

Abstract
Objective
To analyze factors associated with leaving employment among women with newly diagnosed rheumatoid arthritis (RA) in two patient cohorts.
Methods
Women with RA were recruited from a national sample of rheumatologists in 1987 and 1998. Patients had to be diagnosed with RA for less than 18 months, 18 yrs and older, have no other disabling health condition. 48 and 91 women were in the 1987 and 1998 cohorts, respectively. Data were collected by phone for 4 yrs. Survival analysis was conducted using Kaplan-Meier curves and a proportional hazards generalized linear model to assess whether the time to stopping work differed between the cohorts and to identify baseline predictors and time-varying covariates of leaving work.
Results
Most patients were <50 years, married, >12 years education, white. Fifteen patients (31%) in the 1987 and 24 pts (26%) in the 1998 cohort stopped working in the observation periods. Kaplan-Meier survival curves for each cohort were not significantly different. Multivariate analyses showed women in 1998 cohort were significantly more likely to stop working compared to the earlier cohort (p=0.03) as were married women (p=0.03), those with more joint deformities (p=0.00) and more disease flares (p=0.00). A significant flares by cohort interaction (p=0.01) showed that for the 1987 cohort, those with one or more disease flares had the greatest risk of stopping work.
Conclusion
Unexpectedly, the cumulative rate of stopping work among women in the 1998 study did not differ from that among women diagnosed more than 16 years ago. However, disease flares greatly affected employment in the 1987 but not the 1998 cohort which may indicate that newer medications are effective in maintaining functional status among those with more severe disease activity, measured by number of flares, in the 1998 group.
Introduction
Studies of the psychosocial impacts of rheumatoid arthritis (RA) indicate that disability in paid work is a pervasive social problem (1 2 3 4 5 6 7 8) for RA patients. Many studies of indicate that demographic factors, work characteristics, and health status are related to maintaining employment (9 10 11 12 13). Recent reviews (1 14) of factors contributing to risk of work disability indicate consistency among studies in finding that physically demanding work, lack of autonomy, worse pain and functional status and fewer years of education are associated with increased risk of work disability.
A limitation of some studies of RA and patterns of work disability is that people have had the diagnosis of RA for many years and recall bias may influence the reliability of the data. Furthermore, it is possible that the ability to maintain paid work and to maintain better physical and psychological health status is determined fairly early in the disease course. Studies investigating the experience of people in the early days of the RA diagnosis (within the past 12 to 24 months) are mixed on whether the greatest risk of work disability and functional declines occur early (15). Some investigators report that impacts of RA occur before the diagnosis or soon after (4 14 16 17 18 19 20 21 22 23 24 25) and that these early experiences may determine longer-term consequences over the course of the disease. Others suggest that disability occurs much later in the disease course (26 27 28). As with studies of patients with long term disease, studies of RA during the early years find that health status, family and work factors contribute to increased risk of work disability (29).
Recent developments in the management of early RA with aggressive use of disease modifying antirheumatic drugs (DMARDs) and the newer biologic agents may contribute to lower rates of functional decline and work disability (30). The effects of these treatments and cost-effectiveness have not been studied extensively (31 32). Two groups have shown that early use of DMARDs in the management of RA helps maintain work capacity (33 34) and reduces the risk of work disability (35). The few studies of the effects of etanercept and infliximab (36 37) show that use of these drugs is associated with higher employment rates and more hours worked per week.
The purpose of this study was to investigate rates of work disability among women with recent onset RA and to assess demographic, work characteristic and health status factors that affect the risk of becoming work disabled. The data are from two cohorts of RA patients, one from women recruited in 1987–88 and the other from women recruited in 1998–2000. Both cohorts were followed for four years. Having data from two cohorts ten years apart offers a unique opportunity to determine whether factors influencing risk of work disability remain constant over time and whether trends in work disability have improved. Analysis of these two cohorts offers the opportunity to assess temporal changes in the illness experiences of women with recent onset RA and whether factors influencing risk of work disability changed in the time period. Much has been learned about the impacts of RA in the early period just before and after diagnosis. Having such a historical record will contribute to a better understanding of how and whether these impacts have changed over time.
We hypothesized that: 1) the rate of work disability would be lower in the 1998 cohort than the 1987 cohort because of improvements in disease management and advances in pharmaceutical therapies; 2) women who had less severe self-reported symptoms would have lower rates of work disability; 3) women who had less demanding family work would have lower rates of work disability; 4) women who were more satisfied with employment, had less physically demanding work, better employment benefits, such as paid sick leave, and wanted to work would have lower rates of work disability compared to other women.
Materials and Methods
Sample
Both samples were recruited with a two stage selection process. First, for both studies, a random sample of rheumatologists using a table of random numbers was selected from the membership of the American College of Rheumatology (formerly American Rheumatism Association). In the 1987 study, 116 physicians were randomly selected. Of those asked to participate, 56 agreed to refer any patients (male or female) with classic or definite RA according to the ACR criteria (38) regardless of time since diagnosis. In the 1998 study, 644 physicians were randomly selected, were asked to participate and 189 agreed. The lower response rate (29%) in 1998 likely reflects the greater clinical demands on rheumatologists and the increased number of requests to participate in clinical trials. Physicians in the 1998 study were asked to refer women with a diagnosis of RA using current ACR criteria (39) and only those who had been diagnosed with the past 12 months. Because of lagging recruitment, we expanded the inclusion criteria to include women diagnosed within 18 months.
