

The case: A 56-year-old woman presents to her family physician with a 7-day history of tenderness, swelling and redness of 2 metacarpophalangeal joints and 1 proximal interphalangeal joint in her right hand. She also reports pain and redness of her right knee that makes it difficult to walk. On examination, her right knee appears swollen and red. The patient has a 10-year history of rheumatoid arthritis with intermittent polyarticular flares, primarily involving her wrists, fingers (metacarpophalangeal and proximal interphalangeal joints), feet (metatarsophalangeal joints) and occasionally her knees. However, the condition has been well managed with methotrexate and hydroxychloroquine therapy. She had no flares in the year before presentation and is able to perform household chores and to work as a dry-cleaning attendant. What other history, physical examination and laboratory investigations would you seek to distinguish a simple flare of inflammatory polyarthritis from a superimposed infection?
Septic arthritis can be difficult to diagnosis, especially when it is mistaken for a flare of pre-existing inflammatory arthritis. Because rheumatoid arthritis is the most common type of inflammatory arthritis, occurring in about 1% of the population,1 we chose to use it as an example of inflammatory arthritis in this review of nongonococcal septic arthritis. Septic arthritis in patients with rheumatoid arthritis was initially described by Bywaters2 and by Kellgren and colleagues.3 The case described by Bywaters was fistulous rheumatism. Since these initial reports, hundreds of cases of septic arthritis have been documented in patients with chronic arthritis.4 The risk factors for septic arthritis in patients with rheumatoid arthritis are described in Box 1. Infection as the cause of joint inflammation must be diagnosed quickly because, if left undetected, it can lead to rapid joint destruction. Urgent aspiration of the affected joints is required, followed by antibiotic therapy.
Box 1.
The annual incidence of septic arthritis in the general population is 2 to 5 per 100 000.5 Patients with inflammatory arthritis are predisposed to septic arthritis. Indeed, a study in England reported that 46% of patients with bacterial arthritis had a pre-existing joint disease.6 Of these patients, 14% had rheumatoid arthritis and less than 10% had other forms of inflammatory arthritis. A separate study reported that patients with pre-existing rheumatoid arthritis were at an increased risk of septic arthritis (odds ratio 4.0, 95% confidence interval 1.9–8.3).5 The incidence of septic arthritis among patients with pre-existing inflammatory arthritis has not been well studied, with an estimated annual incidence of 28 to 38 per 100 000,5and a prevalence of 0.3% to 3%.7 One study suggested the annual frequency of septic arthritis to be 0.2% among patients with rheumatoid arthritis.8
Pathophysiology
Invasion of bacteria into the synovial space can occur predominantly by 2 routes: hematogenous spread (most common) or direct invasion.12,13 The synovium is extremely vascular and contains no limiting basement membrane: thus, there is easy access to the synovial space. Bacteria may spread directly from adjacent osteomyelitis or from a local soft-tissue infection, diagnostic or therapeutic procedure, or penetrating trauma (Fig. 1). Within 24–48 hours of bacterial invasion, dramatic infiltration by neutrophils, vascular congestion and proliferation of cells lining the joint space become evident [based on animal studies].12 During the week following bacterial invasion, persistent purulent effusion, marked synovial proliferation, infiltration by mononuclear cells, and granulation tissue and abscesses develop. Eventually, cytokine-induced proteolytic enzymes are released, which leads to cartilage and bone destruction in as little as 10 days.12 The end result is joint destruction and systemic sepsis.

Fig. 1: Routes of bacterial invasion into a joint. Adapted from Lidgren.13. Photo by: Lianne Friesen and Nicholas Woolridge
Patients with rheumatoid arthritis have reduced phagocytic function that may predispose them to septic arthritis.14–16 Although the most common pathogens that cause septic arthritis are members of the gram-positive Staphylococcus and Streptococcus genus, gram-negative bacteria infections occur in about 30% of cases. Other organisms, such as anaerobes and fungi, may also cause septic arthritis. Bacteria, especially staphylococci, may colonize prosthetic joint surfaces.17 The virulence factors of the different types of microbial pathogens, impaired host immunity and the presence of prosthetic joints all act to increase the difficulty of eradicating the infection.
