

Abstract
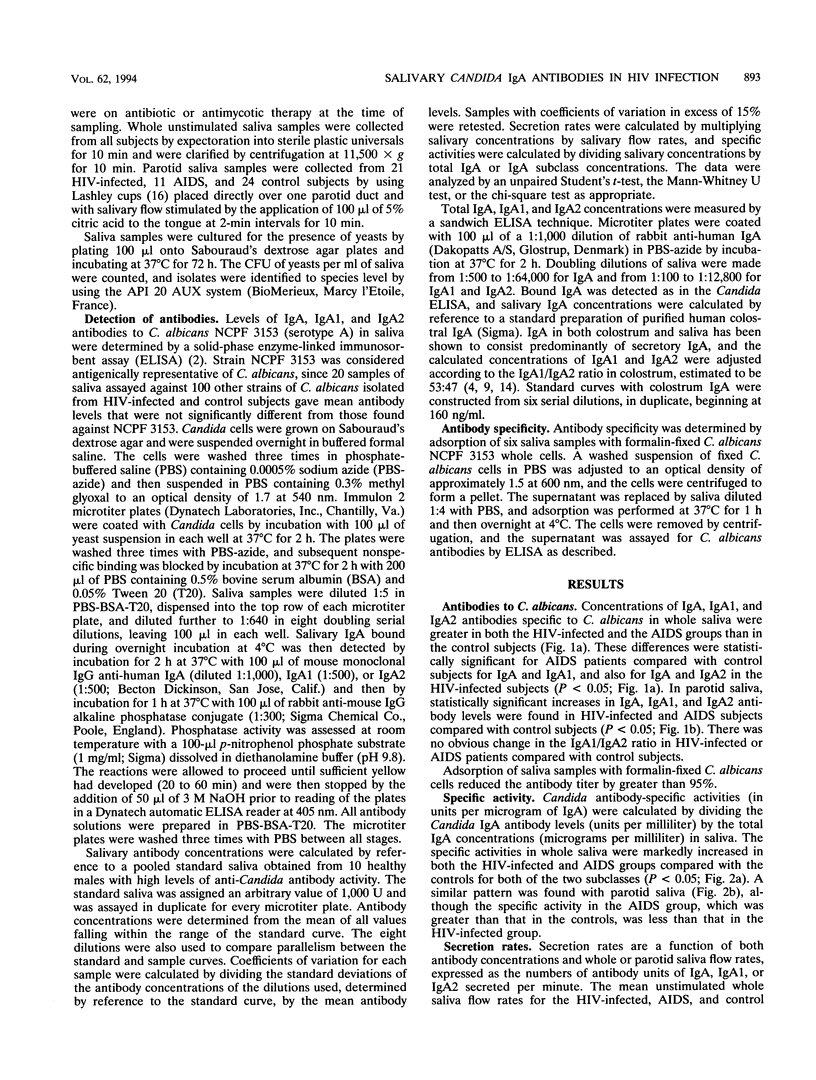
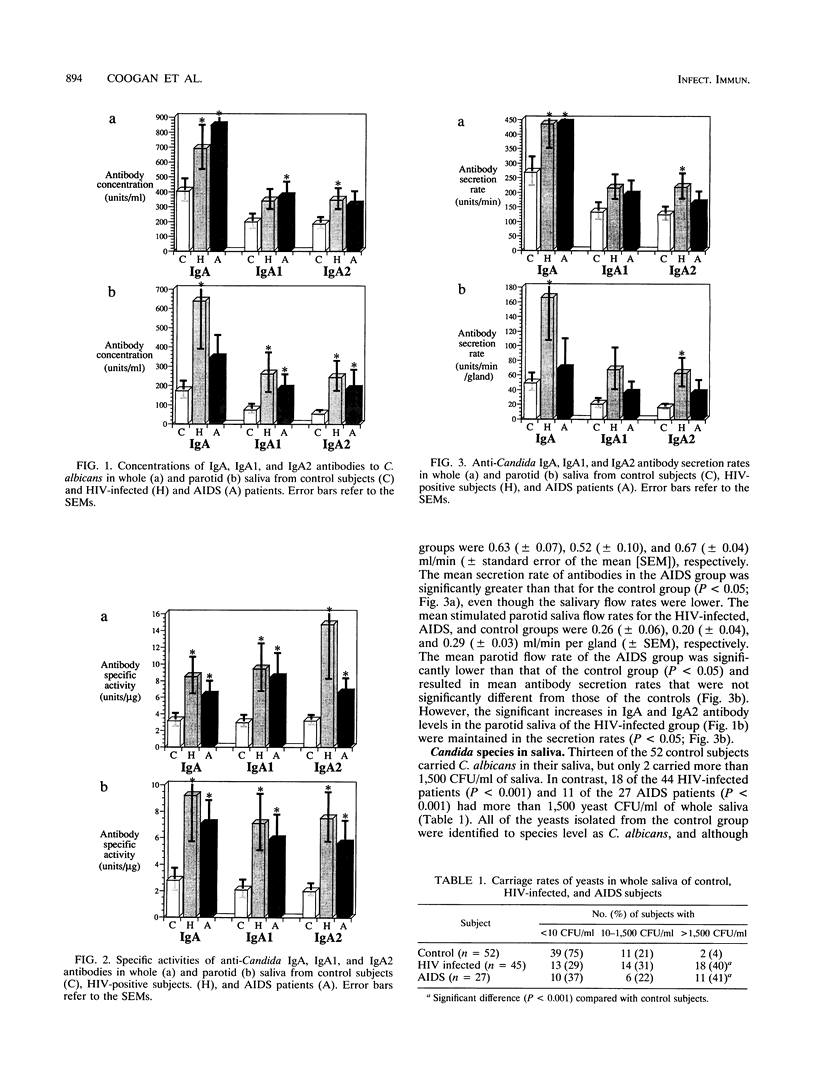
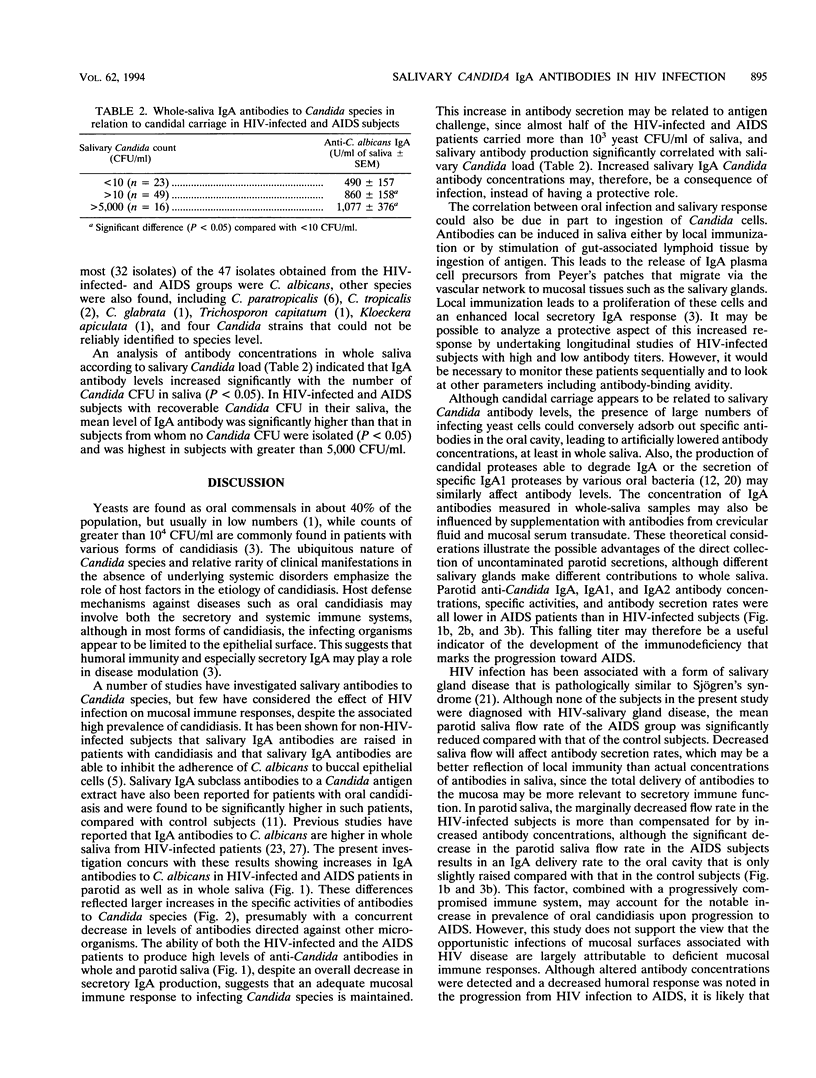
Human immunodeficiency virus (HIV)-infected individuals are predisposed to recurrent oral candidiasis, and, although it has been assumed that this is because of deficient mucosal immune responses, this has not been properly established. The present study aimed to compare the concentrations and secretion rates of immunoglobulin A (IgA) and IgA subclass antibodies to Candida albicans in whole and parotid saliva samples from HIV-infected patients, AIDS patients, and control subjects. Levels of IgA antibody to Candida species in whole saliva were higher in the HIV group than in the controls and were highest in the AIDS group (P < 0.05). In parotid saliva, the mean antibody levels were significantly greater in HIV-positive patients than in controls (P < 0.05) but fell to lower levels in the AIDS group. The secretion rates of Candida antibodies in parotid saliva were reduced in AIDS patients compared with HIV patients. The specific activities of the IgA antibodies and both subclasses were significantly higher in the HIV and AIDS patients than in the controls in both whole and parotid saliva (P < 0.05). Antibody levels were significantly correlated with the numbers of Candida organisms isolated from saliva (P < 0.05). These results suggest clear differences in salivary antibody profiles among HIV-infected. AIDS, and control subjects and are indicative of a response to antigenic challenge by infecting Candida species. No obvious defect in the mucosal immune response in the HIV or AIDS groups that might account for the increased prevalence of candidiasis was apparent.
Full text
PDF

Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Arendorf T. M., Walker D. M. The prevalence and intra-oral distribution of Candida albicans in man. Arch Oral Biol. 1980;25(1):1–10. doi: 10.1016/0003-9969(80)90147-8. [DOI] [PubMed] [Google Scholar]
- Delacroix D. L., Dive C., Rambaud J. C., Vaerman J. P. IgA subclasses in various secretions and in serum. Immunology. 1982 Oct;47(2):383–385. [PMC free article] [PubMed] [Google Scholar]
- Epstein J. B., Kimura L. H., Menard T. W., Truelove E. L., Pearsall N. N. Effects of specific antibodies on the interaction between the fungus Candida albicans and human oral mucosa. Arch Oral Biol. 1982;27(6):469–474. doi: 10.1016/0003-9969(82)90086-3. [DOI] [PubMed] [Google Scholar]
- Fubara E. S., Freter R. Protection against enteric bacterial infection by secretory IgA antibodies. J Immunol. 1973 Aug;111(2):395–403. [PubMed] [Google Scholar]
- Gelderblom H. R. Assembly and morphology of HIV: potential effect of structure on viral function. AIDS. 1991 Jun;5(6):617–637. [PubMed] [Google Scholar]
- Gough P. M., Warnock D. W., Richardson M. D., Mansell N. J., King J. M. IgA and IgG antibodies to Candida albicans in the genital tract secretions of women with or without vaginal candidosis. Sabouraudia. 1984;22(4):265–271. [PubMed] [Google Scholar]
- Grey H. M., Abel C. A., Yount W. J., Kunkel H. G. A subclass of human gamma-A-globulins (gamma-A2) which lacks the disulfied bonds linking heavy and light chains. J Exp Med. 1968 Dec 1;128(6):1223–1236. doi: 10.1084/jem.128.6.1223. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jeganathan S., Ufomata D., Hobkirk J. A., Ivanyi L. Immunoglobulin A1 and A2 subclass of salivary antibodies to Candida albicans in patients with oral candidosis. Clin Exp Immunol. 1987 Nov;70(2):316–321. [PMC free article] [PubMed] [Google Scholar]