Second, office staff in both studies asked patients to complete a response card which was sent to the University of Connecticut. Research staff telephoned prospective participants, explained the study, and conducted a telephone interview at a convenient time. Participants were interviewed annually by telephone for the next three years. Physicians also completed a clinical assessment form in the baseline year.
For this analysis, the sample for the 1987 cohort was assembled by selecting employed women diagnosed within the past year from the final sample. In the 1987 study 1,049 people returned response cards, 988 completed the baseline interview and 498 were employed. Of these 498 employed participants, 107 were diagnosed in the past year and 48 were women. In the 1998 study, 187 female patients returned response cards to the university staff. Of these, 30 were not eligible, 23 refused and 157 agree to participate. Of these, 91 women were employed.
Possible Sample Bias
There could be some small differences in the samples because of the changed diagnostic criteria and the differences in time since diagnosis. Regarding the diagnostic criteria, our exclusion criteria for the 1987 sample align well with the 1987 criteria; therefore, we don’t believe that there are any differences in the diagnosis of RA for women included in the two samples. We only included definite and classic RA patients in the 1987 study; we excluded those with a probable or possible diagnosis; finally, we excluded anyone who had other rheumatic conditions from both samples. As Arnett and colleagues (39) point out, “the new criteria preserve continuity by retaining many features of the old criteria set and, in fact, closely parallel the old definition of definite or classic RA (p.321).”
There also could be some small differences in the sample because we expanded recruitment in the 1998 study to include those diagnosed at 18 months. We believe that 12 or 18 months is an arbitrary cut-off and many studies of recent onset RA include those diagnosed for up to two years. The critical factor is that we have captured women in the early course of their disease in both studies. It is not possible to identify with great precision the exact date of onset of the disease or symptoms thus we relied on the date of diagnosis which could be documented. Including some women with more time since diagnosis in the 1998 study should not appreciably affect the results particularly since the majority, 84 of the 91 patients, in the 1998 study were diagnosed 12 months or less.
Variables
Data were collected on demographic, health status, work and family characteristics.
Demographics
Demographic characteristics included age, years of formal education, marital status and race. Income was assessed using the US census categories and dichotomized at the median income of $40,000 adjusted to 1998 dollars for the 1987 participants.
Work Characteristics
Participants reported total number of hours worked, how much they liked work, whether they preferred to work full-time, part-time or not at all, whether their job was mostly mental, mostly physical or part mental and physical, occupation, whether they supervised people and how much paid sick time they had. These variables were dichotomized for the analyses as follows: total number of hours was grouped into less than 40 hours and 40 or more hours per week; those who liked work a great deal were compared to those who liked work somewhat or not at all; wanting to work full-time was compared to part-time and not at all; mostly mental work was compared to part mental and mostly physical; white collar workers were compared to those in blue collar occupations.
Family/Social Characteristics
Participants were asked to rate satisfaction with their ability to perform household duties from very satisfied to very dissatisfied and if they could take a day off easily. They also reported the number people living in the household. Satisfaction with ability was dichotomized into very satisfied and satisfied in one group and neutral, dissatisfied and very dissatisfied into a second group. Being able to take a day off very easily was compared to not easily or not able to do. Number in the household was divided into 1-2 people and more than 2.
Social support was evaluated by the Qualitative Social Support Scale designed to measure how supportive the social network is perceived to be. It contains 20 Likert-type items scored on a scale of 1 (never true) to 4 (always true) asking about perceptions of social support received by important others, such as feedback, task assistance, and ego support. Four items assessed relationship strain (e.g. the extent to which a relationship is stressful) and were reverse scored (40) (Chronbach’s alpha = .82).
Self-Reported Health Status
Pain was assessed using a visual analogue scale. Participants were asked to rate pain on the day of the interview from zero (no pain) to 100 (the most pain possible). Missed work one or more days was compared to not missing any days; and sick time was grouped as a week or more or some/none.
Physician Assessed Health Status
Physicians were asked to complete a clinical assessment form at baseline. They reported the number of flares in the past year, presence of joint deformities in six areas (wrists/hands, ankles/feet, shoulder, elbows, knees, other); radiographic stage (41) (I, II, III, IV) and presence of rheumatoid factor. For the analyses, the variables were dichotomized at the median category. For flares, this was two or more, for joint deformities, one or more and for stage it was II or higher (none of the participants was in Stage IV).
Data Analysis
Survival analysis methods were applied to identify variables that affected risk of terminating employment in the time following entry to the study. Survival curves, using the Kaplan-Meier method, were used to inspect employment patterns relative to time and to identify any systematic differences in continuation or cessation of employment between the two cohorts. Because data on the continuation/cessation of employment were collected only at the time of annual interviews, the times of changes in employment status were “interval” censored. Following Hosmer and Lemeshow (42), we applied a modified form of proportional hazards regression that allowed us to model relationships between patient characteristics and employment and to account for interval censoring. Models were fitted using bivariate and multivariate approaches to understand both the effects of individual variables on employment and the simultaneous effects of multiple variables. Since the study samples were assembled using a two-stage nested sampling approach, standard errors, statistical tests, and confidence interval estimates based on these models were adjusted for the effects of cluster sampling.
