

Abstract
Isolated inferior division oculomotor nerve palsy (ONP) is rare. Acquired cases have been associated with neurologic or systemic disease. To our knowledge, congenital inferior division ONP is previously unreported. We present a case of congenital inferior division ONP in which magnetic resonance imaging demonstrated the structural neuropathy.
A 21-year-old woman presented with lifelong large-angle exotropia and diminished vision acuity in her right eye (OD). She denied diplopia, periocular pain, cephalgia, migraine, head trauma, or prior surgery. Birth history was unremarkable. She had no history of diabetes mellitus, hypertension, systemic vasculopathy, or thyroid disease. She has three unaffected brothers and four unaffected sisters. General physical and neurologic examinations were normal. Cranial nerves were normal except for ocular motility. Cycloplegic refraction was + 4.00 + 2.75 × 150 OD and + 0.50 + 0.50 × 90 left eye (OS). Corrected visual acuity was 20/80 OD and 20/25 OS. Ptosis was absent. Both pupils were 7 mm in diameter with slight peaking toward 9:00 OD and were normally reactive to light and accommodation. The ocular versions are shown in Figure 1. At near with correction, there was 100Δ exotropia with 10Δ right hypertropia. Head tilt did not appreciably alter the hypertropia, but dissociated vertical deviation was present bilaterally. Abducting and vertical saccades were normal for both eyes (OU ), while adducting saccades were bilaterally slow. Convergence was absent. There was bilateral optic disk pallor with cup-to-disk ratio of 0.5 OD and 0.3 OS. There was incyclotorsion OU on fundus examination.
FIG 1.

Ocular versions in congenital inferior division oculomotor palsy. In primary position there was 75Δ exotropia and 6Δ right hypertropia. The deviation was horizontally comitant, but diminished to 65Δ in upward gaze and increased to 95Δ in downward gaze. The right eye had marked limitation to adduction and infraduction. There was mild-to-moderate limitation to adduction and infraduction of the left eye.
High-resolution magnetic resonance imaging (MRI) performed with orbital surface coils identified a smaller inferior division of the oculomotor nerve (OMN) OD than OS, with no identifiable motor nerve to the right medial (MR) and inferior rectus (IR) muscles, both of whose deep portions exhibited marked atrophy and abnormal internal bright signal on T1 imaging (Figure 2). The abducens nerve was readily demonstrable OU. The inferior oblique muscle was present bilaterally, but both lateral rectus muscle paths were superiorly displaced relative to the MR muscles (Figure 2). Just posterior to the globe, right and left optic nerve diameters were 3.07 and 3.05 mm, respectively (Figure 2), both subnormal compared with published values.1 Imaging with a head coil demonstrated bilateral OMN hypoplasia in the skull base region, with the right OMN too small to resolve in any of the 1 mm thickness contiguous image planes obtained in the plane of its path (Figure 3). These anatomic findings indicate bilateral but asymmetrical OMN abnormality.
FIG 2.
