

Abstract
Background
Health warnings on cigarette packages provide smokers with universal access to information on the risks of smoking. However, warnings vary considerably among countries, ranging from graphic depictions of disease on Canadian packages to obscure text warnings in the U.S. The current study examined the effectiveness of health warnings on cigarette packages in four countries.
Methods
Quasi-experimental design. Telephone surveys were conducted with representative cohorts of adult smokers (N= 14,975): Canada (n =3687); the U.S. (n =4273); the UK (n= 3634); and Australia (n =3381). Surveys were conducted between 2002 and 2005, before and at three time points following new warnings on UK packages.
Results
. At Wave 1, Canadian smokers reported the highest levels of awareness and impact for health warnings among the four countries, followed by Australian smokers. Following the implementation of new UK warnings at Wave 2, UK smokers reported greater levels of awareness and impact, although Canadian smokers continued to report higher levels of impact after adjusting for the implementation date. U.S. smokers reported the lowest levels of effectiveness for almost every measure recorded at each survey wave.
Conclusions
Large, comprehensive warnings on cigarette packages are more likely to be noticed and rated as effective by smokers. Changes in health warnings are also associated with increased effectiveness. Health warnings on U.S. packages, which were last updated in 1984, were associated with the least effectiveness.
INTRODUCTION
Tobacco use remains the second leading cause of death in the world.1,2 Accordingly, cigarette packages in almost every jurisdiction in the world carry health warnings to inform consumers about the risks of smoking. Health warnings on packages are appealing both because of their low cost to regulators and their unparalleled reach among smokers. However, the effectiveness of package warnings depends on their size, position, and design: whereas obscure warnings have been shown to have relatively little impact, more comprehensive warnings, including picture-based warnings, have been associated with greater recall, increased motivation to quit smoking, and greater attempts to quit.4–14 Previous research also indicates that health warnings are subject to “wear-out”, such that newly implemented warnings are most likely to be noticed and rated as effective by smokers.15–18
In recognition of the health and economic burden from tobacco use, more than 135 countries have ratified the Framework Convention on Tobacco Control (FCTC)—the first international treaty devoted to public health.3 Countries that ratify the FCTC are required to implement health warnings on cigarette packages that cover at least 30 per cent of the surface and are “large, clear, visible, and legible”.3 Beyond these minimum requirements, the FCTC also recommends that warnings “should” cover 50 per cent or more of a package’s principle surfaces, and “may” be in the form of pictures.3
Although several countries, such as Canada, already meet the recommended international guidelines, health warnings in the majority of countries, including the United States, fall short of the minimum FCTC standards. Some jurisdictions, such as the European Union, have recently revised their labeling policies to meet the FCTC guidelines.19
The purpose of the current study was to evaluate the effectiveness of health warnings in four countries— the United States (U.S.), Canada, the United Kingdom (UK), and Australia—including the impact of new warnings implemented in the UK, which were enhanced in 2003 to meet the minimum FCTC standard. The “effectiveness” of graphic warnings can be measured in various ways, including: (1) measures of salience, such as noticing and reading the warnings; (2) changes in health knowledge and perceptions of risk; (3) intentions/motivation to quit; and (4) behavioral changes, including changes in consumption, attempts to quit, and successful cessation. Measures of salience have previously been shown to predict future cessation behavior in previous research11; however, each of these downstream outcomes, including changes in perceived risk and motivation to quit, is also mediated by individual factors, such as a smokers’ socioeconomic background, as well as environmental variables including other sources of health information and pro-tobacco marketing.18
The present study used data from the International Tobacco Control (ITC) Four Country Survey—a cohort survey of representative samples of adult smokers in the UK, Canada, the U.S., and Australia. Survey waves were conducted in each country approximately 2 months before the UK warnings were implemented, and at 6, 18, and 32 months after implementation. Figure 1 shows the health warnings in each of the four ITC countries over the course of the survey waves. At baseline, Canadian packages featured 16 graphic warnings covering half of the outside of packages, as well as additional health and cessation information on the inside of packages. Australian packages featured 6 text warnings covering 25% and 35% of the front and back of the package, respectively, whereas the 6 text warnings on UK packages covered only 6% of the package face. In the U.S., 4 warnings were printed on the side of packages. Thus, the current study evaluated warnings that were: (1) well below the minimum FCTC standard (U.S. and UK at baseline); (2) slightly below the FCTC minimum (Australian warnings), (3) enhanced to the FCTC standard (UK at follow-up), and (4) at the recommended FCTC standard (Canada).
