

Abstract
Background
As the number of older drivers increases, concern has been raised about the potential safety implications. Flexibility, coordination, and speed of movement have been associated with older drivers’ on road performance.
Objective
To determine whether a multicomponent physical conditioning program targeted to axial and extremity flexibility, coordination, and speed of movement could improve driving performance among older drivers.
Design
Randomized controlled trial with blinded assignment and end point assessment. Participants randomized to intervention underwent graduated exercises; controls received home, environment safety modules.
Participants
Drivers, 178, age ≥ 70 years with physical, but without substantial visual (acuity 20/40 or better) or cognitive (Mini Mental State Examination score ≥24) impairments were recruited from clinics and community sources.
Measurements
On-road driving performance assessed by experienced evaluators in dual-brake equipped vehicle in urban, residential, and highway traffic. Performance rated three ways: (1) 36-item scale evaluating driving maneuvers and traffic situations; (2) evaluator’s overall rating; and (3) critical errors committed. Driving performance reassessed at 3 months by evaluator blinded to treatment group.
Results
Least squares mean change in road test scores at 3 months compared to baseline was 2.43 points higher in intervention than control participants (P = .03). Intervention drivers committed 37% fewer critical errors (P = .08); there were no significant differences in evaluator’s overall ratings (P = .29). No injuries were reported, and complaints of pain were rare.
Conclusions
This safe, well-tolerated intervention maintained driving performance, while controls declined during the study period. Having interventions that can maintain or enhance driving performance may allow clinician–patient discussions about driving to adopt a more positive tone, rather than focusing on driving limitation or cessation.
KEY WORDS: driving performance, randomized trial, physical conditioning program
Maintaining the safety of older drivers is a concern, given the increasing number of older persons and their heightened susceptibility to crash injury. In 1990, individuals age 65 years and older constituted approximately 13% of licensed drivers (22 million) in the United States, with an expected 50% increase by 2020.1,2 Motor vehicle crashes are the leading cause of injurious and fatal “accidents” among individuals age 65 to 74 years, and the second leading cause among those age 75 years and older, with two- to fourfold increases in rates of injury, hospitalization, and death among individuals 65 years and older compared to younger individuals in crashes of similar magnitude.3–6
Increasing evidence supports the importance of driving for independence and well-being in some countries. Older persons depend on cars for transportation as driver or passenger.7,8 Participation in social and productive activities has been associated with survival and better functional status.9–13 Conversely, driving cessation has been linked to decreased participation in out-of-home activities and increased depressive symptoms.14–16
There is a need to identify individuals at increased risk for crashes or poor driving performance and to determine if driving performance can be enhanced and crash risk lowered, thereby, maximizing and prolonging safe driving by older persons. Previous studies indicated that functional impairments (vision, cognition, and physical ability), medical conditions, and medications, rather than age alone, contribute to crash risk and poor driving performance.17–34
Based on our previous work, the current study utilized a randomized control design to determine whether a multicomponent physical conditioning program targeted to physical abilities relevant to driving safety (axial and extremity flexibility, coordination, and speed of movement) could enhance driving performance.33,34 While physical ability is only one of several contributing factors to driving safety, improving driving performance by enhancing physical ability would be an initial step toward extending the safe mobility of older persons, thereby, maintaining their independence and social functioning.
METHODS
Participant Recruitment
Participants in the greater New Haven area were recruited from the waiting rooms of the general medicine clinics at VA Connecticut Healthcare System [VACHS (62% of participants)], general medicine and geriatrics clinics at a local hospital (3%), and from several community sites including two senior housing complexes (9%), a senior center (1%), a health fair (1%), volunteer groups (6%), and the enrollment list of a former health maintenance organization [HMO (19%)]. At clinic sites, participants were recruited and screened on-site. At community sites, participants were recruited through on-site presentations or by mail/phone contacts (HMO enrollees); screening took place in their homes.
