

Abstract
In a double blind placebo controlled 3 year osteoporosis study in elderly women, we collected prospective data on falls. The study population comprised 489 normal elderly women aged 65–77 years randomized to 4 groups, placebo, calcitriol 0.25 mcg bid, conjugated equine estrogens (0.625mg/d )and calcitriol + estrogen. Falls occurred in 57 percent of all women.
Using a Poisson regression model, the placebo group with low GFR - creatinine clearance (CrCl <60 ml/min) had 60 percent more falls compared to the group with CrCl ≥ 60mls/min. Further sub group analyses showed that there is no increased risk of falls with CrCl 60–70, 70–80 and >90ml/min. Calcitriol treatment significantly reduced the number of falls by 50 percent (OR=0.5, 95% CI: 0.4–0.9, p=0.010) compared to placebo in the low CrCl group.
The group with lower CrCl had lower calcium absorption (p<0.001), lower serum 1,25 dihydroxyvitamin D (1,25(OH)2D) (p<0.001) and normal serum 25OHD suggesting that there is decreased conversion of 25OHD to 1,25(OH)2D by the aging kidney. It is postulated that the decrease in falls on calcitriol therapy is related to an increase in serum 1,25 (OH)2D, upregulation of VDR and improvement in muscle strength although one cannot exclude an effect on the central nervous system.
Keywords: Falls; GFR; Creatinine clearance; 1,25 dihydroxyvitamin D Calcitriol treatment; Aging
Introduction
Falls in elderly people represent a serious public health problem in United States. Approximately 30 percent of people over age of 65 and 50 percent over age 80 years fall each year and ten percent of falls cause fractures. There is increasing data relating falls and decreased muscle strength to changes in vitamin D metabolism and decreasing renal function. A possible link between these two observations is that the decrease in renal function with age measured by creatinine clearance (CrCl) is associated with a decrease in production of 1,25 dihydroxyvitamin D together with a decrease in vitamin D receptors (VDR) in muscle.
We showed earlier that treatment with 1,25 dihydroxyvitamin D (calcitriol) vitamin D significantly reduced the risk of falls in elderly women (1;2) and now this has been confirmed in men and women using alphacalcidol (3;4).
A creatinine clearance of <65 ml/min has been recently reported as a significant risk factor for falls and increased risk of vertebral, hip and radial fractures in elderly men and women treated for osteoporosis (5;6). Treatment with alphacalcidol significantly reduced the number of fallers and falls in a group with low CrCl (< 65 ml/min) (4).
In an osteoporosis intervention trial primarily designed to test the efficacy of conjugated estrogens and calcitriol given alone or in combination on bone loss, we had the opportunity to collect prospective data on the incidence of falls and the effect of estrogen, calcitriol and combination (calcitriol +estrogen) therapies on fall incidence. We have shown that a CrCl <60 mls/min is associated with a 60 percent increase in falls. In this paper we examine different levels of CrCl in relation to falls.
Materials and Methods
Four hundred and eighty nine elderly women aged 65–77 years were enrolled into a prospective double blind randomized placebo controlled clinical trial (STOP IT) lasting 3 years to test the efficacy of conjugated equine estrogens and calcitriol given individually or in combination, on bone loss (1). Women were excluded if they had severe chronic illness (chronic liver or kidney disease, severe COPD, severe rheumatoid arthritis, serious heart failure), had primary hyperparathyroidism or active renal stone disease, were on certain medications, such as bisphosphonates, anticonvulsants, estrogen, fluoride, or thiazide diuretics in the previous six months. Women were randomized to one of 4 groups; Conjugated equine estrogens 0.625 mg/daily (Premarin) (medroxyprogesterone acetate 2.5mg/daily (Provera) was added if the women had a uterus), calcitriol 0.25mcg twice daily, and the combination of both or placebo. 489 women were randomized to treatment. 415 came in for a final visit at 3 years. Creighton University Human Institutional Review Board approved the trial and all patients signed an informed consent form.
Falls
Falls data was collected prospectively by an interview-administered questionnaire on the incidence of falls every 6 months for the entire study period of 36 months. Falls were defined as “unintentionally coming to rest on the ground, floor or other lower level”. However, the exact date of the fall was not ascertained at the time of the scheduled visit.
