

Abstract
Aim
To report a potential adverse effect of intensified treatment with sodium hyaluronate artificial tears.
Methods
Five cases of deep calcium deposition in the cornea associated with ocular surface disease and frequent use of hyaluronic acid artificial tears are described. All patients used one formulation of phosphate buffered hyaluronate eye drops when rapid calcification developed. All eyes required corneal graft surgery for visual rehabilitation. Specimens at keratoplasty were available for light microscopy and investigation by dispersive x ray analysis. The phosphate concentration in the medication used for topical treatment was measured and compared to alternative hyaluronate preparations.
Results
Light microscopy showed dense mineralisation of the entire stroma. The crystalline deposits consisted of hydroxyapatite, Ca5(PO4)3OH. A 50‐fold higher concentration of phosphate was measured in the sodium hyaluronate eye drops used for treatment (50.9 mmol/l) when compared with normal serum. The other hyaluronate formulations showed phosphate concentrations from <0.1 mmol/l to 10.9 mmol/l.
Conclusions
The hyaluronate artificial tear formulation “Hylo‐Comod” favours the formation of insoluble crystalline calcium phosphate deposits in presence of epithelial keratopathy. This is because of its high phosphate concentration and typically frequent instillation. Manufacturers and prescribers should be aware that topical preparations may contain considerable amounts of phosphate which may lead to sight threatening corneal complications.
Keywords: cornea, corneal calcification, calcareous degeneration, sodium hyaluronate, artificial tears
Calcium deposition in the cornea occurs as a spectrum of phenomena, ranging from subtle age related superficial changes to full thickness calcification with visual loss.1,2,3,4,5,6,7,8,9,10,11,12
Morphologically, two types of corneal calcium deposition are discerned. Most frequently it occurs as band shaped keratopathy which refers to calcium deposition in the Bowman's layer and superficial stroma, mainly in the interpalpebral zone.4 Calcareous degeneration is calcium deposition in the deeper stroma including Descemet's membrane.4,8,9,10 It may coexist with band shaped keratopathy and is denoted as extremely rare.5,9
This paper describes five patients who developed calcareous degeneration in association with ocular surface disease and frequent use of sodium hyaluronate artificial tears.
Materials and methods
In 2004 we observed six corneas of five patients that developed rapidly progressing calcification. The clinical situation is described below and summarised in table 1. Corneal graft surgery for visual rehabilitation was carried out in five eyes. The corneal buttons and the excised material became available for analysis.
Table 1 The clinical situation in which calcium deposition developed.
| Surface disease following | Epithelial keratopathy | Plaque formation observed within | Hyaluronate drops frequency | |||
|---|---|---|---|---|---|---|
| Case 1, left eye | Pseudomembranous conjunctivitis | diffuse punctate changes | 5 days | up to 100×/day | ||
| Case 1, right eye | Pseudomembranous conjunctivitis | circumscribed, irritating lash | 2 days | up to 100×/day | ||
| Case 2 | Mucous membrane pemphigoid | epithelial defect 2×2 mm | 1 week | up to 15×/day | ||
| Case 3 | Atopic keratoconjunctivitis | complete erosion | 5 days | 6×/day | ||
| Case 4 | Pars plana vitrectomy and diabetes | large epithelial defect | 2 weeks | up to 15×/day | ||
| Case 5 | Topical anaesthesia, Sjögren syndrome | epithelial defect 3×2 mm | 2 weeks | up to 30×/day |
Case 1
A 45 year old woman developed severe bilateral pseudomembranous conjunctivitis with subsequent conjunctival scarring. Several investigations failed to elucidate the nature of the initial disease process. Entropion repair was carried out on all four lids, but conjunctival inflammation with severe keratoconjunctivitis sicca persisted despite intensive lubrication. Four weeks after lid repair the left eye developed a large calcified corneal plaque (fig 1A). At this time, the patient was on a medication with ofloxacin (Floxal, Bausch & Lomb) three times per day, unpreserved dexamethasone phosphate (Dexasine, Alcon) three times daily, and very frequent preservative free hyaluronate eye drops (Hylo‐Comod, Ursapharm, Germany).