In the multivariate analyses, model building was performed by entering variables sequentially in five blocks. The blocks and their order were: demographic variables, self-assessed health status, physician-assessed health status, family/social characteristics, and employment characteristics. Within each block, a forward stepwise selection strategy was applied based on a 5% level of significance. Variables found to be significant within a block were retained when the next block of variables was evaluated. The cohort effect –i.e., whether the participant was in the 1987 or 1998 cohort, was included as a covariate throughout the model building process. Once all blocks had been evaluated, first-order interaction terms were evaluated. Due to the limited sample size, potential interaction terms were added to the model only one at a time. In the final models with interaction terms, we decided to include variables based on a 10% level of significance because the small sample size might obscure significant effects that were worthy of investigation in future studies.
Results
Description of the Samples
Table 1 presents data on the descriptive characteristics of the women in the studies. Most women were less than 50 years of age, had more than a high school education, were married and were white. The only significant difference in the demographic characteristics between the two cohorts was that the women in the 1998 cohort were in more affluent households adjusting to 1998 dollars.
Table 1.
Comparison of Baseline Characteristics Between 1987 and 1998 Cohorts of Women with Recently Diagnosed RA who were Employed at Study Entry
| % (N) 1987 Cohort (N = 48) | % (N) 1998 Cohort (N = 91) | |
|---|---|---|
| Demographic Characteristics | ||
| Age 50 and Over | 43.8 (21) | 33.0 (27) |
| Beyond High School Education | 47.9 (23) | 60.4 (55) |
| Married | 60.4 (29) | 61.5 (56) |
| Non-Hispanic White | 87.5 (42) | 80.2 (73) |
| Income Over $40,000 (adjusted to 1998 Income levels)‡ | 41.7 (20) | 59.3 (54) |
| Work Status | ||
| Work 40 or More Hours Per Week | 52.1 (25) | 64.8 (59) |
| Like Work a Great Deal‡ | 64.6 (31) | 44.0 (40) |
| Want Full-time Work | 45.8 (22) | 31.9 (29) |
| Mostly Mental Job | 18.8 (9) | 30.8 (28) |
| White Collar | 79.2 (38) | 76.9 (70) |
| Supervisor | 45.8 (28) | 40.7 (37) |
| A Week or More of Sick Time per Year | 54.2 (26) | 54.9 (50) |
| Family/Social Characteristics | ||
| Very Satisfied and Satisfied with Household Activities | 52.1 (25) | 49.5 (45) |
| 1–2 People in Household | 45.8 (22) | 53.8 (49) |
| High Social Support (63 and over) | 50.0 (25) | 50.5 (46) |
| Very Easily Take Day Off | 54.2 (26) | 53.8 (49) |
| Self-Assessed Health Status | ||
| High Pain (25 and over) | 56.3 (27) | 60.4 (55) |
| Missed Work 1 or More Days Past Week | 16.7 (8) | 20.9 (19) |
| Physician-Assessed Health Status | ||
| High Total Flares (2 or more) | 68.8 (33) | 60.4 (55) |
| High Total Joint Deformities (1 or more) ‡ | 39.6 (19) | 22.0 (20) |
| Disease Stage of II or III‡ | 52.1 (25) | 23.1 (21) |
| Rheumatoid Factor Positive‡ | 33.3 (41) | 76.9 (70) |
Proportions are significantly different using a Chi-Square test statistic with p < .05
Women in the two cohorts had working conditions that were similar. Most participants worked 40 or more hours per week although most did not want to work full-time and would have preferred part-time work or staying at home. The only significant difference was that women in the 1987 cohort liked their jobs more than women in the 1998 cohort.
There were no significant differences in family structure or family work responsibilities and most women reported ability to take a day off easily, satisfaction with ability to do family work and were in households with 1–2 additional people. Most women had supportive social networks with a median score of 63 of a possible total of 80.
Physicians reported that disease activity was fairly high among women in both cohorts with more than 60% reporting two or more flares in the previous year. Physicians also reported a high percent of women already having deformities in at least one joint group within the first year of diagnosis. Women in the earlier cohort had significantly more deformities than the later group, 39.6% in the 1987 group compared to 22% in the 1998 group. Further, women in the earlier cohort were significantly more likely to be in Radiographic Stage II or III indicating that, overall, women in the earlier cohort were in worse clinical health status as assessed by their physicians. Interestingly, more women in 1998 were positive for rheumatoid factor which could be a function of more sensitive laboratory testing in the later years.
Cohorts were similar on self-reported pain levels and days missed from work. Most participants (56.4% in the 1987 cohort and 60.4% in the 1998 cohort) reported a score of 25 or more on the 100-point visual analogue scale and 16% to 20% missed one or more day from work in the previous week.