Diagnosis
The classic presentation of septic arthritis is a single, acutely hot, swollen and painful joint (in 80%–90% of cases);18 however, patients with inflammatory arthritis may not present classically. A polyarticular pattern may be seen in 10%–20% of cases. The knee joint is involved in about 50% of cases. Associated clinical features include an extra-articular site of infection, reduced joint function, toxic appearance and fever. A history of injection drug use, an immunocompromised state, recent surgery or the presence of indwelling catheters may increase the likelihood of septic arthritis.18
Septic arthritis should be considered if a patient with rheumatoid arthritis has a flare of joint inflammation, with either a monoarticular or a polyarticular distribution. Although the knee is most commonly affected, other large and medium joints can also be affected.6,8,18 Fluid from the joint should be aspirated if the flare is more severe than usual, if there is a significant loss of joint function (e.g., the patient requires crutches), if the joint is red, or if the patient has systemic symptoms (e.g., fever, night sweats). The presentation may be more subtle in patients who are taking glucocorticoids, disease-modifying antirheumatic drugs or biologic agents.
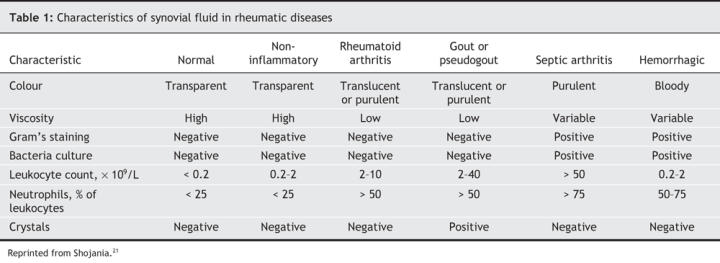
It is essential that the aspirated fluid be sent for microbial examination (e.g., Gram's staining, culture, cell count) before initiation of therapy.19 Accurate identification of the pathogen becomes more challenging if fluid is aspirated after empiric antibiotic therapy is started. Identification of the pathogen may be aided by simultaneous blood culture and by culture of other potential sites of infection.20,21 The leukocyte count (from synovial fluid) is considered elevated if it is greater than 20 × 109/L, and markedly elevated if it is greater than 50 × 109/L (Table 1).18,22 If septic arthritis is suspected, a negative result of Gram's staining should not delay the start of empiric antibiotic therapy. If the initial bacterial culture is negative, a biopsy may be considered to test for slower growing organisms such as mycobacteria or fungi. In the future, polymerase chain reaction may aid in early diagnosis. An elevated peripheral leukocyte count and elevated levels of inflammatory markers (e.g., erythrocyte sedimentation rate, C-reactive protein) may also be supportive, but not diagnostic, of septic arthritis.6,23
Table 1
Radiologic investigations such as bone and gallium scans are often not helpful at the onset in distinguishing between infectious arthritis and inflammatory arthritis in patients with underlying inflammatory arthritis. Radiologically guided aspiration may be required for technically difficult joints, such as the hip or sacroiliac joints.
Treatment
The goal of treatment is to rapidly eradicate the infection and to protect the joint. Ideally, the choice of treatment is based on the result of the Gram's staining.24 If the initial result shows that gram-positive organisms are present, cefazolin (for community-acquired infections) or vancomycin (for nosocomial infections) should be used. However, if Gram's staining shows gram-negative bacteria, a third-generation cephalosporin should be used. If there is suspicion of Pseudomonas infection (e.g., in injection drug users), double coverage with ceftazidime and gentamicin is warranted. If Gram's staining does not show bacteria yet septic arthritis is still suspected, the patient should be given cefazolin and gentamicin while waiting for the results of the cultures. The duration of therapy is generally prolonged. Parenteral therapy for 2–6 weeks followed by oral therapy is common.7 Longer courses of therapy are required for the treatment of complications, such as adjacent osteomyelitis, or causitive etiologies, such as infective endocarditis.18 Shorter courses may be considered for infections by organisms that are susceptible in vitro to orally administered agents with high bioavailability (e.g., fluoroquinolones).