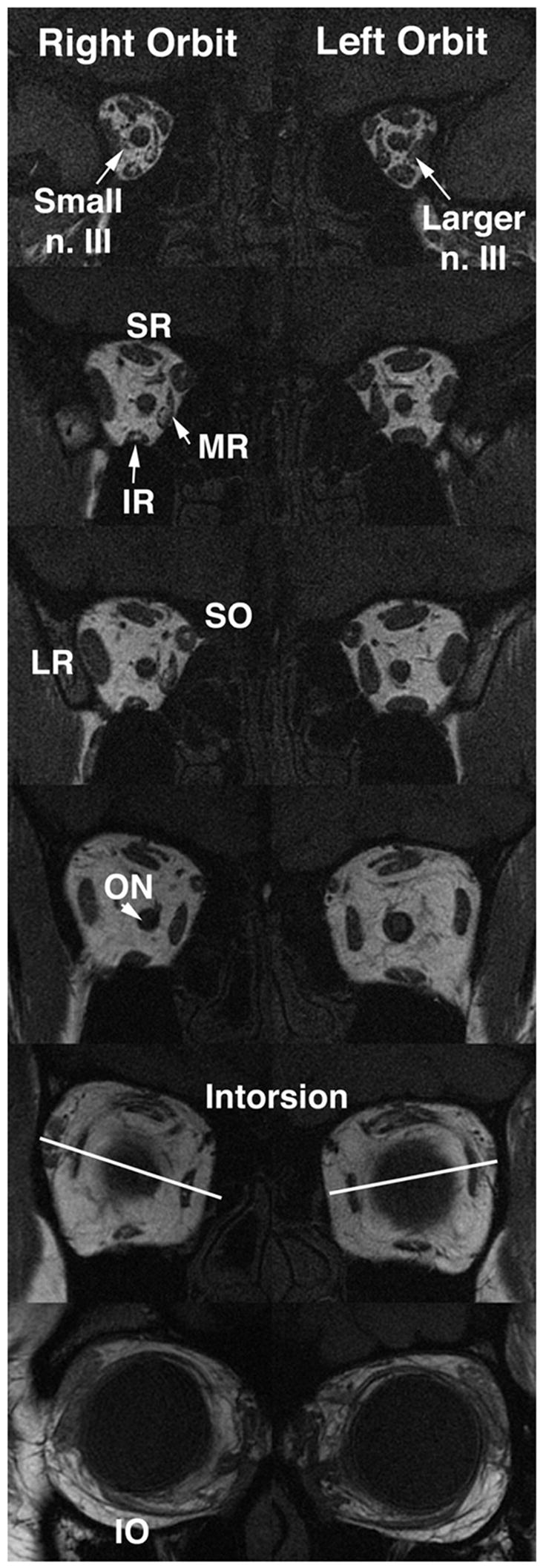
High-resolution, T1-weighted magnetic resonance imaging (MRI) in 2 mm thickness quasi-coronal image planes perpendicular to the long axis of both orbits, arranged from posterior to anterior. Ordinarily the oculomotor nerve is easily evident in these views. The right oculomotor nerve is smaller, but the inferior division to the right medial and inferior rectus (IR) muscles cannot be visualized. There is deep atrophy of the IR and medial rectus (MR) muscles. The right optic nerve is smaller. There is superior heterotopia of lateral rectus (LR) pulley resulting in more incyclotorsion in the right eye (OD). n. III, oculomotor nerve; SR, superior rectus muscle; SO, superior oblique muscle; IO, IO muscle; ON, optic nerve.
FIG 3.
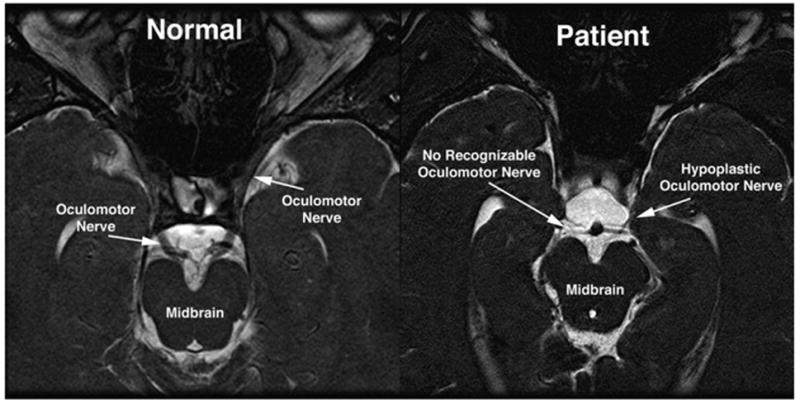
High-resolution, heavily T2-weighted MRI in a 1 mm thickness plane paralleling the anterior optic pathway demonstrates no recognizable right oculomotor nerve exiting the midbrain, compared with the obvious oculomotor nerves in the normal midbrain image. The left oculomotor nerve was markedly hypoplastic.