Biochemical analysis
Fasting blood and 24 h urine samples were obtained from the subjects at baseline and at the end of the study. Blood specimens were allowed to clot and were then centrifuged at 4°C for 15 min at 2056xg to separate serum. All samples were stored frozen at −70°C until analysis. Total calcium and creatinine in urine samples were determined by automated procedures (Nova Nucleus Chemistry Analyzer, Waltham, MA) Creatinine clearance (CrCl) was estimated from a 24h urine collection and serum/urine creatinine. Estimated CrCl was calculated using the Cockcroft Gault (7)and MDRD (8) formulae. Serum 25-hydroxyvitamin D (calcidiol, 25OHD) was assayed by a competitive protein binding assay. Serum 1,25(OH)2 D was measured by a non equilibrium radioreceptor assay (Incstar Corp., Stillwater, MN). Serum intact parathyroid hormone (PTH) was measured with the Allegro immunoradiometric assay (Nichols Institute, San Juan Capistrano, CA).
Statistical analysis
All analyses were done by the SAS statistical package (version 9.1, SAS Inc., Chicago). The presented results are from ITT analyses. Baseline patient characteristics and biochemical variables were compared according to CrCl with t test. Univariate comparisons of the physical performance variables were conducted with ANOVA. Poisson regression was used to examine the predictors of the cumulative number of falls at 6, 12, 24 and 36 months. Treatment group and subgroups of CrCl were considered as predictors. In a multivariate model falls were adjusted for significant confounders at each time point. The covariates used in the model were age, baseline serum 25OHD, weight, height. Serum 1,25(OH)2D was significantly associated with falls but was not included in the model. Data are summarized with unadjusted means and standard errors.
Results
The distribution of low CrCl by age is shown in figure 1. Most values for the low CrCl group are distributed equally over the age span of the study population.
Figure 1.
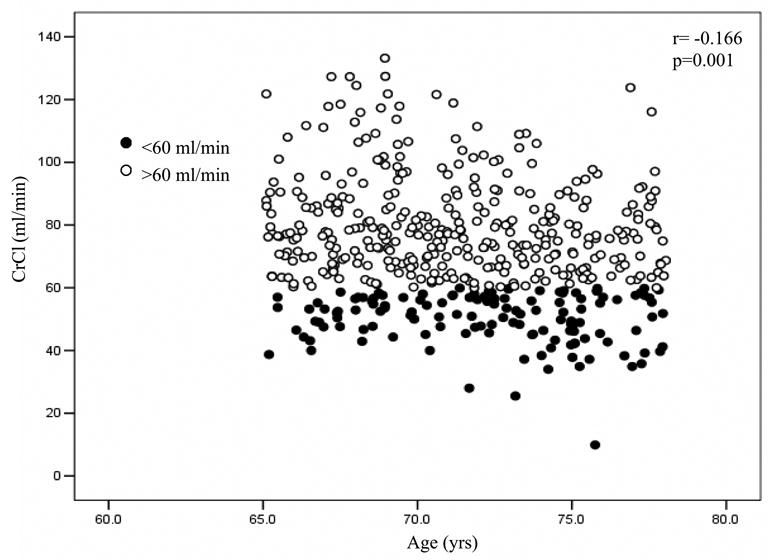
Creatinine Clearance with age. (● CrCl < 60ml/min, ○ CrCl > 60ml/min)
Baseline characteristics of study population
Mean measured 24 h urine CrCl (ml/min) was 50.3±0.69 in women with CrCl <60 ml/min and 80.4±0.83 in women with CrCl >60 ml/min. Significant differences for the low CrCl group were as follows: Mean age 72 years- one year older (p< 0.02); weight 65kg–5kg lower(p< 0.002); serum 1,25(OH)2D levels 33.1pg/ml–2pg/ml lower(p< 0.01); Calcium absorption was significantly lower(p< 0.001);; Serum 25OHD 32.7ng/ml and PTH 36.6pg/ml were not significantly different.
Falls
Out of 415 subjects who completed the study and came in for the 36 month visit, the percentage of subjects in each group having a fall at any time during the study was 64% on placebo, 49.5% on calcitriol (p<0.001), 58% on calcitriol + ET/HT, and 57% on ET/HT alone; there was no effect of treatment on the number of fallers. Falls are distributed across the age span of the study subjects (Fig 1).