Figure 1.

Health warnings in the ITC Four-Country Survey: 2002–2005
Note: the new UK warnings include one of two warnings on the front (“Smoking Kills” or “Smoking seriously harms you and others around you”), and one of 14 rotating warnings on the back of the package.
ITC, International Tobacco Control
METHODS
Sample
Respondents in the ITC Four Country Survey were 18 years or older, smoked more than 100 cigarettes in their life, and smoked at least once in the past 30 days at recruitment.
Procedure
The cohort was constructed from probability sampling methods with telephone numbers selected at random from the population of each country, within strata defined by geographic region and community size. Eligible households were identified by asking a household informant the number of adult smokers. The Next Birthday Method20 was used to select the respondent in households with more than one eligible adult smoker.
The surveys were conducted using Computer-Assisted Telephone Interviewing (CATI) software. In order to increase recruitment rates,21 participants were mailed compensation equivalent to US$10 prior to completing the main survey. All aspects of the interviewer training and calling protocol were standardized across countries.
The current analysis includes data from the first four waves of the ITC Four-Country Survey, a series of cohort surveys in Canada, Australia, the UK, and the U.S. Respondents in each country are surveyed annually using parallel survey protocols and measures. Respondents lost to attrition at each wave are “replenished” using the original sampling design. Figure 2 indicates the survey dates and sample sizes for each wave. A full description of the ITC methodology, including country-level AAPOR survey rates has been published elsewhere.22
Figure 2.
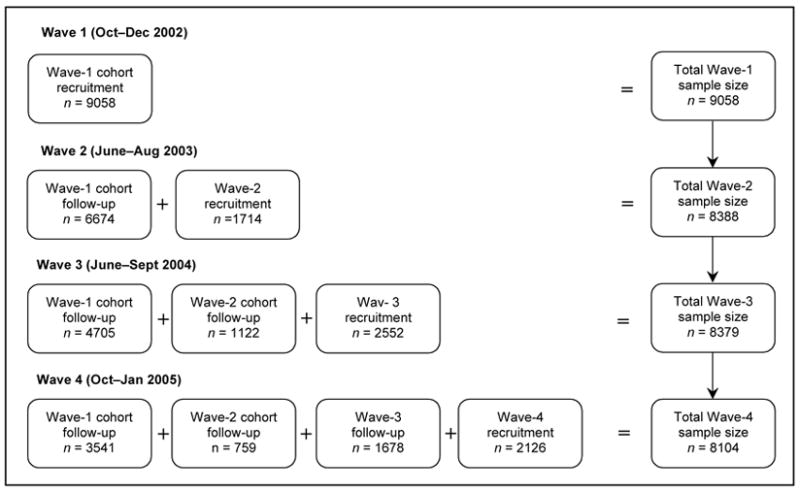
Sample size and follow-up rates for the ITC Four-Country Survey: Waves 1–4 ITC, International Tobacco Control
MEASURES
The survey was standardized across the four countries; respondents in each country were asked the same questions, with only minor variations for colloquial speech.
Demographics
Respondents were asked to report their age, gender, income, ethnicity, and education level. Comparable measures of education in each country were combined into three categories: “less than “secondary” school” / “some post-secondary training” / “post-secondary degree or higher”. Annual income was categorized into: “under £15,000 or $30,000” / “between £15,001 and £30,000” or “$30,001 and $59,999” / “above £30,000/$60,000”. In Canada, the U.S., and UK, minority status was defined in terms of being nonwhite. In three countries, minority status was defined in terms of being nonwhite; in Australia it was defined in terms of not speaking English at home, consistent with the census question in that country.
Smoking Behavior
Smoking behavior was assessed using standardized measures, including the Heaviness of Smoking Index, which combines cigarettes smoked per day and time to first cigarette (range =0–6).23 Recent quitting behavior was coded as a dichotomous variable (0=quit attempt in past year vs 1=no attempt). Intention to quit was coded as “no plans to quit” (0) or “plans to quit” (1). Respondents were also categorized as daily (0) or nondaily (1) smokers.