Figure 1 presents Kaplan-Meier survival curves comparing employment patterns relative to time for the 1987 cohort (dotted line) to that for the 1998 cohort (solid line). In total, 15 of 48 patients in the 1987 cohort (31%) and 24 of the 91 patients in the 1998 cohort (26%) stopped working in the follow-up period. As shown in Table 2, a higher cumulative proportion of subjects in the 1987 cohort ended employment during the follow-up period, the differences in overall survival patterns were not significantly different. The hazard ratio (HR) was 0.83 with the 95% CI of 0.44–1.58. (p=0.58). The cumulative proportions in both cohorts approximated the well-established rate of about half of those employed at onset of disease leaving the workforce within 10 years (28). It should be noted, however, that once participants left employment, they were censored or dropped from the analyses. Some participants may have returned to work at a later date.
Figure 1.
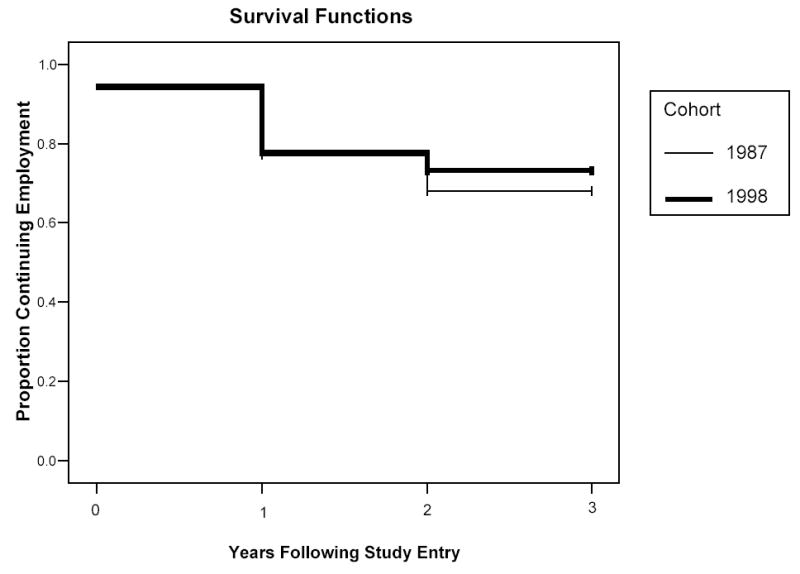
Proportion Continuing Employment Among the 1987 and 1998 Cohorts
Table 2.
Results of Fitting Bivariate Models to Investigate Relationships Between Baseline Characteristics and Risk of Discontinuing Work Data Adjusting for Study Cohort
| Cumulative Percentage Who Discontinued Work | Hazard Ratio | 95% CI | P-Value | |
|---|---|---|---|---|
| Study Cohort | ||||
| Cohort | ||||
| 1987 | 31.3 | Comparison Group | ||
| 1998 | 26.4 | 0.83 | 0.44–1.58 | 0.57 |
| Demographic Characteristics | ||||
| Age† | ||||
| Less than 50 | 26.1 | Comparison Group | ||
| 50 or More | 31.4 | 1.22 | 0.64–2.31 | 0.54 |
| Education, yrs | ||||
| 12 or More | 23.1 | 1.56 | 0.83–2.94 | 0.17 |
| Less than 12 | 34.4 | Comparison Group | ||
| Marital Status | ||||
| Not Married | 18.5 | Comparison Group | ||
| Married | 34.1 | 2.02 | 0.98–4.16 | 0.06 |
| Race | ||||
| Non-white | 41.7 | Comparison Group | ||
| White | 25.2 | 0.47 | 0.22–0.99 | 0.05 |
| Adjusted Income† | ||||
| Less than 40,000 | 23.1 | Comparison Group | ||
| 40,000 or More | 32.4 | 1.72 | 0.87–3.40 | 0.12 |
| Employment Characteristics | ||||
| Work Hours | ||||
| Less than 40 | 32.1 | Comparison Group | ||
| 40 or More | 25.3 | 0.68 | 0.36–1.28 | 0.29 |
| Like Work† | ||||
| Mod/Not at All | 32.4 | Comparison Group | ||
| Great Deal | 23.9 | 0.52 | 0.27–0.99 | 0.05 |
| Desire for Paid Work | ||||
| Want Part Time or Stay Home | 29.5 | Comparison Group | ||
| Want Full Time | 25.5 | 0.89 | 0.45–1.75 | 0.74 |
| Physical Demands of Job | ||||
| Mostly Physical or Both | 30.4 | Comparison Group | ||
| Mostly Mental | 21.6 | 0.67 | 0.31–1.48 | 0.32 |
| Occupation | ||||
| Blue Collar | 38.7 | Comparison Group | ||
| White collar | 25.0 | 0.53 | 0.27–1.04 | 0.07 |
| Supervise Others | ||||
| No | 28.8 | Comparison Group | ||
| Yes | 27.1 | 0.85 | 0.45–1.62 | 0.63 |
| Paid Sick Days† | ||||
| Less than Week | 35.5 | Comparison Group | ||
| Week or More | 19.0 | 0.54 | 0.29–1.00 | 0.05 |
| Family/Social Characteristics | ||||
| Satisfaction with Household Activity† | ||||
| Not Satisfied | 31.9 | Comparison Group | ||
| Satisfied/Very | 24.3 | 0.83 | .44–1.57 | 0.57 |
| Take Day Off | ||||
| Not Easy | 31.3 | Comparison Group | ||
| Very Easy | 25.3 | 0.82 | .44–1.53 | 0.53 |
| Number People in House† | ||||
| 3 or More | 35.3 | Comparison Group | ||
| 1–2 | 21.1 | 0.65 | .34–1.22 | 0.18 |
| Social Support† | ||||
| Less Than 64 | 23.2 | Comparison Group | ||
| 64 and Over | 32.9 | 1.40 | .74–2.64 | 0.30 |
| Health Status | ||||
| Total Number of Joint Deformities | ||||
| No Deformities | 20.0 | Comparison Group | ||
| 1 or More | 48.7 | 2.74 | 1.45–5.19 | 0.01 |
| Total Number Flares | ||||
| 0 or 1 | 23.5 | Comparison Group | ||
| 2 or More | 30.7 | 1.49 | .75–2.94 | 0.25 |
| Disease Stage | ||||
| Stage I | 23.7 | Comparison Group | ||
| Stage II or III | 37.0 | 1.67 | .86–3.27 | 0.13 |
| Rheumatoid Factor | ||||