Study inclusion criteria were: age ≥70 years, driving at least once per week, valid driver’s license, English speaking, having a phone, absence of medical conditions that might deteriorate during the study (e.g., dementia and other neurodegenerative disorders, metastatic cancer) or acute medical illness at time of screening, binocular near visual acuity of 20/40 or better, Mini-Mental State Examination score ≥24, and presence of two or more physical impairments described below.34,35
Screening
A screening method was developed to identify drivers at increased risk for safety difficulties based on the presence of physical impairments; drivers with substantial visual or cognitive impairment were excluded. The screening method was derived from our earlier work demonstrating a high correlation (r = .73) between the number of physical impairments and on-road driving performance. These impairments (utilizing cut points established in earlier studies) included: inability to turn one’s head to touch shoulders (neck rotation), turn one’s trunk to touch the wall behind shoulders (trunk rotation), lift shoulders to touch hands behind one’s head (shoulder abduction), clear a 4-in. card placed beneath the foot (hip flexion); >18.5 seconds to place 5 small objects in a cup using tweezers (manual dexterity); and >11 seconds to walk 10 ft and back as quickly as possible (gait speed).34 To identify participants who had physical impairments and lower driving performance scores and therefore might benefit from the intervention, a linear regression model identified drivers with 2 or more physical impairments as having a predicted total driving score of 59 (72 point scale) with an upper 95% confidence limit of 67.
Assessment of Driving Performance
Eligible participants completed an on-road driving evaluation. A route through New Haven and West Haven, Connecticut included a mix of off-road settings (parking lot maneuvers); low, medium, and high traffic density areas; and highway segments, with two entry points depending on recruitment site.
Driving assessments were conducted by 1 of 2 driving evaluators [specially trained occupational therapist, former Connecticut Department of Motor Vehicles (CT DMV) assessor] blinded to treatment assignment. Assessments occurred at the same time of day (mornings), on the same route, and in the same dual brake-equipped vehicle. Assessments lasted approximately 45 minutes and were conducted in daylight under favorable weather conditions. Evaluations were rescheduled in the event of ice, snow, or thunderstorms that might adversely affect safety or driving performance.
Driving performance was rated on a 36-item scale that evaluated a number of driving maneuvers and traffic situations based on the driving evaluation form utilized by the CT DMV.36 Scoring criteria were developed beforehand. Each item was scored 0 for major problem, 1 for minor problem, and 2 for no problem, and then summed to give a total score ranging from 0 (worst) to 72 (best). Secondary driving performance measures were the driving evaluator’s rating and number of critical errors committed. The driving evaluator gave an overall rating of driving performance based on a 4-point scale (1 for no problem, 2 for minor, 3 for moderate, 4 for major). Critical errors, enumerated before the study by the driving therapist, observed during the evaluation (range 0–3) included inattention, turning or changing lanes without looking, and disobeying signs or signals.
Inter-rater reliability established on 89 drivers in this intervention cohort with two driving evaluators providing independent ratings demonstrated an intra-class correlation coefficient of 0.98 for the total road test score. Weighted kappas for each of 36 scale items ranged from 0.66 to 1.0, with mean = 0.92 (SD = 0.08) and median = 0.94.
Randomization
Randomization was stratified by recruitment site using a permutated block scheme with a block size of four and equal allocation. The sequence was concealed until interventions were assigned. Participants not completing the baseline assessment or failing the driving evaluation (deemed unsafe by the evaluator) were excluded from the study before randomization. Drivers were determined to be unsafe if the evaluator had to repeatedly take control of the vehicle or if the road test needed to be aborted because of potentially life-threatening errors and driver unawareness of the errors or their severity. A similar exclusion criterion was added early in the study for drivers performing too well on the baseline road test (scoring 71 or 72) as it would not be possible to detect an improvement with intervention. Before this exclusion criterion, two participants with scores of 71 and 72 were randomized to the intervention group and included in the analyses.
Intervention
Participants randomized to the intervention group received weekly visits for 12 weeks by a physical therapist who guided them through a graduated exercise program directed at physical abilities potentially relevant to driving based on earlier studies. The intervention protocol targeted the following physical domains and abilities: axial/extremity conditioning (cervical, trunk and axial rotation; cervical flexion and extension, shoulder flexion and abduction, hip flexion and abduction, knee flexion and extension, ankle dorsiflexion and plantarflexion); upper extremity coordination/dexterity and hand strength; gait and foot abnormalities. Consulting academic and practicing occupational and physical therapists, an orthopedic surgeon, and a rheumatologist reviewed the intervention protocol for completeness and safety. Two experienced physical therapists administered the intervention protocol; both underwent intensive initial training to familiarize themselves with protocol content and quarterly quality control sessions to review protocol elements and address any questions or concerns.
Each of the conditioning and coordination domains consisted of three progressive levels of exercises. A manual with pictorial and written instructions, and relevance of each exercise to driving, was provided to participants and reviewed with them by the therapist at weekly visits. The therapist gradually increased the number of repetitions for each exercise once the participant demonstrated the ability to perform the exercises safely and correctly. Exercise programs were designed to take 15 minutes; participants were asked to perform the exercises once daily, 7 days a week. Gait abnormalities were identified and recommendations made to correct unsafe or inefficient gait patterns and encourage walking for exercise. Participants with foot problems were referred to podiatry, and suggestions for safe footwear were made by the therapist.