Exposure and Response to Product Warnings
Respondents were asked three questions about exposure to health warnings: (1) how often they had noticed the warning labels on cigarette packages in the past month, (2) whether they had read or looked closely at the warning labels in the past month, and (3) whether they had noticed advertising or information that talked about the dangers of smoking or encouraged quitting on cigarette packages. The first two measures of noticing and reading used a 5-point response scale ranging from “never” to “very often” whereas the third question was answered either yes or no.11
Respondents were also asked three questions designed to measure responses to product warnings. In each question, respondents were asked to what extent, if at all, the warning labels had: (1) stopped them from having a cigarette when they were about to smoke one, (2) made them think about the health risks of smoking, and (3) led them to think about quitting smoking.
All measures were assessed at each survey wave, except the Health Risks measure, which was not asked at Wave 1.
STATISTICAL ANALYSIS
SAS Version 9.1 (Research Triangle Institute, Research Triangle Park NC, 2004) was used for all statistical analyses. The current analysis included 14,975 unique respondents who provided complete information for at least one of the four waves. Generalized estimating equation (GEE) models were fitted to test the cross-sectional differences between countries, as well as any longitudinal changes within countries over the four survey waves. In order to control for the “novelty” effect of new warnings, GEE models were also conducted to compare responses from UK respondents at Wave 4 (approximately 2.5 years after new UK warnings were introduced in 2003) with data from Canadian respondents at Wave 1 (approximately 2.5 years after new Canadian warnings were introduced in 2000). All models were adjusted for gender, age, income, education, minority status, HSI, and any attempt to quit in the past year. All point estimates were weighted to reflect appropriate age–gender prevalence estimates within geographic strata, as well as to account for nonresponse and the survey design.22 All other analyses were conducted with both weighted and unweighted data. No significant differences were detected; unless otherwise noted, weighted data are presented. Given that each survey wave was conducted over a 3-month period in each country, preliminary analyses were conducted to identify any “survey date” effect. No association was found between the date the survey was completed and responses to any outcome of interest.
Note that tobacco manufacturers in the UK were required to begin printing the new warnings on all packages beginning in December 2002; however, for the purposes of the analyses, January 2003 has been identified as the implementation date given that packages with the new warnings did not begin appearing in retail outlets until this time.
RESULTS
Characteristics of Sample
Table 1 presents the demographic profile of the samples for each country.
Table 1.
Characteristics of adult smokers in the sample* (n =14,975)
| Characteristic | Canada
|
Australia
|
United Kingdom
|
United States
|
||||
|---|---|---|---|---|---|---|---|---|
| % | (n) | % | (n) | % | (n) | % | (n) | |
| Gender | ||||||||
| Females | 54.6 | (2012) | 52.7 | (1783) | 56.1 | (2038) | 56.2 | (2401) |
| Males | 45.4 | (1675) | 47.3 | (1598) | 43.9 | (1596) | 43.8 | (1872) |
| Age (years) | ||||||||
| 18–24 | 14.4 | (531) | 16.0 | (540) | 8.5 | (308) | 13.4 | (573) |
| 25–39 | 31.3 | (1155) | 36.2 | (1223) | 32.9 | (1194) | 29.1 | (1245) |
| 40–54 | 36.3 | (1337) | 33.5 | (1132) | 34.1 | (1241) | 35.2 | (1506) |
| 55+ | 18.0 | (664) | 14.4 | (486) | 24.5 | (891) | 22.2 | (949) |
| Education | ||||||||
| Low | 47.1 | (1738) | 65.7 | (2221) | 63.1 | (2293) | 44.3 | (1895) |
| Moderate | 39.1 | (1441) | 20.4 | (690) | 24.2 | (881) | 40.9 | (1746) |
| High | 13.8 | (508) | 13.9 | (470) | 12.7 | (460) | 14.8 | (632) |
| Income | ||||||||
| Not provided | 7.6 | (282) | 5.9 | (200) | 9.1 | (329) | 5.5 | (234) |
| Low | 29.1 | (1073) | 27.7 | (938) | 30.6 | (1111) | 37.6 | (1606) |
| Moderate | 34.8 | (1283) | 33.7 | (1139) | 32.9 | (1194) | 34.5 | (1476) |
| High | 28.5 | (1049) | 32.7 | (1104) | 27.5 | (1000) | 22.4 | (957) |
| Minority status | ||||||||
| Other | 88.9 | (3277) | 86.7 | (2930) | 95.2 | (3458) | 78.4 | (3348) |
| Identified minority | 11.1 | (410) | 13.3 | (451) | 4.8 | (176) | 21.6 | (925) |
| CPD | ||||||||
| Mean | 16.4 | (3687) | 17.9 | (3381) | 16.9 | (3634) | 18.1 | (4273) |
| SD | 9.7 | 12.9 | 10.7 | 11.6 | ||||
| Prior quit attempts | ||||||||
| Attempt in past year | 46.4 | (1710) | 45.7 | (1544) | 38.8 | (1411) | 43.8 | (1871) |
| No attempt | 53.6 | (1977) | 54.3 | (1837) | 61.2 | (2223) | 56.2 | (2402) |
Adult smokers were defined as 18 years or older, smoked more than 100 cigarettes in their life, and smoked at least once in the past 30 days at recruitment.