| Negative | 35.8 | Comparison Group | ||
| Positive | 23.3 | 0.61 | .31–1.22 | 0.17 |
| Self-Reported Pain† | ||||
| Less Than 25 | 33.3 | Comparison Group | ||
| 25 and Over | 24.4 | 0.93 | .49–1.76 | 0.82 |
| Missed work† | ||||
| No Missed Work | 24.1 | Comparison Group | ||
| 1 or More Days | 44.4 | 1.90 | 0.92–3.92 | 0.08 |
Time Dependent Covariate
Bivariate Associations between Demographic, Work, Family and Health Status Characteristics and Stopping Work
Table 2 presents the HRs from a series of regression models in which cessation of employment was the dependent variable and each demographic, work, family, or health status measure was entered as a single covariate. The only significant demographic characteristic related to risk of leaving work was race, with whites having about half (HR =0.47; 95% CI=0.22–0.99) the risk of leaving employment compared to non-whites.
The only significant employment characteristic associated with risk of work disability was how much participants liked their work. Those who liked their work a great deal had about half the risk of becoming work disabled compared to those who reported liking work a moderate amount or not at all (HR=0.52; 95% CI=0.27–0.99; p=0.048).
Among the physician-assessed variables, having one or more joint deformity greatly increased the risk the leaving employment. Those with one or more deformity were almost three times as likely to stop working as those with no deformity (HR=2.74; 95% CI=1.45–5.19; p=0.002).
Self-reported pain and days missed from work were not significantly related to risk of work disability.
Multivariate Analysis
Table 3 presents the results of the model building process. In the presence of other predictive factors, women without flares in the more recent study (1998 cohort) were significantly more likely to stop working compared to women without flares in the earlier cohort (HR=6.6; 95% CI=1.19–36.5; p=0.03). Women who were married were more likely to stop working than those who were not married (HR=3.34; 95% CI=1.5–7.4; p=0.01). Clinical health status reported by physicians was very important as those with more joint deformities and those with more disease flares were considerably more likely to stop working compared to those with no deformities (HR=3.37; 95% CI=1.74–6.5; p=0.00) and those not having any disease flares (HR=8.8; 95% CI=2.0–38.7; p=0.01).
Table 3.
Variables included in the final multivariate model of continuation/cessation of employment
| Hazard Ratio | 95% CI | P-value | |
|---|---|---|---|
| 1998 Study Member | 6.60 | 1.19–36.46 | 0.03 |
| White | 0.52 | 0.24–1.11 | 0.09 |
| Married | 3.34 | 1.51–7.39 | 0.01 |
| White Collar Occupation | 0.49 | 0.20–1.16 | 0.11 |
| One or More Joint Deformity | 3.37 | 1.74–6.50 | 0.00 |
| Two or More Flares in Past Year | 8.80 | 2.0–38.73 | 0.01 |
| Flares by Cohort Interaction | 0.09 | 0.02–0.49 | 0.01 |
The effect of flares differed between cohorts in that there was a significant flares by cohort interaction (p=0.01). Those in the earlier study with more flares were more likely to leave employment. Figure 2 illustrates the interaction effect. The solid and dashed thick lines representing the 1998 cohort almost completely overlap indicating that their risk was the same regardless of number of flares. For the 1987 cohort, those with no flares (thin dotted line) were the least likely to leave employment while women with one or more disease flares (thin solid line) had the greatest risk of stopping work.
Figure 2.

Proportion Continuing Employment Among Those with and without Flares in the 1987 and 1998 Cohorts
Two other variables remained in the model, although they did not achieve statistical significance. Being white (p<0.09) and having a white collar occupation reduced the risk of work disability (p=0.106) compared to non-whites (HR=0.52; 95% CI=0.24–1.11) and those with blue collar work (HR=0.49; 95% CI=0.2–1.16), respectively.