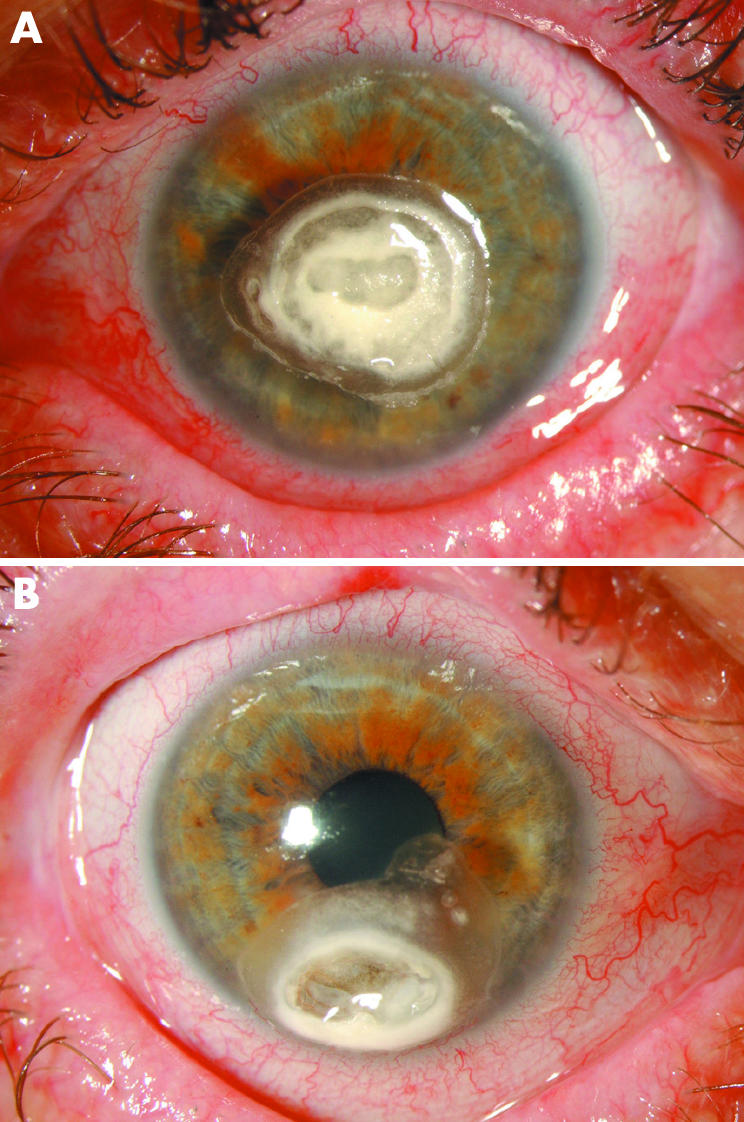
Figure 1 (A) Case 1 left eye. The grey white calcium phosphate deposits recurred within days after an attempt to remove them by superficial keratectomy. The calcification extended into the deep stroma. (B) Case 1 right eye. Calcified plaque that developed within 48 hours in an area previously affected by epithelial keratopathy following trichiasis. Note corneal thinning within the plaque that developed over 2 months and required emergency repair.
Three months later the right eye developed a similar plaque (fig 1B). Again calcium deposition occurred within a few days in an area previously affected by mild trichiasis. At this time, the right eye was receiving cefuroxime, dexamethasone (Maxidex, Alcon) three times daily and intensified lubrication with Hylo‐Comod. With disodium edate (EDTA) drops 0.16% three times daily, the plaque advanced only very slowly. Visual acuity remained at 6/12, but 4 months later corneal surgery became inevitable because of stromal thinning.
In the left eye a lamellar keratoplasty was planned, but during dissection it became obvious that the calcification had reached Descemet's membrane. Therefore, a penetrating keratoplasty had to be carried out. In the right eye the calcification was also full thickness. An eccentric patch keratoplasty allowed us to leave the central cornea intact, preserving visual acuity at 6/18.
Four weeks postoperatively a small superficial plaque in the graft of the left eye was noted. The patient was on topical ofloxacin, prednisolone acetate (Predforte, Allergan), and Hylo‐Comod. Excimer laser ablation of the plaque was carried out and the phosphate buffered Hylo‐Comod stopped and replaced by balanced salt solution (BSS, Alcon). The plaque did not recur.
Case 2
This 64 year old man with mucous membrane pemphigoid and cicatrising conjunctivitis developed an epithelial defect in his right eye. Lubrication with hyaluronate drops (Hylo‐Comod) every hour and topical ofloxacin three times daily was started. Multilayered amniotic membrane grafts were carried out twice, but the epithelial defect recurred. The lubrication with hyaluronate drops was intensified. One week later a dense band shaped calcification had developed. The calcification extended into the deep stroma, and a penetrating graft became inevitable.