- Kilian M., Mestecky J., Russell M. W. Defense mechanisms involving Fc-dependent functions of immunoglobulin A and their subversion by bacterial immunoglobulin A proteases. Microbiol Rev. 1988 Jun;52(2):296–303. doi: 10.1128/mr.52.2.296-303.1988. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Korting H. C., Ollert M., Georgii A., Fröschl M. In vitro susceptibilities and biotypes of Candida albicans isolates from the oral cavities of patients infected with human immunodeficiency virus. J Clin Microbiol. 1988 Dec;26(12):2626–2631. doi: 10.1128/jcm.26.12.2626-2631.1988. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ladjeva I., Peterman J. H., Mestecky J. IgA subclasses of human colostral antibodies specific for microbial and food antigens. Clin Exp Immunol. 1989 Oct;78(1):85–90. [PMC free article] [PubMed] [Google Scholar]
- Langford-Kuntz A. A., Rüchel R., Reichart P. A. Orale Manifestationen der Candidiasis bei HIV-Infektion. Klinische und mikrobiologische Untersuchungen. Dtsch Z Mund Kiefer Gesichtschir. 1988 Jan-Feb;12(1):28–35. [PubMed] [Google Scholar]
- McGhee J. R., Mestecky J., Elson C. O., Kiyono H. Regulation of IgA synthesis and immune response by T cells and interleukins. J Clin Immunol. 1989 May;9(3):175–199. doi: 10.1007/BF00916814. [DOI] [PubMed] [Google Scholar]
- Müller F., Frøland S. S., Hvatum M., Radl J., Brandtzaeg P. Both IgA subclasses are reduced in parotid saliva from patients with AIDS. Clin Exp Immunol. 1991 Feb;83(2):203–209. doi: 10.1111/j.1365-2249.1991.tb05615.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Phelan J. A., Saltzman B. R., Friedland G. H., Klein R. S. Oral findings in patients with acquired immunodeficiency syndrome. Oral Surg Oral Med Oral Pathol. 1987 Jul;64(1):50–56. doi: 10.1016/0030-4220(87)90116-2. [DOI] [PubMed] [Google Scholar]