A safety protocol was developed with therapists actively instructing and monitoring correct performance of the exercises and inquiring about pain or injury on each weekly visit. Conditions requiring precautions or contraindicating an exercise were identified before the study and reviewed at therapist visits. Adherence was monitored with monthly calendars completed by participants.
Control Group
The control group received monthly in-home education modules reviewing general safety issues about home safety, fall prevention, and vehicle care, presented by trained research assistants. Materials were written at an eighth-grade level and illustrated with simple line drawings. Intervention group participants also received these modules to ensure that the materials did not influence study outcomes.
Outcomes
The primary outcome was change in on-road driving performance at 3 months relative to baseline. To improve the clinical interpretability of driving performance scores, participants were also classified into terciles of driving performance based on baseline road test scores: high ( ≥ 63), middle (58 to 62), and low ( ≤ 57). Secondary outcomes were the driving evaluator’s overall rating and number of critical errors at 3 months, as defined above.
Sample Size
Based on a pilot test and discussion with the driving evaluator a priori, a clinically meaningful difference in the primary outcome was defined as a change of two points. The sample size to detect this difference between intervention and control groups was 150 participants for 80% power, 30% adjustment for losses, and road test standard deviation of 13.6 points (pilot data).
Informed Consent
The study was approved by the School of Medicine’s Human Investigation Committee and the VACHS Human Subjects Subcommittee. Written informed consent was obtained for all participants.
Analysis
The primary outcome was analyzed according to original treatment assignment by randomization. Four participants in the intervention group without a follow-up road test were excluded from the analysis. Multiple linear regression was used to analyze treatment efficacy, adjusted for recruitment site (clinic or nonclinic), driving evaluator and baseline driving tercile. Treatment effects were summarized as least square means (± 1 standard error) overall and by tercile. Treatment differences were tested by the t-statistic. Analyses were repeated utilizing imputed values for the four drivers without follow-up road tests, which did not appreciably change the findings (data not presented).
The effect of treatment on the two discrete secondary outcomes was analyzed similar to the primary outcome according to the original treatment assignment. A Poisson regression model was used to analyze the effect of treatment on the number of critical errors, and an ordinal logistic regression model was used for the evaluator rating.37 Models were adjusted for recruitment site (clinic or nonclinic), driving evaluator, and baseline values of each secondary outcome. Treatment effects were summarized as odds ratios and corresponding 95% confidence intervals. Differences in safety measures (incident falls) between the two treatment groups were tested by the chi-square statistic.
SAS version 8.1 (SAS Institute, Cary, NC) was used for all analyses, and a value of 0.05 (2-sided) was used for all tests of significance.
RESULTS
Participant Characteristics
A total of 744 drivers age 70 years and older were screened from May 1998 to June 2000 (Fig. 1). Of these, 485 (65%) were ineligible, primarily because of not meeting physical, visual, or cognitive criteria for participation (435% or 90% of those ineligible). Sixty-six (25%) of the 259 eligible subjects refused to participate, mainly because they did not want to drive someone else’s car or drive in New Haven, or because their family recommended against participation. An additional 15 (6%) were excluded before randomization because they either failed or scored too high on the baseline road test. The remaining 178 participants were randomized, 90 to the control group and 88 to the intervention group. All completed the 3-month follow-up evaluation except 4 people in the intervention group (3 refused to take the road test, another stopped driving permanently because of medical illness).
Figure 1.
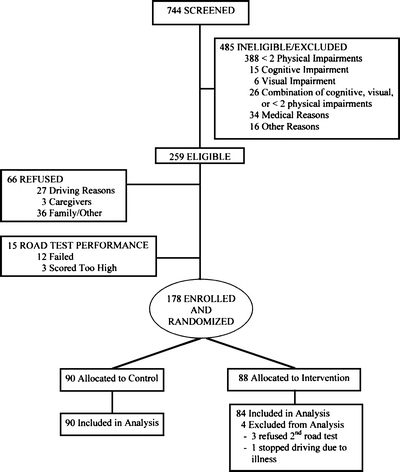
Screening and eligibility flow diagram.
Table 1 displays the baseline characteristics of the 178 participants. Participants had a mean age of 77 years, nearly one-third were women, two-thirds were recruited from clinic sites, and approximately three-fourths drove daily with a mean of 120 miles per week. Of the more than 20 factors assessed, only 1 factor (the number expected by chance), manual dexterity, was significantly different between the groups.