Case 3
This 70 year old man with atopic eczema underwent penetrating keratoplasty several months after microbial keratitis. Postoperative topical therapy consisted of a combination of dexamethasone and gentamicin (Dexamytrex, Gerhard Mann GmbH, Germany) three times daily and of hyaluronate drops (Hylo‐Comod). The graft and large areas of the host cornea were completely denuded of epithelium. Six days postoperatively a large calcified corneal plaque developed. Over a period of 2 months the calcification expanded into Descemet's membrane. The cornea became available for examination when the keratoplasty was repeated.
Case 4
A 69 year old diabetic male underwent pars plana vitrectomy for vitreous haemorrhage. Ten days after the operation he developed a large epithelial defect that was treated with hourly hyaluronate artificial tears (Hylo‐Comod). In addition to the lubrication, he received Dexamytrex three times daily. On follow up 2 weeks later, a large calcified corneal plaque extended from the surface into the deep stroma. Corneal graft surgery was postponed because of poor visual prognosis.
Case 5
A 73 year old woman with primary Sjögren syndrome and moderate dry eyes underwent phacoemulsification under topical anaesthesia. Two weeks after surgery she developed a central epithelial keratopathy. Her topical lubrication with hyaluronate (Hylo‐Comod) was intensified (one drop every 30 minutes). The epithelial problems progressed, an epithelial defect developed, and after 2 months she presented with a non‐inflamed calcified ulcer (fig 2A–C). Apart from the lubrication, only ofloxacine drops were used three times daily. The Hylo‐Comod lucbrication was replaced by autologous serum. The calcification did not progress, but keratoplasty was required for visual rehabilitation.
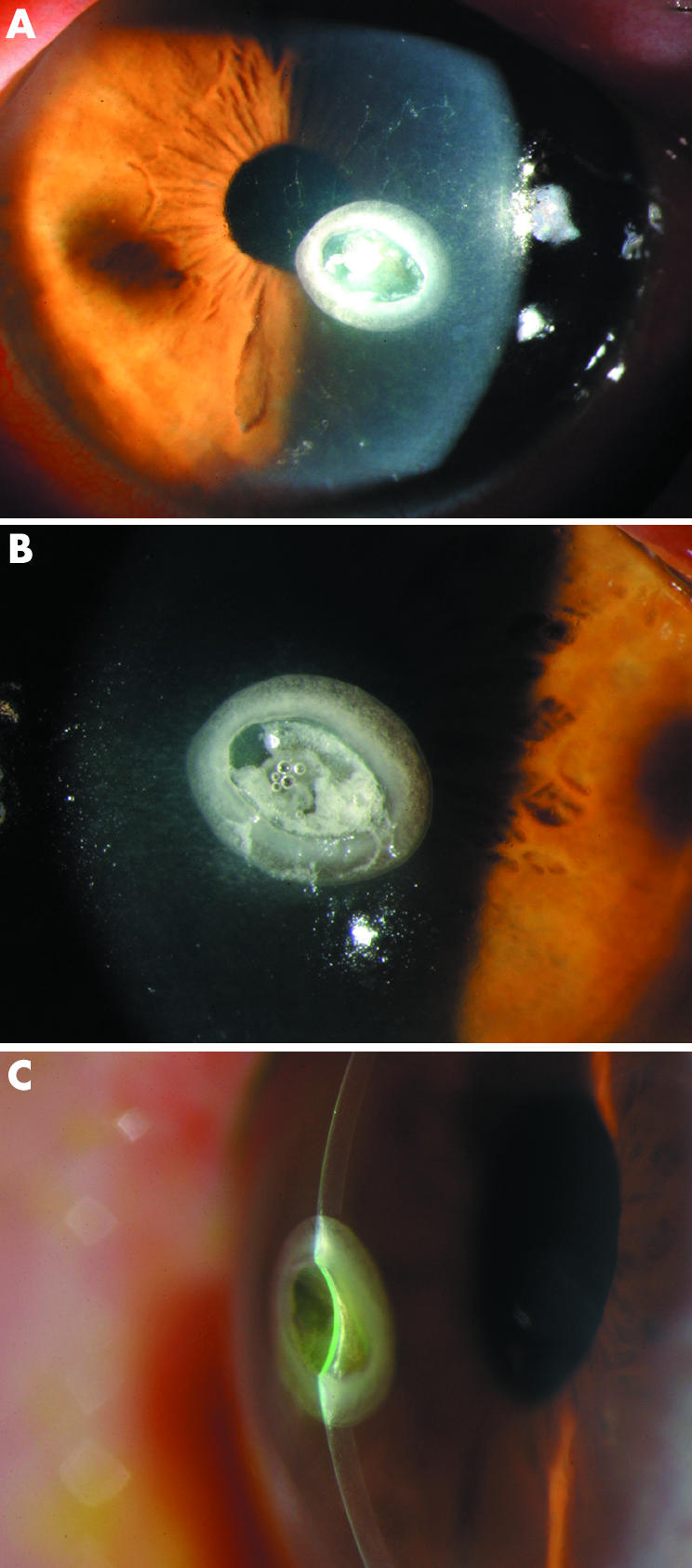
Figure 2 Case 5. (A) A progressive non‐inflamed calcified corneal ulcer developed on hyaluronate eye drops in an area of epithelial keratopathy. The patient had undergone uneventful phacoemulsification and had Sjögren syndrome. The calcification did not further progress after replacement of the phosphate rich lubricant by autologous serum. The ring shaped pattern of calcification is shown in (B), the central thinning in (C).