CPD, cigarettes per day; SD, standard deviation
Responses to Health Warnings—Wave 1
Figure 3 shows responses to health warnings across four survey waves. At Wave 1, Canadian smokers were significantly more likely to report noticing health warnings compared to smokers in the other three countries: 60% of Canadian smokers noticed the warning “often” or “very often”, compared to 52% of Australians (OR=1.48, CI95=1.25–1.63, p<0.001), 44% of UK smokers (OR=1.95, CI95=1.71–2.23, p<0.001), and 30% of U.S. smokers (OR=3.72, CI95=3.24–4.28, p<0.001). Canadian smokers reported greater levels for every measure recorded at Wave 1 (p<0.001 for all comparisons).
Figure 3.
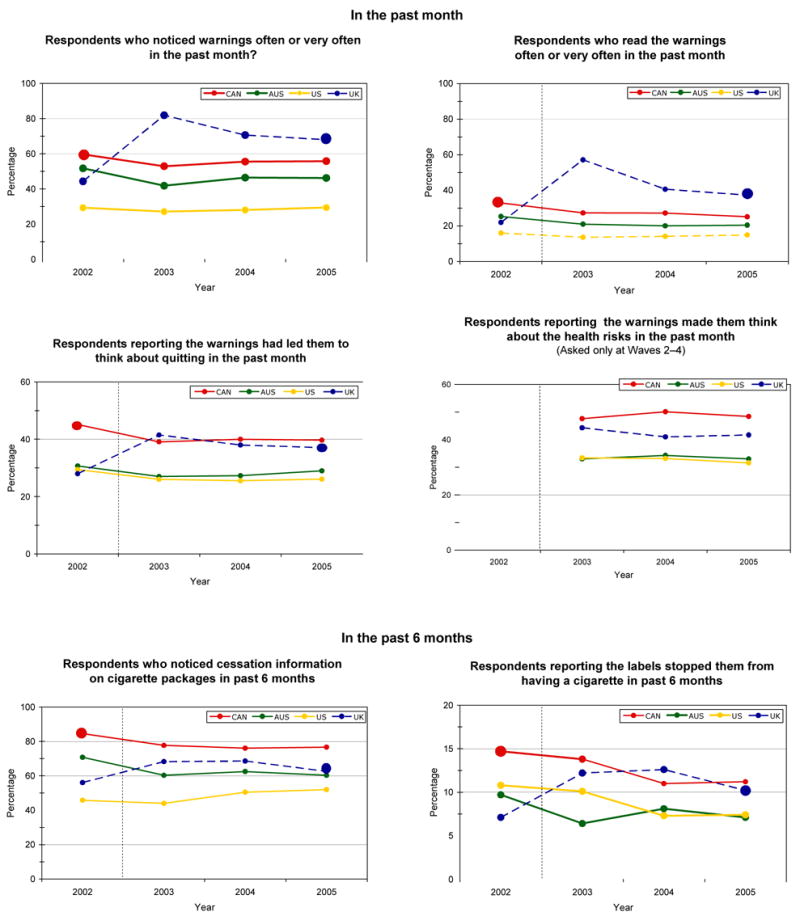
Responses to cigarette health warnings between 2002 and 2005 (n =14,975)* †
† The vertical dotted line indicates the implementation date of the new health warnings in the UK.
*The Wave 1 data from Canada and Wave 4 data from the UK have been highlighted to indicate 2.5 year post-implementation dates in each country.