Discussion
There has been considerable discussion of whether impacts of RA occur early in the disease process or whether disease progression occurs slowly with more limited impacts in the early years. This analysis offers the unique opportunity to examine impacts with respect to paid work and whether they have changed over time. The women who participated in this study had been diagnosed with RA for less than 18 months. The physicians of the participants reported considerable disease activity among their patients in the previous year with more than 60% having had two or more disease flares, 60% having had one or more joint deformities, and a third having progressed to Stage II or III in one year. Women in the more recent cohort have better overall clinical status compared to the earlier study despite a greater prevalence of positive rheumatoid factor among the more recent cohort. This improved clinical picture could be the result of more effective clinical management among women in the 1998 cohort compared to the 1987 cohort, including prescription of new medications. Interestingly, self-reported pain levels were about the same in the two groups with a majority reporting pain scores greater than 25 on a 100-point scale and 30% reporting pain levels greater than 50.
The cumulative rate of work disability among the women in the two samples is high –31% and 26% for the 1987 and 1998 cohorts respectively. These rates are similar to those reported in European studies of recent onset RA that followed patients for five rather than four years (43). This represents a major social impact of RA which occurs fairly early in the disease course for these women. The rate is slightly lower for women in the 1998 cohort, but these differences were not significant.
Our study found clinical factors to be very important in becoming work disabled. Having more flares and deformed joints greatly increased the risk of leaving the workforce. The interaction effect, which indicated that flares were important only for women in the earlier cohort, was intriguing. It suggests that reasons for leaving work are changing in that those entering the study in 1998 left the workforce for reasons other than increased disease activity. These factors in 1998 might include the negative effects of prevailing economic conditions and/or the changing economic structure towards a more service based economy. Further investigation is needed to assess the underlying mechanisms accounting for this effect.
Finally, marital status was a significant factor in that married women had a greater tendency to leave the workforce compared to those who were unmarried. This may be related to financial assistance that a spouse provides. It also could be related to the greater physical and social demands placed on married women with families. Although family size and satisfaction with performing household activities were not significantly related to work disability, other factors such as family-work conflict and the instrumental and nurturant family demands could be important risk factors for work disability and deserve further attention.
The results of this study should be viewed cautiously. Different diagnostic criteria were used in the two samples although the changes in the criteria should not make any appreciable difference in the diagnosis of RA among women in the two studies. However, because disease flares were much more important in the earlier cohort there is a possibility that changes in criteria could have an effect. There also could be some differences in the samples because the 1998 sample included women who have had a diagnosis of RA for a longer period. Again, this should not have a major effect on the results as we have captured women in the early experiences of the disease. Small sample size limited the power of the study to detect small effects and the possibility of investigating the effects of simultaneous interactions between covariates. Thus, some effects that were clinically significant and that could have policy implications for the management of RA patients may have been missed. Some important variables about the structure of paid and family work, such as control over work and work demands, which are potentially critical variables for women with a chronic health condition, were not analyzed because this information was not uniformly collected in both samples. However, the results are consistent with other studies of people with recent onset RA and further builds on what is known about disease progression in the early years.
Footnotes
Supported by a grant from the National Arthritis Foundation and the Multipurpose Arthritis Center, NIAMS grant #AR20621
References
- 1.Allaire SH. Update on work disability in rheumatic diseases. Curr Opin Rheumatol. 2001;13(2):93–8. doi: 10.1097/00002281-200103000-00001. [DOI] [PubMed] [Google Scholar]