Histology
The corneal buttons were fixed in formalin and embedded in paraffin. Sections of 3 μm were studied, all stained with haematoxylin and eosin, von Kossa, periodic acid Schiff (PAS), combined Alcian blue PAS, and silver stains for fungal organisms.
X ray diffraction
The crystalline deposits of case 1 were pulverised and analysed by x ray diffraction using a CubixPro diffractometer (PANalytical, Almelo, NL) and Ni‐filtered CuKα radiation. The identification of the crystalline components was performed with the ICDD database (International Centre for Diffraction Data).
Phosphate concentration
The phosphate concentration of the medications that were used for topical treatment was measured and compared with other hyaluronate tear preparations. The quantification was performed with the molybdate method on a Modular P autoanalyser (Roche Diagnostics, Basel, Switzerland).
Results
Paraffin histology
Light microscopy showed a partial loss of epithelium and mineralisation of Bowman's membrane and the entire stroma. In four specimens, the calcification reached and involved Descemet's membrane. A mild inflammatory infiltrate was present in three corneas (nos 1, 3), but no micro‐organisms were detected. Figure 3 shows the extent and the variable appearance of the calcifications.

Figure 3 Case 1, light microscopy. The low power photomicrographs (A), (D), and (G) show the extent of the calcifications in both the left and the right cornea, affecting the entire thickness of the specimens. The calcifications are slightly more purple than the non‐calcified corneal stroma in these haematoxylin and eosin stained sections of cornea. The higher power photomicrographs (B), (E), and (H) show the variable histological appearance of the calcifications. The calcifications could consist of small concentrically laminated spherules (B) and (E), they could be confluent (indicated by the arrow in (B)), and form areas of solid plaque (arrowhead in (H)). Solid plaque formation could be seen in the centre of the lesion (open arrowhead in (B)) or at the periphery (arrowhead in (H)). The margin of affected corneal stroma could be sharp (arrowhead in (H)) or consist of a sprinkling of individually calcified spherules (arrowhead in (B)). Descemet's membrane of the left eye was detached from the corneal stroma after histotechnical processing (indicated by an arrowhead in (D)). It is therefore represented in the separate photomicrograph (F). Bowman's membrane (arrows in (H)) and Descemet's membrane (arrows in (F) and (I)) were found to show calcifications in both eyes.
X ray diffraction
The analysis of the diffractograms showed reflections at 2θ = 25.9°, 32.1°, and 39.6°. By automated library search the crystalline material was identified as 100% hydroxyapatite Ca5(PO4)3OH.
Phosphate concentration in eye drops
The phosphate concentration in the topical preparations used for treatment is listed in table 2.
Table 2 Phosphate concentration in the eye drop preparations that were used for treatment and that are commercially available.
| Phosphate, PO4 (mmol/l) | ||
|---|---|---|
| Sodium hyaluronate (Hylo‐Comod, Ursapharm, Germany) | 50.9 | |
| Dexamethasone phosphate 0.1% (Dexasine, Alcon) | 45.5 | |
| Dexamethasone alcohol 0.1% (Maxidex, Alcon) | 13.9 | |
| Dexamethasone phosphate 0.1%, gentamicin (Dexamytrex, Gerhard Mann Gmbh, Germany) | 70.3 | |
| Prednisolone acetate 1% (Predforte, Allergan) | <0.1 | |
| Ofloxacin 0.3 % (Floxal, Bausch & Lomb) | 0.21 | |
| Balanced salt solution (BSS, Alcon) | <0.1 | |
| Normal serum, aqueous humour, and tears | 0.4–1.45 |
The phosphate concentration in hyaluronate eye drops ranged from 0.1–50.9 mmol/l. The highest concentration was found in Hylo‐Comod, the lubricant used by all our patients (table 3).