Changes following UK Enhancement—Wave 2
At Wave 2, after the new UK warnings were implemented, measures of salience and self-reported impact significantly increased among UK smokers (all p <0.001), whereas no increases were observed among smokers in Canada, Australia, or the U.S. For example, the proportion of UK smokers who noticed health warnings on packages “often” or “very often” increased from 44.4% to 82.0% (p<0.001)—the highest level of any country. In fact, UK respondents reported significantly greater levels of salience and self-reported impact on every Wave 2 measure compared to Australian and U.S. respondents. For example, at Wave 2, UK smokers were significantly more likely to report that the health warnings had deterred them from having a cigarette (12.2%) compared to U.S. (10.1%; OR=1.58, CI95=1.25–2.00, p <0.001) and Australian smokers (9.7%; OR=2.59 CI95=2.02–3.32, p <0.001). In contrast, Canadian smokers continued to report greater levels of noticing anti-smoking/cessation information on packs than UK smokers (77.7% vs 68.3%, p <0.001), with no significant differences in thinking about quitting (39.1% vs 41.5%, n.s.), or thinking about the health risks because of the warnings (47.6% vs 44.3%, n.s.).
Between Waves 2 and 4, the levels of salience and self-reported impact decreased in the UK (p<0.001 for all comparisons), although levels remained above the U.S. and Australia in every case (p ≤0.02 for all). There were no significant decreases between Waves 2 and 4 for any measure in the other countries.
Comparison Between UK and Canadian Warnings 2.5 Years After Implementation
In order to adjust for the “novelty effect” associated with the introduction of new warnings, Wave 1 responses among Canadian smokers were compared to Wave 4 responses among UK smokers to compare data collected at similar time points following the implementation of new warnings in each country. At Wave 4, UK smokers reported significantly higher levels of noticing (68.0%; OR=1.40, CI95=1.21–1.62; p <0.001) and reading the warnings (37.3%; OR=1.39, CI95=1.20–1.61; p <0.001) than Canadian smokers at Wave 1 (59.7% and 32.8%, respectively). However, Canadian smokers at Wave 1 were significantly more likely than UK smokers at Wave 4 to report that they had noticed cessation information on packs (84.6% vs 62.6%; OR=3.28, CI95=2.76–3.90; p <0.001), stopped from smoking a cigarette as a result of the warnings (14.7% vs 10.2%; OR=1.35, CI95=1.09–1.67, p =0.007), and that warnings had led them to think about quitting (45.1% vs 37.1%; OR=1.16, CI95=1.00–1.34, p =0.047). Note that respondents were not asked whether the warnings had made them think about the health risks of smoking at Wave 1; however, Canadian smokers reported greater levels than UK smokers at Wave 3 (50.1% vs 41.0%; p <0.001) and Wave 4 (48.4% vs 41.7%; p =0.004), with no significant difference at Wave 2 (47.6% vs 44.3%; n.s.).
DISCUSSION
This study suggests that more prominent health warnings are associated with greater levels of awareness and perceived effectiveness among smokers. In particular, the findings provide strong support for the effectiveness of new health warnings implemented on UK packages that were enhanced to meet the minimum international standards. The new UK warnings were significantly more likely to be noticed and read than the previous set of UK warnings, as well as the U.S. and Australian warnings, neither of which met the minimum international standards. UK smokers were also more likely to report that the new warnings had led them to think about quitting, to think about the health risks of smoking, and had deterred them from having a cigarette compared to Australian and U.S. smokers.
The findings highlight the “novelty” effect of health communications and the importance of periodically revising the warnings on cigarette packages.6,24 Indeed, the enhanced UK warnings were considerably more likely to be noticed than the Australian warnings, which are only slightly smaller, but had been in place for more than 8 years at the start of the survey. Not surprisingly, declines in salience and impact were also observed during the 2.5 years following the introduction of the new UK warnings. The declines were greatest for measures of salience—noticing and reading the warnings—whereas measures of perceived effectiveness were somewhat less likely to decrease. This pattern suggests that the key downstream effects of warnings may persist for longer than the more immediate measures of salience. It is interesting to note, however, that measures of salience and impact remained high in Canada even 4 years after implementation. This is consistent with the principle that larger, more vivid warnings are more likely to retain their salience over time than less prominent warnings.18 Additional follow-up data will be required to examine whether the text warnings in the UK are associated with an accelerated wear-out curve compared to the Canadian pictorial warnings.