- 2.Backman CL. Employment and work disability in rheumatoid arthritis. Curr Opin Rheumatol. 2004 Mar;16:148–52. doi: 10.1097/00002281-200403000-00014. [DOI] [PubMed] [Google Scholar]
- 3.Sokka T. Work disability in early rheumatoid arthritis. Clin Exp Rheumatol. 2003;21(Suppl 31):S71–4. [PubMed] [Google Scholar]
- 4.Hallert E, Husberg M, Jonsson D, Skogh T. Rheumatoid arthritis is already expensive during the first year of the disease (the Swedish TIRA project) Rheumatology. 2004;43:1374–82. doi: 10.1093/rheumatology/keh324. [DOI] [PubMed] [Google Scholar]
- 5.Burton W, Morrison A, Maclean R, Ruderman E. Systematic review of studies of productivity loss due to rheumatoid arthritis. Occup Med (Lond) 2005 Nov 11; doi: 10.1093/occmed/kqi171. Epub ahead of print. [DOI] [PubMed] [Google Scholar]
- 6.Wolfe F, Michaud K, Choi HK, Williams R. Household income and earnings losses among 6,396 persons with rheumatoid arthritis. J Rheumatol. 2005;32:1875–83. [PubMed] [Google Scholar]
- 7.Allaire S, Wolfe F, Niu J, Lavalley M, Michaud K. Work disability and its economic effect on 55-64-year-old adults with rheumatoid arthritis. Arthritis Rheum. 2005;53:603–8. doi: 10.1002/art.21326. [DOI] [PubMed] [Google Scholar]
- 8.Merkesdal S, Ruof J, Huelsemann JL, Mittendorf T, Handelmann S, Mau W, Zeidler H. Indirect cost assessment in patients with rheumatoid arthritis (RA): comparison of data from the health economic patient questionnaire HEQ-RA and insurance claims data. Arthritis Rheum. 2005;53:234–40. doi: 10.1002/art.21080. [DOI] [PubMed] [Google Scholar]
- 9.Yelin E, Henke C, Epstein W. The work dynamics of the person with rheumatoid arthritis. Arthritis Rheum. 1987;30:507–512. doi: 10.1002/art.1780300504. [DOI] [PubMed] [Google Scholar]
- 10.Yelin E, Meenan R, Nevitt M, Epstein W. Work disability in rheumatoid arthritis: The effects of disease, social and work factors. Ann Internal Med. 1980;93:551–556. doi: 10.7326/0003-4819-93-4-551. [DOI] [PubMed] [Google Scholar]
- 11.Reisine ST, Grady KE, Goodenow C, Fifield J. Work disability among women with rheumatoid arthritis: The relative importance of disease, social, work, and family factors. Arthritis Rheum. 1989;32:538–543. doi: 10.1002/anr.1780320505. [DOI] [PubMed] [Google Scholar]
- 12.Reisine S, McQuillan J, Fifield J. Predictors of work disability in rheumatoid arthritis patients: A five year follow-up. Arthritis Rheum. 1995;38:1630–37. doi: 10.1002/art.1780381115. [DOI] [PubMed] [Google Scholar]
- 13.Lacaille D, Sheps S, Spinell JJ, Chalmers A, Esdaile JM. Identification of modifiable work-related factors that influence the risk of work disability in rheumatoid arthritis. Arthritis Rheum. 2004;51:843–52. doi: 10.1002/art.20690. [DOI] [PubMed] [Google Scholar]
- 14.Sokka T, Pincus T. Markers for work disability in rheumatoid arthritis. J Rheumatol. 2001;28:1718–22. [PubMed] [Google Scholar]
- 15.Sokka T, Pincus T. A historical perspective concerning population-based and clinical studies of early arthritis and early rheumatoid arthritis. Clin Exp Rheumatol. 2003;21(Suppl 31):S5–S14. [PubMed] [Google Scholar]
- 16.Meenan RF, Kazis LE, Anthony JM, Wallin BA. The clinical and health status of patients with recent-onset rheumatoid arthritis. Arthritis Rheum. 1991;34:761–65. doi: 10.1002/art.1780340618. [DOI] [PubMed] [Google Scholar]
- 17.Doeglas D, Suurmeijer, Krol B, Sanderman R, van Leeuwen M, van Rijswijk M.Work disability in early rheumatoid arthritis. Ann Rheum Dis 1995;54:455–60. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Eberhardt K. Experiences from a prospective early rheumatoid arthritis study in southern Sweden. J Rheumatol Suppl. 2004;69:9–13. [PubMed] [Google Scholar]
- 19.Sokka T, Kautiainen H, Mottonen T, Hannonen P. Work disability in rheumatoid arthritis 10 years after the diagnosis. J Rheumatol. 1999;26:1681–5. [PubMed] [Google Scholar]
- 20.Barrett EM, Scott DGI, Wiles NJ, Symmons DPM. The impact of rheumatoid arthritis on employment status in the early years of disease: a UK community based study. Rheumatol. 2000;39:1403–09. doi: 10.1093/rheumatology/39.12.1403. [DOI] [PubMed] [Google Scholar]
- 21.Merkesdal S, Ruof J, Schoffski O, Bernitt K, Zeidler H, Mau W. Indirect medical costs in early rheumatoid arthritis: composition of and changes in indirect costs within the first three years of disease. Arthritis Rheum. 2001;44:528–34. doi: 10.1002/1529-0131(200103)44:3<528::AID-ANR100>3.0.CO;2-U. [DOI] [PubMed] [Google Scholar]
- 22.Young A, Dixey J, Kulinskaya E, Cox N, Davies P, Devlin J, Emery P, Gough A, James D, Prouse P, Williams P, Winfield J. Which patients stop working because of rheumatoid arthritis? Results of five years' follow up in 732 patients from the Early RA Study (ERAS) Ann Rheum Dis. 2002;61:335–40. doi: 10.1136/ard.61.4.335. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Fex E, Larsson BM, Nived K, Eberhardt K. Effect of rheumatoid arthritis on work status and social and leisure time activities in patients followed 8 years from onset. J Rheumatol. 1998;25:44–50. [PubMed] [Google Scholar]
