

Surgery (resection or transplantation) is the treatment of choice for early hepatocellular carcinoma (HCC) but unfortunately it is feasible in only a minority of patients.1 Local percutaneous ablation has therefore dramatically increased in importance and radiofrequency thermal ablation (RFTA) has been shown in recent reports to have global or disease free survival better than that reported for percutaneous ethanol injection (PEI).2 The recent report in Gut apparently also supports the superiority, albeit small, of RFTA over PEI or acetic acid injection in a randomised prospective controlled study (Gut 2005;54:1151–6). Nevertheless, not all agree on the efficacy of RFTA3 and major complications have been described.4 In Lin et al's study (Gut 2005;54:1151–6), the incidence of major complications was significantly higher than that with the ethanol or acetic acid injection procedures.
We have conducted a multicentre prospective study on the efficacy and complications of RFTA in HCC in North‐East Italy, involving 399 HCC patients and a centralised radiological assessment. Overall, 133 patients (33%) experienced some complications, five of which were severe (1.3%). There were two deaths (0.5%), one being procedure related (intestinal perforation) and the other a cerebral infarction.
Some authors have reported rapid intrahepatic progression after RFTA,5,6 a fact that deserves special attention. We documented nine cases of rapid unexpected spread of HCC after RFTA in our multicentre study. The nine cases (2.3% of the series) are reported in table 1 and examples are given in fig 1 (computed tomography (CT) scan, one month after RFTA; the lesion appears to be partially treated with no clearcut residual activity in the arterial CT phase) and fig 2 (after five months, complete reactivation of the original lesion and 13 new additional lesions were evident).
Table 1 Nine cases of rapid unexpected spread of hepatocellular carcinoma (HCC) after radiofrequency thermal ablation (RFTA).
| Patient No | Sex, age, aetiology | % Efficacy | No of nodules | Size before RFTA (cm) | New nodules (time/months) | Grading | AFP (ng/ml) |
|---|---|---|---|---|---|---|---|
| 1 | M, 79, HCV | 100% | 1 | 4.6 | Satellites + new controlateral HCC node (1 month) | G1 | 15.7 |
| 2 | M, 78, HBV | 90% | 2 | 2.4–3 | 3 (3 cm each) (3 months) | G1 | 32.9 |
| 3 | M, 61, HBV | 100% | 1 | 1.8 | Multifocal (>3) (4 months) | G1 | 32 |
| 4 | M, 68, HCV | 90% | 1 | 4.2 | 3 (1 month) | G1–G2 | 10 |
| 5 | M, 69, HCV | 100% | 2 | 4.2–1.5 | Multiple (up to 6 cm) (3 months) | – | 8 |
| 6 | M, 73, HCV | 100% | 1 | 4 | Multiple (>3) (1 month) | – | 32 |
| 7 | F, 73, HCV | 70% | 1 | 3.1 | 13 (5 months) | – | 117 |
| 8 | M, 65, HCV | 100% | 1 | 2.0 | 1 (8 cm) new lesion (7 months) | G1 | 12.6 |
| 9 | M, 72, HBV+ETOH | 100% | 1 | 2.8 | Multifocal (5 months) | G1 | 4.9 |
HBV, hepatitis B virus; HCV, hepatitis C virus; ETOH, alcohol; AFP, α fetoprotein.
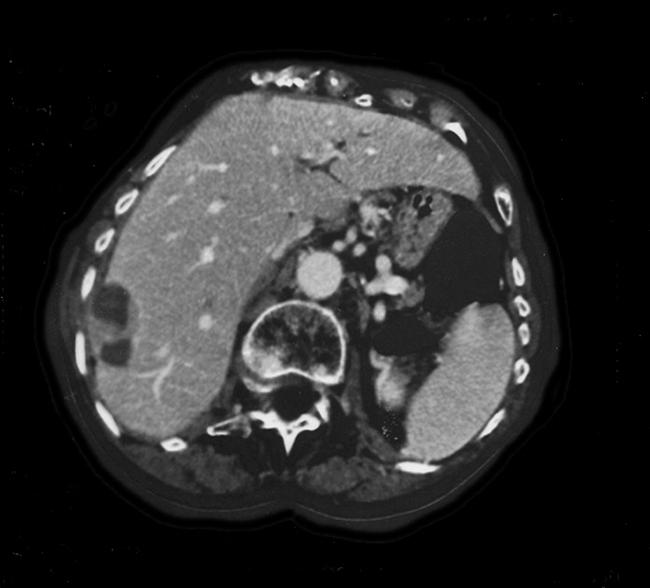
Figure 1 Computed tomography (CT) scan, one month after radiofrequency thermal ablation. The lesion appears to be partially treated with no clearcut residual activity in the arterial CT phase.