Whilst the results demonstrate the effectiveness of prominent text-based warnings, they also suggest that larger pictorial warnings may have an even greater impact. Data collected 2.5 years after the implementation of the Canadian pictorial warnings and 2.5 years after the implementation of the new UK warnings indicate that the Canadian warnings had impact levels above the UK warnings for each of the measures of “self-reported impact,” as well as noticing anti-smoking information on packages. Although UK smokers were more likely to notice and read package warnings, Canadian smokers were significantly more likely to report thinking about the health risks of smoking, to stop from having a cigarette, and to think about quitting because of the health warnings. These findings may simply be due to the larger size of the Canadian warnings; however, they are consistent with a growing body of literature, which suggests that graphic warnings typically evoke more of an emotional response, increase memory and awareness of health risks, and reinforce motivations to quit smoking to a greater extent than text warnings.10,17,25
It should also be noted that, in contrast to noticing and reading the warnings, at no point were UK smokers more likely to report noticing anti-smoking/cessation information on packages than Canadian smokers. Although the new UK warnings include two specific messages on smoking cessation, they appear only on the “back” of packages approximately 5% of the time due to the rotating nature of the warnings. In contrast, every Canadian package includes cessation tips and messages of encouragement on the inside of packages. Although these interior messages are not as noticeable as the warnings on the exterior of the pack, previous research suggests that most Canadian smokers are nevertheless familiar with their content.11 As the health risks depicted on packages become more explicit and direct, this type of supportive information may become increasingly important for helping smokers to change their behavior. Adding website information and toll-free telephone “quitlines” on cigarette packages also represent very promising ways of helping smokers to access cessation services.26 Indeed, the UK Department of Health estimates that the UK warnings have prompted an additional 2000–4000 calls to the NHS Smoking helpline every month.27
Limitations
Although the prospective quasi-experimental design utilized in this study offers considerable advantages over previous research evaluating product warnings, this research nevertheless has important limitations common to survey research, including bias from nonresponse and attrition. The data were weighted to help account for nonresponse and potential sample bias. In order to assess the threat of bias due to attrition and to examine any “time-in-sample” effects, each of the analyses was run with: (1) the “cohort” sample only (i.e., only those who completed all four waves); (2) the “repeat cross-sectional” sample (i.e., the first wave of data from each respondent only); and (3) all of the available data at each wave (as presented in the Results section). No significant differences were observed in any of the analyses. Another limitation concerns the self-report nature of the measures. For example, it is not possible to estimate the influence of the new UK warnings or the Canadian pictorial warnings on prevalence rates using the current data. National prevalence rates are determined by a constellation of individual, social, and environmental factors, including other policy measures as well as “secular” trends in marketing and pricing. However, the results from our analyses, as well as evaluation data from the UK National Health Services, are consistent with the hypothesis that more comprehensive package warnings increase the extent to which smokers notice, believe, and act on the health messages.27 Finally, the current study assessed only the impact of the warnings on adult smokers and included neither youth nor nonsmokers in the sample.
Overall, the current study indicates that larger, more comprehensive health warnings on cigarette packages are rated as more effective by smokers. The findings provide strong support for the effectiveness of prominent text warnings that meet the minimum international standards; however, the findings also suggest that larger pictorial warnings, such as those implemented in Canada and seven other countries to date, are likely the most effective means of communicating the full range and severity of health risks to smokers (see Figure 4). Finally, the U.S. warnings performed poorly compared to those in the other countries. The health warnings that appear on the side of U.S. cigarette packages provide even less health information than many other, more benign consumer goods. The current findings, along with previous research,7,10 suggest that U.S. smokers might benefit from large graphic warnings on cigarette packages.
Figure 4.
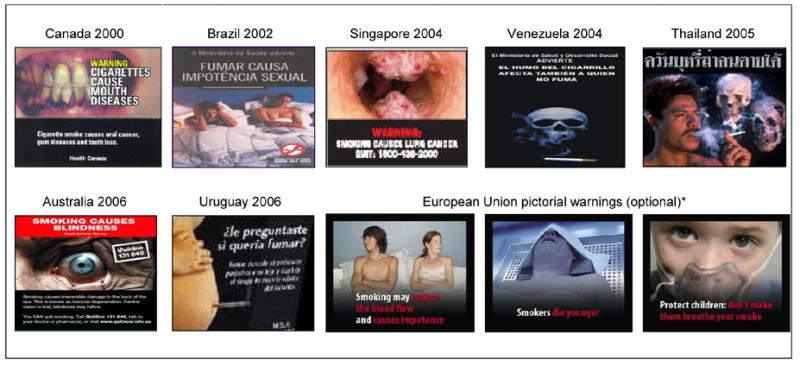
Countries with picture-based health warnings
*A set of pictorial warnings has been created for European Union members; however, each member can decide whether or not to adopt the pictorial warnings in place of the mandatory text-based warnings.