Table 1.
Baseline Characteristics of Participants in the Intervention and Control Groups
| Characteristics | Intervention (n = 88) | Control (n = 90) | P value* |
|---|---|---|---|
| Age | 77.4 (3.9) | 77.2 (4.6) | 0.70 |
| Mean in years (SD) | |||
| Education | 12.2 (2.8) | 12.6 (2.9) | 0.31 |
| Mean in years (SD) | |||
| Miles driven in a given week | 113 (93) | 128 (121) | 0.37 |
| Mean miles (SD) | |||
| Chronic conditions† | 1.8 (1.1) | 1.7 (1.1) | 0.53 |
| Mean number (SD) | |||
| Alcohol use† | 49 | 58 | 0.23 |
| Percent (%) presently drinks alcohol | |||
| Alcohol quantity x frequency | 1.8 (3.4) | 2.8 (4.8) | 0.12 |
| Mean (SD) | |||
| Medications† | 5.3 (3.3) | 4.7 (2.7) | 0.23 |
| Mean number (SD) | |||
| MMSE | 27.8 (1.6) | 27.9 (1.7) | 0.81 |
| Mean score (SD) | |||
| Distance acuity (20 / x) | 29.1 (9.1) | 30.4 (10.7) | 0.40 |
| Mean acuity, (SD) | |||
| Road test score | 59.8 (6.3) | 58.0 (7.7) | 0.09 |
| Mean Score (SD) | |||
| Gender | 32 | 31 | 0.92 |
| Percent (%) female | |||
| Race | 8 | 5 | 0.50 |
| Percent (%) non-white | |||
| Recruitment site | 65 | 66 | 0.91 |
| Percent (%) from clinic site | |||
| Driving frequency | 78 | 74 | 0.65 |
| Percent (%) drive daily | |||
| Self-rated health | 22 | 16 | 0.30 |
| Percent (%) fair/poor/bad | |||
| Fall history | 28 | 32 | 0.62 |
| Percent (%) with fall in past year | |||
| Manual dexterity | 36 | 53 | 0.02 |
| Percent (%) with impairment | |||
| Hip flexion | 70 | 59 | 0.11 |
| Percent (%) with impairment | |||
| Shoulder flexion | 20 | 23 | 0.64 |
| Percent (%) with impairment | |||
| Neck rotation | 95 | 89 | 0.10 |
| Percent (%) with impairment | |||
| Trunk rotation | 30 | 32 | 0.70 |
| Percent (%) with impairment | |||
| Mobility (gait speed) | 2 | 8 | 0.09 |
| Percent (%) with impairment | |||
| Foot abnormalities | 57 | 57 | 0.95 |
| Percent (%) with impairment | |||
*Continuous characteristics tested with a t-test and dichotomous tested with a chi-square
†Ascertained by self report
Driving Performance
Tables 2 and 3 display the scores on individual elements of the road test at baseline and types of critical errors committed. Figure 2 shows the observed baseline and 3-month road test scores by treatment group and by tercile of road test score. The least squares mean change in road test score at 3 months relative to baseline was 2.43 points higher in the intervention than in the control group (P = .03). This difference was evident for drivers in each tercile of baseline driving performance, with least squares mean change 0.68 points higher in the intervention than the control group in the high tercile, 1.83 points in the middle tercile, and 4.81 points in the low tercile (P = .29 for test of interaction). The treatment differences within each tercile are also apparent in Figure 2, with the intervention group declining slightly less than controls in the high tercile, remaining relatively stable while controls declined in the middle tercile, and improving while controls remained stable in the low tercile. The net effect was that the intervention group maintained driving performance while controls declined over the 3 months.
Table 2.