- 24.Albers JM, Kuper HH, van Riel PL, Prevoo ML, van 't Hof MA, van Gestel AM, Severens JL. Socio-economic consequences of rheumatoid arthritis in the first years of the disease. Rheumatology (Oxford) 1999;38:423–30. doi: 10.1093/rheumatology/38.5.423. [DOI] [PubMed] [Google Scholar]
- 25.Jantti J, Aho K, Kaarela K, Kautiainen H. Work disability in an inception cohort of patients with seropositive rheumatoid arthritis: a 20 year study. Rheumatology (Oxford) 1999;38:1138–41. doi: 10.1093/rheumatology/38.11.1138. [DOI] [PubMed] [Google Scholar]
- 26.Wolfe F, Hawley D. The long-term outcomes of rheumatoid arthritis. Work disability: A prospective 18 year study 823 patients. J Rheumatol. 1998;25:2108–17. [PubMed] [Google Scholar]
- 27.Pugner KM, Scott DI, Holmes JW, Hieke K. The costs of rheumatoid arthritis: An international long-term view. Semin Arthritis Rheum. 2000;29:305–320. doi: 10.1016/s0049-0172(00)80017-7. [DOI] [PubMed] [Google Scholar]
- 28.Sheehan TJ, Dubrava S, Fifield J, Reisine S, DeChello LM. Rate of change in functional limitations for rheumatoid arthritis patients: effects of gender, age, and duration of illness. J Rheumatol. 2004;(7):1286–92. [PubMed] [Google Scholar]
- 29.Puolakka K, et al. Predictors of productivity loss in early rheumatoid arthritis: a 5 year follow up study. Ann Rheum Dis. 2005;64:130–33. doi: 10.1136/ard.2003.019034. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Verstappen SMM, van Albada-Kuipers GA, Bijsma JWJ, Blaauw AAM, Schenk Y, Haanan HCM, Jacobs JWG. A good response to early DMARD treatment of patients with rheumatoid arthritis in the first year predicts remission during follow up. Ann Rheum Dis. 2005;64:38–43. doi: 10.1136/ard.2003.014928. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Lacaille D. Arthritis and employment research: Where are we? Where do we need to go? J Rheumatol. 2005;32(Suppl 72):42–45. [PubMed] [Google Scholar]
- 32.Yelin E. Is early intervention worth it? J Rheumatol. 2005;32(Suppl 72):36–38. [PubMed] [Google Scholar]
- 33.Borg G, Allander E, Berg E, Brodin U, From A, Trang L. Auranofin treatment in early rheumatoid arthritis may postpone early retirement: results from a 2-year double blind trial. J Rheumatol. 1991;18:101–20. [PubMed] [Google Scholar]
- 34.Puolakka K, et al. Early suppression of disease activity in essential for maintenance of work capacity in patients with recent-onset rheumatoid arthritis. Arthritis Rheum. 2005;52:36–41. doi: 10.1002/art.20716. [DOI] [PubMed] [Google Scholar]
- 35.Puolakka K, Kautiainen H, Mottonen T, Hannonen P, Korpela M, Julkunen H, Luukkainen R, Vuori K, Paimela L, Blafield H, Hakala M, Leirisalo-Repo M. Impact of initial aggressive drug treatment with a combination of disease-modifying antirheumatic drugs on the development of work disability in early rheumatoid arthritis: a five-year randomized follow-up trial. Arthritis Rheum. 2004;50:55–62. doi: 10.1002/art.11436. [DOI] [PubMed] [Google Scholar]
- 36.Moreland LW. Drugs that block tumour necrosis factor: experience in patients with rheumatoid arthritis. Pharmacoeconomics. 2004;22(2 Suppl):39–53. doi: 10.2165/00019053-200422001-00005. [DOI] [PubMed] [Google Scholar]
- 37.Yelin E, Trupin L, Katz P, Lubeck D, Rush S, Wanke L. Association between etanercept use and employment outcomes among patients with rheumatoid arthritis. Arthritis Rheum. 2003;48:3046–54. doi: 10.1002/art.11285. [DOI] [PubMed] [Google Scholar]
- 38.Ropes MW, Bennett GA, Cobb S, Jacox R, Jessar RA. 1958 revision of diagnostic criteria for rheumatoid arthritis. Bull Rheum Dis. 1958;9:175–76. [PubMed] [Google Scholar]
- 39.Arnett FC, Edworthy SM, Block DA, McShane DJ, Fries JF, Cooper NS, et al. The American Rheumatism Association 1987 revised criteria for the classification of rheumatoid arthritis. Arthritis Rheum. 1988;31:315–24. doi: 10.1002/art.1780310302. [DOI] [PubMed] [Google Scholar]
- 40.Reisine S, Goodenow C, Grady KE. The impact of rheumatoid arthritis on the homemaker. Soc Sci Med. 1987;25:89–95. doi: 10.1016/0277-9536(87)90210-3. [DOI] [PubMed] [Google Scholar]
- 41.Steinbrocker O, Trager CH, Batterman RC. Therapeutic cireteria in rheumatoid arthritis. JAMA. 1949;140:659–662. doi: 10.1001/jama.1949.02900430001001. [DOI] [PubMed] [Google Scholar]
- 42.Hosmer DW, Lemeshow S. Applied Logistic Regression, Solutions Manual, Second Edition. New York: Wiley, 2001.
- 43.Puolakka K, Kautiainen H, Mottonen T, Hannonen P, Hakala M, Korpela M, Ilva K, Yli-Kerttula U, Piirainen H, Leirisalo-Repo M, FIN-RACo Trial Troup Predictors of productivity loss in early rheumatoid arthritis: a 5 year followup study. Ann Rheum Dis. 2005;64:130–3. doi: 10.1136/ard.2003.019034. [DOI] [PMC free article] [PubMed] [Google Scholar]