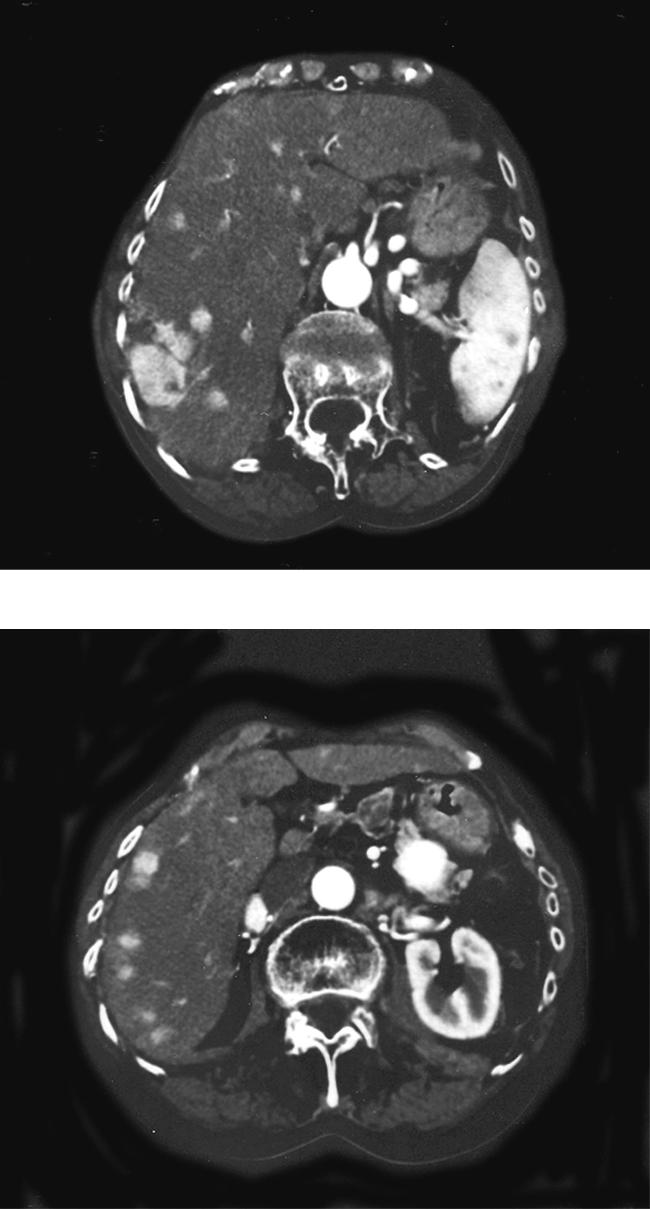
Figure 2 After five months, complete reactivation of the original lesion and 13 new additional lesions were evident.
This rapid unexplained and biologically unclear progression of HCC following RFTA treatment is most unusual considering the natural history of the disease. It may be prompted by increased intratumoral pressure with intravascular spread, seeding due to arterovenus fistula, or to the expandable hooks needles. Suggested risk factors have been high α fetoprotein levels, location near major portal branches, and poor tumour differentiation.4,5 Also, increased liver concentrations of growth factors (transforming growth factor β1 and β fibroblast growth factor) have been documented in rat liver after thermal coagulation, with increased HCC growth.7
Our data show that side effects are relatively frequent following RFTA, with a mortality rate less than 1%. Our series confirmed that “explosive HCC spread” may occur after RFTA, with no correlation with AFP, or differentiation or location of the tumour, and frequently even after total ablation.
Why do these patients develop this severe (and dramatic if observed in patients on waiting lists for orthotopic liver transplantation)8 and unexpected complication and what is its prevalence? Whether or not we can identify patients at risk is open to discussion, which we believe should be exhaustive before abandoning PEI as obsolete in favour of RFTA as the treatment of choice for early disease not eligible for surgery. Let us wait for the end of the honeymoon period of this new procedure!
Footnotes
Conflict of interest: None declared.
References
- 1.Christians K K, Pitt H A, Rilling W S.et al Hepatocellular carcinoma: multi‐modality management. Surgery 2001130554–560. [DOI] [PubMed] [Google Scholar]
- 2.Lencioni R, Cioni D, Crocetti L.et al Percutaneous ablation of hepatocellular carcinoma: state‐of‐the‐art. Liver Transpl 200410(suppl 1)S91–S97. [DOI] [PubMed] [Google Scholar]
- 3.Mazzaferro V, Battiston C, Perrone S.et al Radiofrequency ablation of small hepatocellular carcinoma in cirrhotic patients awaiting liver transplantation: a prospective study. Ann Surg 2004240900–909. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.De Baère T, Risse O, Kuoch V.et al Adverse event during radiofrequency treatment of 582 hepatic tumors. AJR Am J Roentgenol 2003181695–700. [DOI] [PubMed] [Google Scholar]
- 5.Ruzzante A, De Manzoni G, Molfetta M.et al Rapid progression of hepatocellular carcinoma after radiofrequency ablation. World J Gastroenterol 2004101137–1140. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Nicoli N, Casaril A, Hilal M A.et al A case of rapid intrahepatic dissemination of hepatocellular carcinoma after radiofrequency thermal ablation. Am J Surg 2004188165–167. [DOI] [PubMed] [Google Scholar]
- 7.Ohno T, Kawano K, Yokoyama H.et al Microwave coagulation therapy accelerates growth of cancer in rat liver. J Hepatol 200236774–779. [DOI] [PubMed] [Google Scholar]
- 8.Cillo U, Vitale A, Bassanello M.et al Liver transplantation for the treatment of moderately or well‐differentiated hepatocellular carcinoma. Ann Surg 2004239150–159. [DOI] [PMC free article] [PubMed] [Google Scholar]