CrCl and falls in placebo and treatment groups
From the Poisson regression model, urine CrCl, whether measured or estimated from the CG and MDRD formulae, was a significant predictor of mean cumulative number of falls in the placebo group (p=0.012), but not in the treatment groups. CrCl was not a significant predictor of fallers in any of the treatment groups. Comparing groups with CrCl <60 vs >60 ml/min, the mean cumulative number of falls on placebo was significantly higher in the group with CrCl<60 ml/min (OR=1.6, 95% CI:1.1–2.2, p=0.012).
We compared fall incidence at different levels of CrCl <60, 60–70, 70–80, 80–90 and<90ml/min. Only in the group <60 ml/min was there a significant increase in falls (table 2).
We also compared fall incidence using the CrCl classification estimated from the formulae of Cockcroft Gault and MDRD. Results were similar with only the < 60 ml/min group having a significant increase in falls.(table 2).
In women with CrCl<60 ml/min, whether measured or using the formulae, calcitriol treatment significantly reduced the cumulative number of falls by 50 percent (p<0.01), calcitriol + estrogen reduced falls by 40 percent (p<0.01) whereas estrogen was not effective. The effect of calcitriol treatment was evident by 12 months of treatment and statistically significant at 36 months of treatment.
Discussion
In this study of normal elderly women, we previously originally noted that a low 24h CrCl (<60 ml/min) was associated with an increase in the number of falls but not in the number of fallers. We explored the data further by comparing fall incidence in sub groups of CrCl. There was no evidence that falls were increased in the groups with CrCl of 60–70 or 70–80 or >90ml/min, so it would seem that this fall effect is associated only in the women with CrCl< 60ml/min or stage III chronic renal failure. Similar results were found using CrCl estimated from the Cockroft-Gault and MDRD-4 variable formulae. These observations suggest that Cockroft-Gault and MDRD formulae easily allow one to predict which elderly women are at risk for falls from a single blood measurement and body weight, though whether this applies to women with a low body weight is not known. Calcitriol was effective in reducing falls in women with CrCl <60ml/min by almost 50 percent, there was also a marginal effect at 60–70ml/min though it was less significant (P<0.04). Because we saw essentially the same results on treatment with estrogen + calcitriol but not estrogen alone, the findings confirm the that it is the calcitriol that is effective in reducing falls. The results of the present study are in agreement with the recently published observations of Dukas et al (4–6) in community-dwelling elderly men and women age 75 years, from Switzerland. They used the Cockroft-Gault formula to predict CrCl and using a cut off of <65mls/min showed a similar association between low CrCl and falls. They showed also a significant reduction in falls on alphacalcidol which is a pro drug for calcitriol. In a recent paper they have extended their original findings to a study in more than 5,000 men and women and confirmed the link between low CrCl and falls and also with fractures (6).
A decrease in the muscle strength with aging is associated with an increased incidence of falls in the elderly (9). Vitamin D supplementation improves muscle strength and prevents falls in the elderly (10–13), probably by increasing production of 1,25(OH)2D and its interaction with the highly specific nuclear receptors in muscle tissue (14;15). The results from our study were observed in women with a mean normal serum 25OHD of 30 ng/ml so that vitamin D insufficiency i.e serum 25OHD <20 ng/ml was not a contributing cause. Several studies show that higher serum 25OHD levels of 30–32 ng/ml are needed to reduce serum PTH in the elderly so it is possible that serum 25OHD is not high enough for elderly subjects and that substrate deficiency or insufficiency may be a contributing factor, especially in areas of the world where vitamin D deficiency and insufficiency are common. However, because there is decreased conversion of 25OHD to 1,25(OH)2D in the aging kidney, increasing the substrate may have a limited effect (16). An additional factor may be the status of the VDR. Receptors for 1,25(OH)2D in muscle have been reported to be decrease with aging (17) and if combined with the finding of lower serum 1,25(OH)2D could be responsible for decreased muscle strength. The group with low CrCl also had significantly lower calcium absorption and serum 1,25(OH)2D. Thus endogenous calcitriol, though normal, needs to be higher. There have not been many studies of simple vitamin D therapy. Two recent meta-analyses of vitamin D 400–800 IU/d on falls were not able to show a reduction in falls whereas calcitriol and its analogs were effective (18;19). Controlled trials are needed to compare a higher dose of vitamin D with calcitriol because of the potential benefit and economic impact of using an inexpensive therapy such as vitamin D.
Figure 2.