Baseline Road Test Components and Frequency of Occurrence (N = 178)
| Performance measurement | Poor (0) | Fair (1) | Good (2) | |||
|---|---|---|---|---|---|---|
| Number (N) | Percent (%) | Number (N) | Percent (%) | Number (N) | Percent (%) | |
| Scans to sides | 4 | 2 | 149 | 84 | 25 | 14 |
| Scans to rear/head check | 3 | 2 | 147 | 82 | 28 | 16 |
| Uses Mirrors | 1 | 1 | 72 | 40 | 105 | 59 |
| Uses seat belt | 74 | 42 | N/A | N/A | 104 | 58 |
| Responds to traffic signals | 34 | 19 | 4 | 2 | 140 | 79 |
| Responds to vehicles/pedestrians | 13 | 7 | 19 | 11 | 146 | 82 |
| Grants right of way | 5 | 3 | 16 | 9 | 157 | 88 |
| Centers car in lane | 14 | 18 | 56 | 31 | 108 | 61 |
| Safe following distance | 3 | 2 | 99 | 55 | 76 | 43 |
| Uses directional signals | 32 | 18 | 96 | 54 | 50 | 28 |
| Positions car for turns | 21 | 12 | 22 | 12 | 135 | 76 |
| Proper lane selection | 11 | 6 | 29 | 16 | 138 | 78 |
| Gas to break reaction time | N/A | N/A | 2 | 1 | 176 | 99 |
| Appropriate steering recovery | N/A | N/A | N/A | N/A | 178 | 100 |
| Acceleration | 1 | <1 | 7 | 4 | 170 | 96 |
| Braking | 2 | 1 | 14 | 8 | 162 | 91 |
| Shifting | 1 | 1 | 4 | 2 | 173 | 97 |
| Right turns | N/A | N/A | 1 | 1 | 177 | 99 |
| Left turns | 6 | 4 | 70 | 39 | 102 | 57 |
| Backing up | 1 | 1 | 122 | 68 | 55 | 31 |
| K turns | 24 | 13 | 3 | 2 | 151 | 85 |
| Angle parking | 18 | 10 | 20 | 11 | 140 | 79 |
| Low density traffic areas | N/A | N/A | 25 | 14 | 153 | 86 |
| Simple traffic situations | N/A | N/A | 27 | 15 | 151 | 85 |
| Medium traffic situations | 1 | 1 | 31 | 17 | 146 | 82 |
| Limited access highway | 3 | 2 | 31 | 17 | 140 | 81 |
| Enter | 15 | 8 | 29 | 17 | 130 | 75 |
| Exit | 5 | 3 | 8 | 5 | 160 | 92 |
| Merge | 4 | 2 | 29 | 17 | 144 | 81 |
| Lane change | 5 | 3 | 148 | 83 | 25 | 14 |
| Speed regulation | 7 | 4 | 103 | 58 | 68 | 38 |
| Follows direction | 6 | 3 | 96 | 54 | 76 | 43 |
| Judgment | 2 | 1 | 25 | 14 | 151 | 85 |
| Decision making | 6 | 3 | 41 | 23 | 131 | 74 |
| Memory | 7 | 4 | 93 | 52 | 78 | 44 |
| Attitude/emotions | 1 | 1 | 2 | 1 | 175 | 98 |
Table 3.
Baseline Critical Errors
| Outcome | Number (N) | Percentage (%) |
|---|---|---|
| Types of critical errors | ||
| Inattention | 60 | 34 |
| Lane changes without looking | 21 | 12 |
| Disobey traffic signs/signals | 38 | 21 |
Figure 2.
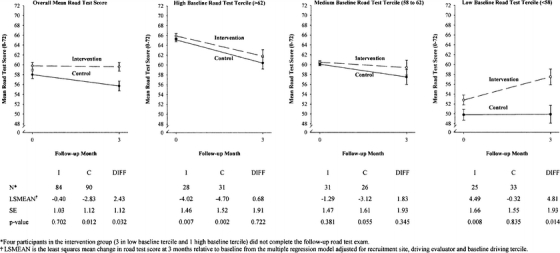
Comparison of road test scores at baseline and 3 months for intervention and control groups.
Table 4 displays the observed distribution of critical errors and the driving evaluator’s overall rating at baseline and 3 months by treatment group. Participants in the intervention group had a 37% lower number of critical errors than the control group (57 vs 91; P = .08, Poisson regression). Although there were fewer intervention drivers in the “major problem” category (6% vs 12%) at 3 months, the distribution of the driving evaluator’s overall rating was comparable in the two treatment groups (P = .29, ordinal regression).
Table 4.
