (BASC) Circle Pines, MN: American Guidance Service; 1992. [Google Scholar]
- Rohner RP. Handbook for the Study of Parental Acceptance and Rejection. Storrs, CT: University of Connecticut; 1991. [Google Scholar]
- Rosenbaum M. Women on Heroin. New Brunswick, NJ: Rutgers University Press; 1981. [Google Scholar]
- Sedlak AJ, Broadhurst DD. Executive Summary of the Third National Incidence Study of Child Abuse and Neglect. Washington, DC: US Department of Health and Social Services; 1996. [Google Scholar]
- Simon D, Burns E. The Corner: a year in the life of an inner-city neighborhood. New York: Broadway Books; 1997. [Google Scholar]
- Spitzer RL, Williams JB, Gibbon M, First MB. Instruction Manual for the Structured Clinical Interview for DSM-III-R: SCID. New York: Biometrics Research; 1988. [Google Scholar]
- Stice E, Barrera M. A longitudinal examination of the reciprocal relations between perceived parenting and adolescents’ substance use and externalizing behaviors. Developmental Psychology. 1995;31:322–334. [Google Scholar]
- Tabachnick BG, Fidell LS. Using Multivariate Statistics. 3. New York: Harper Collins; 1996. [Google Scholar]
- Taylor A. Women Drug Users: an ethnography of a female injecting community. Oxford: Clarendon Press; 1993. [Google Scholar]
- Weinraub M, Gringlas MB. Single parenthood. In: Bornstein M, editor. Handbook of Parenting. Vol. 3. Mahwah, NJ: Lawrence Erlbaum; 1995. pp. 65–87. Status and social conditions of parenting. [Google Scholar]
- Wirt R, Lachar D, Klinedinst J, Seat P, Broen W. Multidimensional Description of Child Personality: a manual for the personality inventory for children. Los Angeles: Western Psychological Services; 1990. [Google Scholar]