Acknowledgments
We wish to thank Christian Boudreau (PhD, Assistant Professor, University of Waterloo) for analytical support, as well as Jennifer Topham (BA, Research Assistant, University of Waterloo) and Carla Parkinson (BSc, Research Assistant, University of Waterloo) for their assistance in preparing this manuscript. This research was funded by grants from the National Cancer Institute of the United States (through R01 CA 100362 and through the Roswell Park Transdisciplinary Tobacco Use Research Center, P50 CA111236), Robert Wood Johnson Foundation (045734), Canadian Institutes of Health Research (57897), National Health and Medical Research Council of Australia (265903), Cancer Research UK (C312/A3726), Canadian Tobacco Control Research Initiative (014578), with additional support from the Centre for Behavioural Research and Program Evaluation, National Cancer Institute of Canada/Canadian Cancer Society.
None of the sponsors played any direct role in the design and conduct of the study; the collection, management, analysis, and interpretation of the data; or the preparation, review, and approval of the manuscript.
David Hammond had full access to all of the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Footnotes
CONTRIBUTIONS OF AUTHORS
David Hammond helped to design the measures, conduct the analysis, and was the primary author of the manuscript. Geoffrey Fong, Ron Borland, Mike Cummings, and Ann McNeill helped to design the study and write the manuscript. Pete Driezen helped to conduct the analysis and write the manuscript.
ETHICS CLEARANCE
The study protocol was cleared for ethics by the institutional review boards or research ethics boards of the University of Waterloo (Canada), Roswell Park Cancer Institute (U.S.), University of Strathclyde (UK), University of Stirling (UK), The Open University (UK), and The Cancer Council Victoria (Australia).
CONFLICTS OF INTEREST
No financial conflict of interest was reported by the authors of this paper.
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
References
- 1.Murray CJ, Lopez AD. Alternative projections of mortality and disability by cause 1990–2020: Global Burden of Disease Study. Lancet. 1997;349:1498–1504. doi: 10.1016/S0140-6736(96)07492-2. [DOI] [PubMed] [Google Scholar]
- 2.World Health Organization [homepage on the Internet] Tobacco Free Initiative. Information on global tobacco use. [cited 2006 June 11]. Available from: H http://www.who.int/tobacco/health_priority/en/index.htmlH.
- 3.World Health Organization [homepage on the Internet] Geneva, Switzerland: 2005. WHO Framework Convention on Tobacco Control. [cited 2006 June 11]. Available from: H http://www.who.int/tobacco/framework/WHO_FCTC_english.pdfH. [Google Scholar]
- 4.Fischer PM, Richards EJB, Krugman DM. Recall and eye tracking study of adolescents viewing tobacco advertisements. J Am Med Assoc. 1989;261:84–89. [PubMed] [Google Scholar]
- 5.Crawford MA, Balch GI, Mermelstein R the Tobacco Control Network Writing Group. Responses to tobacco control policies among youth. Tob Control. 2002;11:14–19. doi: 10.1136/tc.11.1.14. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Borland R. Tobacco health warnings and smoking-related cognitions and behaviours. Addiction. 1997;92:1427–35. [PubMed] [Google Scholar]
- 7.Willemsen MC. The new EU cigarette health warnings benefit smokers who want to quit the habit: results from the Dutch Continuous Survey of Smoking Habits. Eur J Public Health. 2005;15:389–92. doi: 10.1093/eurpub/cki061. [DOI] [PubMed] [Google Scholar]
- 8.Tandemar Research P. f. H. C. Cigarette packaging study: The evaluation of new health warning messages. 1996. (Rep. No. TR#663022) [Google Scholar]