It is important to remove as much of the infected fluid as possible from the joint. Depending on the location, fluid can be removed by repeated needle aspiration (e.g., knee), or by arthroscopic or open drainage of the joint. There have been no randomized controlled trials comparing the different forms of drainage; however, most joint infections can be managed by repeated needle aspiration. Arthroscopy and open arthrotomy should be considered when there is adjacent osteomyelitis, or when initial aspiration is unsuccessful or incomplete (e.g., loculated effusions).24
Limited mobilization with range-of-movement exercises is indicated when antibiotic therapy is started. After the inflammation has been reduced, more active physical therapy can be started.24
Alteration of risk factors for septic arthritis is an important consideration. This may include treatment of comorbidities such as diabetes and the management of coexisting infections. The removal of joint prostheses should strongly be considered, as should discontinuation of immunosuppressant therapy (particularly newer biologics).13
Case revisited
Additional medical history was obtained, and the patient was examined fully. The patient denied factors that might predispose her to septic arthritis, including intravenous drug use, or adjacent skin trauma or infection. She also denied having other sites of infection or skin ulceration. The patient was not diabetic, nor did she have any prosthetic joints, urinary catheters or recent surgeries. She was not taking glucocorticoids or biologic agents. Apart from her musculoskeletal symptoms, she had felt vaguely unwell the week before presentation and felt that she was getting “worse.” The patient reported having intermittent night sweats. On presentation she was afebrile and normotensive but had tachycardia (102 beats/min). Findings on physical examination, including examination of the cardiopulmonary and dermatologic systems, were unremarkable. The patient's right knee joint was the most inflamed; the aspirated fluid was cloudy and yellow, with a leukocyte count of 86 × 109/L. The results of Gram's staining showed clusters of gram-positive cocci that were later identified as Staphylococcus aureus. The patient was admitted to hospital, and intravenous cefazolin therapy was started. Fluid was removed from the knee by needle aspiration daily for the first few days and less frequently as the effusion settled.
Key learning points
Diagnosis and treatment
• Consider septic arthritis in any patient with inflammatory arthritis who presents with a joint flare, particularly if one joint has flared more often than others
• Fluid should be aspirated if the flare is more severe than usual, if there is a substantial loss of joint function, if the joint is red or if the patient has systemic symptoms
• Aspiration is the most important part of both diagnosis and management
• Initiate empiric antibiotic therapy after aspiration, and narrow antimicrobial coverage once microbiology results are known
Consequences
• If septic arthritis is untreated, cartilage and bone destruction occurs in as little as 10 days. The end result is joint destruction and systemic sepsis
Acknowledgments
We thank Farzana R. Kherani for assistance with editing, and Drs. Barry E. Koehler and Robert Reynolds for reviewing this manuscript.
Footnotes
This article has been peer reviewed.
Contributors: Both authors contributed substantially to the conception and design. Raheem Kherani wrote the first draft of the article. Both authors revised the article critically for important intellectual content and gave final approval of the version to be published.
Competing interests: None declared.
