

[Four of the authors respond:]
We thank Jean-Pierre Dery and Robert DeLarochellière for their comments. Although only 8% of patients who underwent primary percutaneous coronary intervention after interhospital transfer were treated within the recommended time in our study, 36% of those treated on site received therapy within the recommended time.1 Therefore, at least in this latter group, the time to primary percutaneous coronary intervention exceeded recommendations in many (but not most) patients.
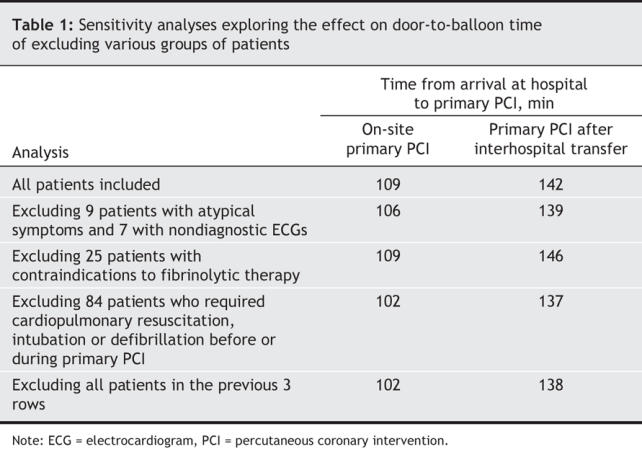
To address Dery and DeLarochellière's concerns that inclusion of particular groups of patients may increase time delays to primary percutaneous coronary intervention, we undertook sensitivity analyses in which we excluded the following groups: patients who present with atypical symptoms (e.g., patients who may have aortic dissection and pulmonary embolism), patients with initial electrocardiograms that are nondiagnostic, patients with contraindications to fibrinolytic therapy and patients who required intubation and cardiopulmonary resuscitation for stabilization. The time to primary percutaneous coronary intervention remained prolonged even after exclusion of these patients (Table 1).
Table 1
Dery and DeLarochellière were also concerned that we may have included patients who underwent rescue percutaneous coronary intervention. As the objective of our study was to measure time delays to initial reperfusion therapy (i.e., primary percutaneous coronary intervention and fibrinolytic therapy), we did not include patients who underwent rescue percutaneous coronary intervention. Only patients who underwent primary percutaneous coronary intervention without prior administration of fibrinolytic therapy were retained for analysis.
Door-to-open-artery time is difficult to determine accurately, because the exact time when the artery opens is often unknown. This measure is relevant mainly for patients who already have an open artery before any coronary intervention (20% of the patients in our study). In these patients, the median door-to-open-artery time was 113 min (first and third quartile 76, 168) and 149 min (first and third quartile 107, 270) among those who underwent primary percutaneous coronary intervention on site and after interhospital transfer, respectively. These times were similar to the door-to-balloon times that we reported in our study.
Footnotes
Competing interests: Dr. Huynh has received travel assistance from Hoffmann-La Roche Pharma Canada.
REFERENCE
- 1.Huynh T, O'Loughlin J, Joseph L, et al; AMI-QUEBEC Study Investigators. Delays to reperfusion therapy in acute ST-segment elevation myocardial infarction: results from the AMI-QUEBEC Study. CMAJ 2006;175(12):1527-32. [DOI] [PMC free article] [PubMed]