- Reinholdt J., Krogh P., Holmstrup P. Degradation of IgA1, IgA2, and S-IgA by Candida and Torulopsis species. Acta Pathol Microbiol Immunol Scand C. 1987 Dec;95(6):265–274. doi: 10.1111/j.1699-0463.1987.tb00040.x. [DOI] [PubMed] [Google Scholar]
- Schiødt M. HIV-associated salivary gland disease: a review. Oral Surg Oral Med Oral Pathol. 1992 Feb;73(2):164–167. doi: 10.1016/0030-4220(92)90189-w. [DOI] [PubMed] [Google Scholar]
- Svanborg-Edén C., Svennerholm A. M. Secretory immunoglobulin A and G antibodies prevent adhesion of Escherichia coli to human urinary tract epithelial cells. Infect Immun. 1978 Dec;22(3):790–797. doi: 10.1128/iai.22.3.790-797.1978. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tylenda C. A., Larsen J., Yeh C. K., Lane H. C., Fox P. C. High levels of oral yeasts in early HIV-1 infection. J Oral Pathol Med. 1989 Oct;18(9):520–524. doi: 10.1111/j.1600-0714.1989.tb01355.x. [DOI] [PubMed] [Google Scholar]
- Vudhichamnong K., Walker D. M., Ryley H. C. The effect of secretory immunoglobulin A on the in-vitro adherence of the yeast Candida albicans to human oral epithelial cells. Arch Oral Biol. 1982;27(8):617–621. doi: 10.1016/0003-9969(82)90184-4. [DOI] [PubMed] [Google Scholar]
- Walker W. A., Wu M., Isselbacher K. J., Bloch K. J. Intestinal uptake of macromolecules. III. Studies on the mechanism by which immunization interferes with antigen uptake. J Immunol. 1975 Sep;115(3):854–861. [PubMed] [Google Scholar]
- Williams R. C., Gibbons R. J. Inhibition of bacterial adherence by secretory immunoglobulin A: a mechanism of antigen disposal. Science. 1972 Aug 25;177(4050):697–699. doi: 10.1126/science.177.4050.697. [DOI] [PubMed] [Google Scholar]
- Wray D., Felix D. H., Cumming C. G. Alteration of humoral responses to Candida in HIV infection. Br Dent J. 1990 Apr 21;168(8):326–329. doi: 10.1038/sj.bdj.4807186. [DOI] [PubMed] [Google Scholar]