Table 3 The phosphate concentration of some sodium hyaluronate eye drop preparations that are commercially available in Europe.
| Phosphate, PO4 (mmol/l) | ||
|---|---|---|
| Hylo‐Comod, Ursapharm, Germany (0.1%)* | 50.9 | |
| Hyabak, Laboratoires Théa, France (0.15%) | 10.9 | |
| Vismed, TRB chemedica, Germany (0.18%) | 10.5 | |
| Comfort Shield, i.com medical GmbH, Germany (0.15%) | 2.3 | |
| Hyal‐drop, Bausch & Lomb (0.2%) | 2 | |
| Fermavisc, Novartis Pharma (0.1%) | 1.7 | |
| Lacrycon, Pfizer (0.14%) | <0.1 |
*The concentration of sodium hyaluronate is given in parentheses.
Discussion
Superficial calcium deposition in the cornea is relatively common and treatable with chelating agents or ablation. In contrast, calcification involving the deep corneal layers is rare and of great concern, particularly when it occurs following therapeutic measures and as rapidly as in our series.
Corneal calcification typically occurs as deposition of calcium phosphate.5,6,8,11 In our series, the crystalline material was identified as hydroxyapatite Ca5(PO4)3OH. Hydroxyapatite has a very low solubility, decreasing with increasing pH. The ion product of calcium cations and phosphate anions in aqueous humour, tears, and interstitial fluids is close to their solubility product, even under physiological conditions—that is, a minor increase of one of the components may push this system towards precipitation.2,12 A raised serum concentration of calcium or phosphate was not found in our patients. However, a local increase of free calcium may have occurred after tissue degradation as a result of inflammation, epithelial keratopathy, and amniotic membrane transplantation.
Topical medications have been implicated in corneal calcium deposition.5,6,7,13,14,15,16,17,18 Sporadic reports suspected the preservatives phenylmercuric nitrate13 and thiomersal14; retinoic acid,15 dexamethasone,16 and timolol17 play a part. More frequently the use of phosphate as part of an active steroid was thought to be linked with calcification.5,16,18 These reports, however, focused on the pharmaceutically active agent and have possibly neglected the coincident use of phosphate buffers in topical preparations.
The role of phosphate buffers in irrigating solutions has been studied.6,19,20 Rapid calcification may develop after chemical injury in presence of a large epithelial defect and an alkaline pH. Based on these observations it is plausible to suspect that phosphate buffers in eye drop preparations may act similarly.
In our series the phosphate buffers had the crucial role in the calcification process. Our cases have in common that the same phosphate rich formulation of sodium hyaluronate (Hylo‐Comod) was used for a prolonged period and very frequently. The intervals between applications were as short as every 10 minutes—that is, up to 100 drops were administered per day. Labelled as “preservative free” and in a multidose container for unpreserved, sterile eye preparations (Comod‐System, Ursatec, Germany), it took some time before we realised that the adjuvants in Hylo‐Comod were involved in the process of calcification. The high phosphate concentration led to a critical increase of the calcium phosphate ion product which, together with the breakdown of the tissue barrier, resulted in the formation of hydroxyapatite deposits.
As an alternative source of phosphate, the other medications had to be taken into account. Using our measurements we calculated that the amount of phosphate delivered by the other pharmaceuticals was minor. One patient (no 5) was solely on hyaluronate drops and little ofloxacin when the calcification started.
In conclusion, this study indicates that the hyaluronate artificial tear formulation “Hylo‐Comod” (also available as “Hycosan”) favours the formation of insoluble calcium phosphate deposits in the presence of epithelial keratopathy. This is because of its high phosphate concentration and typically frequent instillation. Manufacturers and prescribers should be aware that topical preparations, high in phosphate, may cause severe adverse effects when used very frequently and on a damaged corneal surface. The declaration of the amount of phosphate buffers on drop bottles and in the inserted information leaflets should be introduced. The manufacturer of “Hylo‐Comod” was informed and advised to reformulate this product.
Acknowledgements
The authors are grateful to Maja Baucamp for excellent histotechnical assistance.