Discussion
The OMN divides into superior and inferior divisions just before entering the superior orbital fissure. Classical signs of inferior division OMP were evident here, including large exotropia, hypertropia, incyclotropia, and discoria. Although pupillary light responses were spared, Good and coworkers have postulated that early embryologic damage could partially spare the Edinger–Westphal nucleus.2
Causes of acquired inferior division ONP include local orbital disease, trauma, vascular abnormality, tumor, and infarction in the cavernous sinus or midbrain.3–5 Occasional cases have been associated with vasculitis, demyelination, or viral infection.6,7 The oculomotor nuclear complex consists of one unpaired subnucleus and four paired subnuclei.4 Selective divisional OMP has been reported due to intrinsic brainstem disease,8 while isolated IR palsy has been associated with metastasis to the oculomotor nucleus.5 Takano and Aoki reported a case of dorsal–lateral oculomotor subnucleus infarction presenting with isolated IR palsy.4
The present report is a novel one of congenital inferior division OMP, presumably due to congenital cranial dysinnervation in the midbrain, suggesting that this disorder lies in the spectrum of the congenital cranial dysinnervation disorders, primarily involving motor neurons or their axon projections.9 High-resolution MRI of the midbrain and deep orbit can document the neuromuscular lesion in OMP.3,10
Footnotes
This work was supported by USPHS NIH EY08313 and Research to Prevent Blindness.
The authors hold no proprietary interest in this work.
References
- 1.Karim S, Clark RA, Poukens V, Demer JL. Demonstration of systematic variation in human intraorbital optic nerve size by quantitative magnetic resonance imaging and histology. Invest Ophthalmol Vis Sci. 2004;45:1047–51. doi: 10.1167/iovs.03-1246. [DOI] [PubMed] [Google Scholar]
- 2.Good WV, Barkovich AJ, Nickel BL, Hoyt CS. Bilateral congenital oculomotor nerve palsy in a child with brain anomalies. Am J Ophthalmol. 1991;111:555–8. doi: 10.1016/s0002-9394(14)73697-9. [DOI] [PubMed] [Google Scholar]
- 3.Nagata E, Tanahashi N, Koto A, Fukuuchi Y, Kayama H. A case of spontaneous arteriovenous fistula presenting as the partial oculomotor nerve palsy. Rinsho Shinkeigaku. 1995;35:808–10. [PubMed] [Google Scholar]
- 4.Takano M, Aoki K. Midbrain infarction presenting isolated inferior rectus nuclear palsy. Rinsho Shinkeigaka. 2000;40:832–5. [PubMed] [Google Scholar]
- 5.Chou TM, Demer JL. Isolated inferior rectus palsy caused by a metastasis to the oculomotor nucleus. Am J Ophthalmol. 1998;126:737–40. doi: 10.1016/s0002-9394(98)00139-1. [DOI] [PubMed] [Google Scholar]
- 6.Cunningham ET, Jr, Good WV. Inferior branch oculomotor nerve palsy. A case report J Neuroophthalmol. 1994;14:21–3. [PubMed] [Google Scholar]
- 7.Matsuda A, Chin S, Ohashi T. Two cases of inferior branch palsy of the oculomotor nerve in children. Nippon Ganka Gakkai Zasshi. 1995;99:861–5. [PubMed] [Google Scholar]
- 8.Ksiazek SM, Repka MX, Maguire A, Harbour RC, Savino PJ, Miller NR, et al. Divisional oculomotor nerve paresis caused by intrinsic brainstem disease. Ann Neurol. 1989;26:714–8. doi: 10.1002/ana.410260605. [DOI] [PubMed] [Google Scholar]
- 9.Gutowski NJ, Bosley TM, Engle EC. 110th ENMC International workshop: the congenital cranial dysinnervation disorders (CCDDs). Naarden, The Netherlands, 25–27 October, 2002. Neuromuscul Disord. 2003;13:573–8. doi: 10.1016/s0960-8966(03)00043-9. [DOI] [PubMed] [Google Scholar]
- 10.Demer JL, Clark RA, Kono R, Wright W, Velez F, Rosenbaum AL. A 12-year, prospective study of extraocular muscle imaging in complex strabismus. J AAPOS. 2002;6:337–47. doi: 10.1067/mpa.2002.129040. [DOI] [PubMed] [Google Scholar]