Correspondence to: Dr. Raheem B. Kherani, Richmond Rheumatology, Suite 230, 6091 Gilbert Rd., Richmond, BC, V7C 5L9; kherani@ualberta.net
REFERENCES
- 1.Lawrence RC, Helmick CG, Arnett FC, et al. Estimates of the prevalence of arthritis and selected musculoskeletal disorders in the United States. Arthritis Rheum 1998;41:778-99. [DOI] [PubMed]
- 2.Bywaters EG. Fistulous rheumatism; a manifestation of rheumatoid arthritis. Ann Rheum Dis 1953;12:114-21. [DOI] [PMC free article] [PubMed]
- 3.Kellgren JH, Ball J, Fairbrother RW, et al. Suppurative arthritis complicating rheumatoid arthritis. BMJ 1958;1:1193-9. [DOI] [PMC free article] [PubMed]
- 4.Epstein JH, Zimmerman B, Ho G. Polyarticular septic arthritis. J Rheumatol 1986;13:1105-7. [PubMed]
- 5.Kaandorp CJ, Van Schaardenburg D, Krijnen P, et al. Risk factors for septic arthritis in patients with joint disease. A prospective study. Arthritis Rheum 1995;38:1819- 25. [DOI] [PubMed]
- 6.Cooper C, Cawley MI. Bacterial arthritis in an English health district: a 10 year review. Ann Rheum Dis 1986;45:458-63. [DOI] [PMC free article] [PubMed]
- 7.Goldenberg DL. Infectious arthritis complicating rheumatoid arthritis and other chronic rheumatic disorders. Arthritis Rheum 1989;32:496-502. [DOI] [PubMed]
- 8.Ostensson A, Geborek P. Septic arthritis as a non-surgical complication in rheumatoid arthritis: relation to disease severity and therapy. Br J Rheumatol 1991;30:35-8. [DOI] [PubMed]
- 9.Baum J. Infection in rheumatoid arthritis. Arthritis Rheum 1971;14:135-7. [DOI] [PubMed]
- 10.Jackson MS, Bagg J, Gupta MN, et al. Oral carriage of staphylococci in patients with rheumatoid arthritis. Rheumatology (Oxford) 1999;38:572-5. [DOI] [PubMed]
- 11.Giles JT, Bartlett SJ, Gelber AC, et al. Tumor necrosis factor inhibitor therapy and risk of serious postoperative orthopedic infection in rheumatoid arthritis. Arthritis Care Res 2006;55:333-7. [DOI] [PubMed]
- 12.Goldenberg DL, Reed JI. Bacterial arthritis. N Engl J Med 1985;312:764-71. [DOI] [PubMed]
- 13.Lidgren L. Septic arthritis and osteomyelitis. In: Hochberg MC, Silman AJ, Smolen JS, et al., editors. Rheumatology. Toronto: Mosby; 2003. p. 1055-66.
- 14.Dolganiuc A, Stavaru C, Anghel M, et al. The migratory and phagocytic activity of polymorphonuclear leukocytes in rheumatoid arthritis and osteoarthritis patients. Roum Arch Microbiol Immunol 2000;59:43-53. [PubMed]
- 15.Nada R, Datta U, Deodhar SD, et al. Neutrophil functions in rheumatoid arthritis. Indian J Pathol Microbiol 1999;42:283-9. [PubMed]
- 16.Turner RA, Schumacher R, Myers AR. Phagocytic function of polymorphonuclear leukocytes in rheumatic diseases. J Clin Invest 1973;52:1632-5. [DOI] [PMC free article] [PubMed]
- 17.Lew DP, Waldvogel FA. Osteomyelitis. Lancet 2004;364:369-79. [DOI] [PubMed]
- 18.Garcia-De La Torre I. Advances in the management of septic arthritis. Rheum Dis Clin North Am 2003;29:61-75. [DOI] [PubMed]
- 19.Margaretten ME, Kohlwes J, Moore D, et al. Does this adult patient have septic arthritis? JAMA. 2007;297:1478-88. [DOI] [PubMed]
- 20.Dubost JJ, Fis I, Denis P, et al. Polyarticular septic arthritis. Medicine (Baltimore) 1993;72:296-310. [DOI] [PubMed]
- 21.Gelman MI, Ward JR. Septic arthritis: a complication of rheumatoid arthritis. Radiology 1977;122:17-23. [DOI] [PubMed]
- 22.Shojania K. Rheumatology: 2. What laboratory tests are needed? CMAJ 2000;162:1157- 63. [PMC free article] [PubMed]
- 23.Levine MJ, McGuire KJ, McGowan KL, et al. Assessment of the test characteristics of C-reactive protein for septic arthritis in children. J Pediatr Orthop 2003;23:373-7. [PubMed]
- 24.Hasan S, Smith JW. Septic arthritis. Curr Treat Options Infect Dis 2001;3:279-86.