Abbreviations
BSS - balanced salt solution
EDTA - disodium edate
PAS - periodic acid Schiff
Footnotes
Competing interests: none declared
Proprietary interest: none.
References
- 1.Cogan D G, Albright F, Bartter F C. Hypercalcaemia and band keratopathy. Report of 19 cases. Arch Ophthalmol 194840624–638. [Google Scholar]
- 2.Doughman D J, Olson G A, Nolan S.et al Experimental band keratopathy. Arch Ophthalmol 196981264–271. [DOI] [PubMed] [Google Scholar]
- 3.Klaassen‐Broekema N, van Bijsterveld O P. Limbal and corneal calcification in patients with chronic renal failure. Br J Ophthalmol 199377569–571. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Cursino J W, Fine B S. A histologic study of calcific and noncalcific band keratopathies. Am J Ophthalmol 197682395–404. [DOI] [PubMed] [Google Scholar]
- 5.Schlötzer‐Schrehardt U, Zagorski Z, Holbach L M.et al Corneal stromal calcification after topical steroid‐phosphate therapy. Arch Ophthalmol 19991171414–1418. [DOI] [PubMed] [Google Scholar]
- 6.Daly M, Tuft S J, Munro P M. Acute corneal calcification following chemical injury. Cornea 200524761–765. [DOI] [PubMed] [Google Scholar]
- 7.Anderson S B, de Souza R F, Hofmann‐Rummelt C.et al Corneal calcification after amniotic membrane transplantation. Br J Ophthalmol 200387587–591. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Freddo T F, Leibowitz H M. Bilateral acute corneal calcification. Ophthalmology 198592537–542. [DOI] [PubMed] [Google Scholar]
- 9.Sharif K W, Casey T A, Casey R.et al Penetrating keratoplasty for bilateral acute corneal calcification. Cornea 199211155–162. [DOI] [PubMed] [Google Scholar]
- 10.Lavid F J, Herreras J M, Calonge M.et al Calcareous corneal degeneration: report of two cases. Cornea 19951497–102. [PubMed] [Google Scholar]
- 11.Pecorella I, McCartney A C E, Lucas S.et al Acquired immunodeficiency syndrome and ocular calcification. Cornea 199615305–311. [DOI] [PubMed] [Google Scholar]
- 12.Nevyas A S, Raber I M, Eagle R C., Jret al Acute band keratopathy following intracameral Viscoat. Arch Ophthalmol 1987105958–964. [DOI] [PubMed] [Google Scholar]
- 13.Kennedy R E, Roca P D, Landers P H. Atypical band keratopathy in glaucomatous patients. Am J Ophthalmol 197172917–922. [DOI] [PubMed] [Google Scholar]
- 14.Lemp M A, Ralph R A. Rapid development of band keratopathy in dry eyes. Am J Ophthalmol 197783657–659. [DOI] [PubMed] [Google Scholar]
- 15.Avisar R, Deutsch D, Savir H. Corneal calcification in dry eye disorders associated with retinoic acid therapy. Am J Ophthalmol 1988106753–755. [DOI] [PubMed] [Google Scholar]
- 16.Weisenthal R W, Krachmer J H, Folberg R.et al Postkeratoplasty crystalline deposits mimicking bacterial infectious crystalline keratopathy. Am J Ophthalmol 198810570–74. [DOI] [PubMed] [Google Scholar]
- 17.Huige W M M, Beekhuis W H, Rijneveld W J.et al Unusual deposits in the superficial corneal stroma following combined use of topical corticosteroid and beta‐blocking medication. Doc Ophthalmol 199178169–175. [DOI] [PubMed] [Google Scholar]
- 18.Taravella M J, Stulting R D, Mader T H.et al Calcific band keratopathy associated with the use of topical steroid‐phosphate preparations. Arch Ophthalmol 1994112 pp 608-13 Erratum in Arch Ophthalmol 19941121608–1613. [DOI] [PubMed] [Google Scholar]
- 19.Schrage N F, Schloßmacher B, Aschenberner W.et al Phosphate buffer in alkali eye burns as an inducer of experimental corneal calcification. Burns 200127459–464. [DOI] [PubMed] [Google Scholar]
- 20.Huang Y, Meek K M, Mangat H.et al Acute calcification in alkali‐injured rabbit cornea treated with synthetic inhibitor of metalloproteinases (SIMP). Cornea 199817423–432. [DOI] [PubMed] [Google Scholar]