Observed Distribution of Secondary Driving Outcomes at Baseline and 3 Months for Intervention and Control Groups
| Outcome | Baseline | P value | 3-Month follow-up | P value | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Intervention | Control | Intervention | Control | |||||||
| Number (n) | Percent (%) | Number (n) | Percent (%) | Number (n) | Percent (%) | Number (n) | Percent (%) | |||
| Critical errors | ||||||||||
| 0 | 46 | 52 | 41 | 46 | 0.379 | 46 | 55 | 38 | 42 | 0.076* |
| 1 | 34 | 39 | 33 | 37 | 23 | 27 | 21 | 23 | ||
| 2 | 7 | 8 | 13 | 14 | 11 | 13 | 23 | 26 | ||
| 3 | 1 | 1 | 3 | 3 | 4 | 5 | 8 | 9 | ||
| Evaluator rating† | ||||||||||
| 1 | 5 | 6 | 4 | 4 | 0.061 | 6 | 7 | 4 | 5 | 0.287‡ |
| 2 | 51 | 58 | 51 | 57 | 40 | 48 | 38 | 42 | ||
| 3 | 32 | 36 | 28 | 31 | 33 | 39 | 37 | 41 | ||
| 4 | 0 | 0 | 7 | 8 | 5 | 6 | 11 | 12 | ||
*The adjusted regression coefficient for intervention relative to control (standard error) from the Poisson regression model was −0.316 (0.178) yielding an expected number of critical errors (95% confidence interval) of 0.729 (0.514, 1.033), which was 27.1% fewer critical errors in the intervention than in the control group (95% confidence limits, 48.6% lower to 3.3% higher).
†Evaluator rating of overall driving performance was coded as 1 for no problem, 2 for minor problem, 3 for moderate problem, and 4 for major problem.
‡The adjusted regression coefficient for intervention relative to control (standard error) from the ordinal regression model was −0.317 (0.298) yielding an odds ratio (95% confidence interval) of 0.728 (0.406, 1.306), or the odds of participants in the intervention group having a worse (higher) evaluator rating was 27.2% lower than the odds for controls (95% confidence limits, 59.4% lower to 30.6% higher).
Adherence and Safety
Intervention participants reported completing the exercises a median of 5.4 days per week for both extremity and axial exercises. The exercise program was safe, with no major injuries reported during the study. Complaints of pain were noted by the intervention therapist in 2/779 (0.3%) weekly reports for extremity exercises and 10/784 (1.3%) weekly reports for axial exercises. There were fewer falls over the 3 months among intervention participants compared to controls [9/86 (10%) vs 18/90 (20%), P = .16].
DISCUSSION
Overall, the physical conditioning intervention was acceptable, safe, and effective in enhancing driving performance relative to controls. There was a least squares mean difference of 2.43 points at 3 months on a 72-point scale of driving performance, comparing intervention to control participants. The net effect was that the intervention group maintained their driving performance, while controls declined over the 3-month intervention period. This benefit was most noticeable among drivers with lower baseline driving scores. The exercise regimen was well tolerated with no injuries reported, and few complaints of pain.
The strengths of this study include its design, a randomized controlled trial of an exercise intervention with blinded intervention arm assignment and end point assessment. Also, participants were volunteers drawn from clinic sites and the community at large, but were not referred because of suspicion of driving difficulties. Two-thirds of participants were enrolled from clinical sites and are likely to be reflective of patients attending a doctor’s visit.
Several study features and findings suggest broad potential applicability. The intervention exercise regimen was designed to be safe, able to be performed in the home, and completed in 15 minutes or less and, thus, is applicable to an aging population with arthritis and other causes of physical impairment. Further analyses will determine if the protocol can be streamlined to enhance efficiency.
The trend toward fewer falls among intervention participants, while not statistically significant, is consistent with recent reports suggesting possible common risk factors for falls and crashes.32,38 If this association is confirmed in a cohort powered to detect a difference in falls, then the intervention’s potential benefits for driving performance and fall risk would make its clinical relevance and applicability even broader.
There were several limitations of the study. First, although 2.43 points is a meaningful difference from a driving evaluator’s perspective as established before the study, the clinical relevance of such a difference is unknown. Whether this difference translates to a difference in crash occurrence or driving patterns over time is uncertain. Data from a similar cohort of 552 drivers we have followed prospectively indicates that a one-point increase in the 72-point scale equates to a 3.3% decrease in crash occurrence over 2 years of follow-up. Extrapolating to the current findings, the overall 2.43 point treatment difference would equate to an 8% lower crash occurrence over 2 years among intervention participants, whereas the 4.81 point difference between groups in the lowest baseline tercile would translate to a 16% lower crash occurrence (data available on request). The trend toward fewer critical errors in the intervention group also suggests direct clinical relevance. Second, while the number of female and minority participants was relatively low, the proportion of drivers in these demographic groups is reflective of this geographic area based on earlier studies.