- 9.Borland R, Hill D. Initial impact of the new Australian tobacco health warnings on knowledge and beliefs. Tob Control. 1997;6:317–325. doi: 10.1136/tc.6.4.317. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Hammond D, Fong GT, Borland R, McNeill A, Cummings KM, Hastings G. Effectiveness of cigarette warning labels in informing smokers about the risks of smoking: findings from the International Tobacco Control (ITC) Four Country Survey. Tob Control. 2006;15(Suppl III):iii19–iii25. doi: 10.1136/tc.2005.012294. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Hammond D, Fong GT, McDonald PW, Cameron R, Brown KS. The impact of the graphic Canadian warning labels on adult smokers. Tob Control. 2003;12:391–95. doi: 10.1136/tc.12.4.391. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Hammond D, Fong GT, McDonald PW, Brown KS, Cameron R. Graphic cigarette package warning labels do not lead to adverse outcomes: Evidence from Canadian smokers. Am J Public Health. 2004;94:1442–45. doi: 10.2105/ajph.94.8.1442. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.O’Hegarty M, Pederson L, Nelson D, Mowery P, Gable J, Wortley P. Reactions of Young Adult Smokers to Warning Labels on Cigarette Packages. Am J Prev Med. 2006;30(6):467–473. doi: 10.1016/j.amepre.2006.01.018. [DOI] [PubMed] [Google Scholar]
- 14.Koval J, Aubur J, Pederson L, O’Hegarty M, Chan S. The potential effectiveness of warning labels on cigarette packages: The perceptions of young adult Canadians. Can J Public Health. 2005 Sep/Oct;96(5):353–356. doi: 10.1007/BF03404031. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Henderson B. Wear out: An empirical investigation of advertising wear-in and wear-out. J Advert Res. 2000;6:95–100. [Google Scholar]
- 16.Bornstein RF. Exposure and affect: Overview and meta-analysis of research. Psychol Bull. 1989;106:265–289. [Google Scholar]
- 17.Health Canada. Prepared by Environics Research Group. 1999. Health Warning Testing: Final Report. [Google Scholar]
- 18.Strahan EJ, White K, Fong GT, Fabrigar LR, Zanna MP, Cameron R. Enhancing the effectiveness of tobacco package warning labels: a social psychological perspective. [Review] [92 refs] Tob Control. 2002 Sep;11(3):183–90. doi: 10.1136/tc.11.3.183. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.European Commission proposal COM (99)594 Final 16th November 1999. [cited 2006 June 11] Available from: H http://TUeuUTropa.TUeuUT.int/TUeuUTr-lex/pri/en/oj/dat/2001/l_194/l_19420010718en00260034.pdfH.
- 20.Binson D, Canchola JA, Catania JA. Random selection in a national telephone survey: a comparison of the Kish, next-birthday, and last-birthday methods. J Off Stat. 2000;16:53–60. [Google Scholar]
- 21.Singer E, van Hoewyk J, Maher MP. Experiments with incentives in telephone surveys. Public Opin Q. 2000;64:171–188. doi: 10.1086/317761. [DOI] [PubMed] [Google Scholar]
- 22.Thompson ME, Fong GT, Hammond D, et al. The methodology of the International Tobacco Control Policy Evaluation (Four-Country) Survey (ITCPES) Tob Control. 2006;15(Suppl III):iii12–iii18. doi: 10.1136/tc.2005.013870. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Heatherton TF, Koslowski LT, Frecker RC, Rickert WS, Robinson J. Measuring the heaviness of smoking using self-reported time to the first cigarette of the day and number of cigarettes smoked per day. Br J Addict. 1989;84:791–800. doi: 10.1111/j.1360-0443.1989.tb03059.x. [DOI] [PubMed] [Google Scholar]
- 24.Health Canada. The Health effects of tobacco and health warning messages on cigarette packages—Survey of adults and adults smokers: Wave 9 surveys. Prepared by Environics Research Group. 2005 Jan [Google Scholar]
- 25.Commonwealth of Australia. Developmental Research for New Australian Health Warnings on Tobacco Products. Population Health Division. Department of Health and Ageing. Commonwealth of Australia. 2003 [cited 2006 June 11]. Available from: H http://www.health.gov.au/Internet/wcms/Publishing.nsf/Content/health-pubhlth-strateg-drugs-tobacco-warnings.htm.
- 26.Willemsen MC, Simons C, Zeeman G. Impact of the new EU health warnings on the Dutch quit line. Tob Control. 2002;11:382. doi: 10.1136/tc.11.4.381. [DOI] [PMC free article] [PubMed] [Google Scholar]