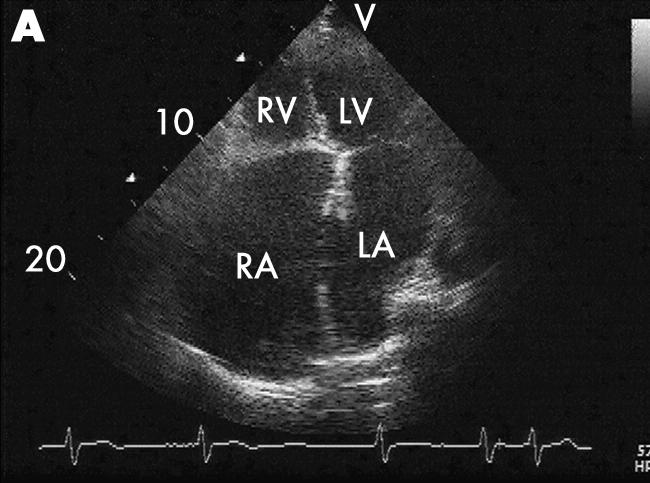
In March 1997, a 72 year old woman with a cardiothoracic ratio of 90% on chest x ray was admitted to our hospital with a haemorrhagic gastric ulcer. However, at that time, she had no cardiac symptoms. Epstein's anomaly was excluded and no other congenital or acquired cardiac abnormality without atrial fibrillation and tricuspid regurgitation was detected. We then made the diagnosis of idiopathic dilatation of the bilateral atria. In October 2003, she came back to our hospital because of congestive heart failure with progressing mitral regurgitation. The echocardiogram revealed notably enlarged atria (right atrium 115.0 × 73.7 mm in diameter; left atrium 102.0 × 53.5 mm in diameter) (panel A). However, no dilation of the ventricles was observed and systolic function was normal. Since bilateral heart failure was resistant to conventional treatment, she received surgical reduction of both atria and tricuspid and mitral valvular annuloplasty was performed because no organic valvular degeneration was confirmed in the operation. Microscopic examination revealed persistent myocarditis with severe scarring (panel B). The major histocompatibility complex (MHC) class I antigens, which are required for the action of direct cytotoxic T cells, were found to be expressed on the myocytes and over expressed in the interstitial spaces (panel C). MHC class II antigens were also over‐expressed in the interstitium. This case suggests that this congenital benign anomaly might be contributed to by atrial persistent myocarditis. This unique condition should be reinvestigated using up‐to‐date diagnostic tools.