Current discussion regarding age and driving safety has centered on the question of who is at risk and whether anything can be done to improve or maintain driving performance. Given the importance of this determination and its implications, including limiting or stopping driving and potential negative effects on autonomy, mobility, out-of-home activity participation, and depressive symptoms, the issue has often been cast in a negative light, with reluctance on the part of drivers and clinicians to address it. A number of initiatives have been undertaken to facilitate and provide a framework for this discussion.39,40
This study demonstrated that it is possible to maintain or enhance driving performance among older drivers using a safe, well-tolerated physical conditioning program. The availability of such an intervention may change the content and tenor of clinician–patient discussions on this topic from a negative interaction regarding the need to limit or stop driving to a more positive one of possible interventions to prolong safe driving by maintaining or enhancing driving ability. Hopefully, this would increase the likelihood of this important issue being addressed.
Acknowledgements
The authors thank Robbin Bonanno for her assistance in preparing this manuscript.
Grant Support Claude D. Pepper Older Americans Independence Center at Yale Intervention Development Study (P60-AG10469- NIA); Dr. Marottoli was supported by a VA Health Services Research and Development Career Development Award, a Beeson Physician Faculty Scholars in Aging Research Award, and a Donaghue Foundation Investigator Award.
Potential Financial Conflicts of Interests None disclosed.
References
- 1.Waller PF. The older driver. Hum Factors. 1991;33:499–505. [DOI] [PubMed]
- 2.Retchin SM, Anapolle J. An overview of the older driver. Clin Geriatr Med. 1993;9:279–96. [PubMed]
- 3.Brody JA, Brock DB, Williams TF. Trends in the health of the elderly population. Annu Rev Public Health. 1987;8:211–34. [DOI] [PubMed]
- 4.Barancik JI, Chatterjee BF, Greene Cradden YC, et al. Motor vehicle trauma in Northeastern Ohio. I: Incidence and outcome by age, sex, and road-use category. Am J Epidemiol. 1986; 123:846–61. [DOI] [PubMed]
- 5.Fife D, Barancik JI, Chatterjee BF. Northeastern Ohio Trauma Study: II. Injury rates by age, sex, and cause. Am J Public Health. 1984;74:473–8. [DOI] [PMC free article] [PubMed]
- 6.Evans L. Older driver involvement in fatal and severe traffic crashes. J Gerontol: Soc Sci. 1988;43:S186–93. [DOI] [PubMed]
- 7.Rosenbloom S. Transportation needs of the elderly population. Clin Geriatr Med. 1993;9:297–310. [PubMed]
- 8.Jette AM, Branch LG. A ten-year follow-up of driving patterns among the community-dwelling elderly. Hum Factors. 1992;34:25–31. [DOI] [PubMed]
- 9.Bygren LO, Konlaan BB, Johansson SE. Attendance at cultural events, reading books or periodicals, and making music or singing in a choir as determinants for survival: Swedish interview survey of living conditions. Br Med J. 1996;313:1577–80. [DOI] [PMC free article] [PubMed]
- 10.Glass TA, Mendes de Leon C, Marottoli RA, Berkman LF. Population based study of social and productive activities as predictors of survival among elderly Americans. Br Med J. 1999;319:478–83. [DOI] [PMC free article] [PubMed]
- 11.House JS, Robbins C, Metzner HL. The association of social relationships and activities with mortality: prospective evidence from the Tecumseh community health study. Am J Epidemiol. 1982;116:123–40. [DOI] [PubMed]
- 12.Phillips DP, King EW. Death takes a holiday: mortality surrounding major social occasions. Lancet. 1988;II:728–32. [DOI] [PubMed]
- 13.Welin L, Larsson B, Svardsudd K, et al. Social network and activities in relation to mortality from cardiovascular diseases, cancer and other causes: a 12-year follow up of the study of men born in 1913 and 1923. J Epidemiol Community Health. 1992;46:127–32. [DOI] [PMC free article] [PubMed]
- 14.Marottoli RA, Mendes de Leon CF, Glass TA, et al. Consequences of driving cessation: decreased out of home activity levels. J Gerontol: Soc Sci. 2000;55B:S334–40. [DOI] [PubMed]
- 15.Fonda SJ, Wallace RB, Herzog AR. Changes in driving patterns and worsening depressive symptoms among older adults. J Gerontol: Soc Sci. 2001;56B:S343–51. [DOI] [PubMed]
- 16.Marottoli RA, Mendes de Leon CF, Glass TA, et al. Driving cessation and increased depressive symptoms: prospective evidence from the New Haven EPESE. J Am Geriatr Soc. 1997;45:202–6. [DOI] [PubMed]
- 17.Larsen GC, Stupey MR, Walance CG, et al. Recurrent cardiac events in survivors of ventricular fibrillation or tachycardia: implications for driving restrictions. JAMA. 1994;271:1335–9. [DOI] [PubMed]
- 18.Friedland RP, Koss E, Kumar A, et al. Motor vehicle crashes in dementia of the Alzheimer type. Ann Neurol. 1988;24:782–6. [DOI] [PubMed]
- 19.Drachman DA, Swearer JM. Driving and Alzheimer’s disease: the risk of crashes. Neurology. 1993;43:2448–56. [DOI] [PubMed]
- 20.Fitten LJ, Perryman KM, Wilkinson CJ, et al. Alzheimer and vascular dementias and driving: a prospective road and laboratory study. JAMA. 1995;273:1360–5. [DOI] [PubMed]
- 21.Hunt LA, Murphy CF, Carr D, et al. Reliability of the Washington University road test: a performance based assessment for drivers with dementia of the Alzheimer type. Arch Neurol. 1997;54:707–12. [DOI] [PubMed]
- 22.Hansotia P, Broste SK. The effect of epilepsy or diabetes mellitus on the risk of automobile accidents. N Engl J Med. 1991;324:22–6. [DOI] [PubMed]
- 23.McLay P. The Parkinsonian and driving. Int Disabil Stud. 1989;11:50–1. [DOI] [PubMed]
- 24.Findley LJ, Unverzagt ME, Suratt PM. Automobile accidents involving patients with obstructive sleep apnea. Am Rev Respir Dis. 1988;138:337–40. [DOI] [PubMed]
- 25.Legh-Smith J, Wade DT, Langton Hewer R. Driving after a stroke. J Royal Soc Med. 1986;79:200–3. [DOI] [PMC free article] [PubMed]
- 26.Wilson T, Smith T. Driving after stroke. Int Rehabil Med. 1983;5:170–7. [DOI] [PubMed]
- 27.Decina LE, Staplin L. Retrospective evaluation of alternative vision screening criteria for older and younger drivers. Accid Anal Prev. 1993;25:267–75. [DOI] [PubMed]
- 28.Johnson CA, Keltner JL. Incidence of visual field loss in 20,000 eyes and its relationship to driving performance. Arch Ophthalmol. 1983;101:371–5. [DOI] [PubMed]
- 29.Klein R. Age-related eye disease, visual impairment, and driving in the elderly. Hum Factors. 1991;33:521–5. [DOI] [PubMed]
- 30.Owsley C, Ball K, Sloane ME, et al. Visual/cognitive correlates of vehicle accidents in older drivers. Psychol Aging. 1991;6:403–15. [DOI] [PubMed]
- 31.Owsley C, Ball K, McGwin G, et al. Visual processing impairment and risk of motor vehicle crash among older adults. JAMA. 1998;279:1083–8. [DOI] [PubMed]
- 32.Margolis KL, Kerani RP, McGovern P, et al. Study of osteoporotic fractures research group. Risk factors for motor vehicle crashes in older women. J Gerontol: Med Sci. 2002;57A:M186–91. [DOI] [PubMed]
- 33.Marottoli RA, Cooney LM, Wagner DR, et al. Predictors of automobile crashes and moving violations among elderly drivers. Ann Intern Med. 1994;121:842–6. [DOI] [PubMed]
- 34.Marottoli RA, Richardson ED, Stowe M, et al. Development of a test battery to identify older drivers at risk for self-reported adverse driving events. J Am Geriatr Soc. 1998;46:562–8. [DOI] [PubMed]
- 35.Folstein MF, Folstein SE, McHugh PR. Mini-mental state: a practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res. 1975;12:189–98. [DOI] [PubMed]
- 36.Richardson ED, Marottoli RA. Visual attention and driving behavior among community-living older persons. J Gerontol: Med Sci. 2003;58:832–6. [DOI] [PubMed]
- 37.Allison LD. Logistic Regression Using the SAS® System: Theory and Application. Cary, NC: SAS Institute, Inc; 1999.
- 38.Sims RV, Owsley C, Allman RM, et al. A preliminary assessment of the medical and functional factors associated with vehicle crashes by older adults. J Am Geriatr Soc. 1998;46:556–61. [DOI] [PubMed]
- 39.Wang CC, Kosinkski CJ, Schwartzberg JG, Shanklin AV. Physicians Guide to Assessing and Counseling Older Drivers. Washington, DC: National Highway Traffic Safety Administration; 2003.
- 40.Ageing and Transport: Mobility Needs and Safety Issues. Paris, France: Organisation for Economic Cooperation and Development; 2001.