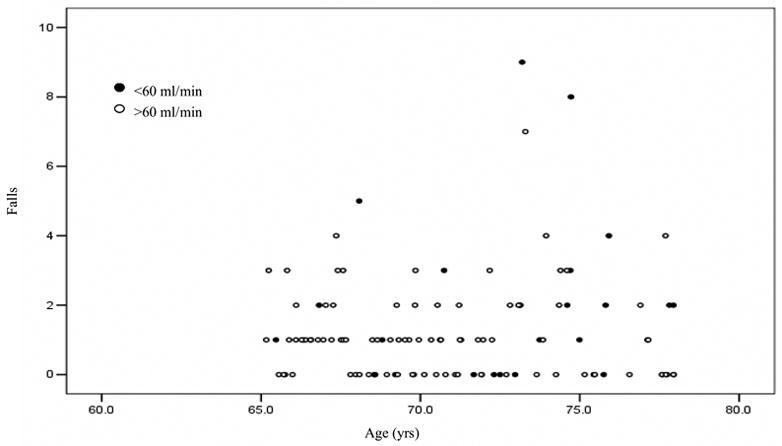
Falls according to age. (● CrCl < 60ml/min, ○ CrCl > 60ml/min)
Table 1.
Odds ratios of falls using different CrCl measurements.
| Odds ratio of falls in treatment groups comparing measured CrCl cutpoints at 36 months
| ||||
|---|---|---|---|---|
| n | Odds ratio | 95% CI | p | |
| Placebo | ||||
| <60 | 28 | 1 | ||
| 60–70 | 19 | 0.73 | (0.44, 1.22) | 0.23 |
| 70–80 | 23 | 0.55 | (0.33, 0.90) | 0.019 |
| 80–90 | 17 | 0.78 | (0.47, 1.30) | 0.34 |
| =90 | 25 | 0.55 | (0.34, 0.89) | 0.015 |
| Odds ratio of falls in treatment groups comparing Cockcroft-Gault formula CrCl cutpoints at 36 months | ||||
|
| ||||
| n | Odds ratio | 95% CI | p | |
|
| ||||
| Placebo | ||||
| <60 | 48 | 1 | ||
| 60–70 | 22 | 0.67 | (0.42, 1.06) | 0.086 |
| 70–80 | 15 | 0.46 | (0.25, 0.84) | 0.012 |
| 80–90 | 12 | 0.69 | (0.39, 1.21) | 0.20 |
| =90 | 15 | 0.93 | (0.57, 1.51) | 0.76 |
| Odds ratio of falls in treatment groups comparing MDRD 4 variable formula CrCl cutpoints at 36 months | ||||
|
| ||||
| n | Odds ratio | 95% CI | p | |
|
| ||||
| Placebo | ||||
| <60 | 24 | 1 | ||
| 60–80 | 61 | 0.79 | (0.53, 1.18) | 0.25 |
| =80 | 27 | 0.79 | (0.49, 1.27) | 0.33 |
| Odds ratio of falls by CrCl cutpoints comparing placebo to treatment at different CrCl at 36 months
| ||||
| n | Odds ratio | 95% CI | p | |
|
| ||||
| Measured CrCl <60 | ||||
| Placebo | 24 | 1 | ||
| Calcitriol | 30 | 0.52 | (0.32, 0.86) | 0.010 |
| ET/HT+Calcitriol | 30 | 0.58 | (0.37, 0.90) | 0.016 |
| ET/HT | 22 | 0.72 | (0.49, 1.32) | 0.39 |
| Measured CrCl 60–70 | ||||
| Placebo | 22 | 1 | ||
| Calcitriol | 30 | 0.45 | (0.23, 0.88) | 0.020 |
| ET/HT+Calcitriol | 30 | 0.68 | (0.34, 1.35) | 0.27 |
| ET/HT | 33 | 0.64 | (0.35, 1.16) | 0.14 |
| Measured CrCl 70–80 | ||||
| Placebo | 15 | 1 | ||
| Calcitriol | 11 | 0.91 | (0.49, 1.70) | 0.78 |
| ET/HT+Calcitriol | 18 | 1.35 | (0.79, 2.30) | 0.27 |
| ET/HT | 25 | 1.06 | (0.61, 1.83) | 0.85 |
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
Contributor Information
JC Gallagher, Bone Metabolism, Creighton University, Omaha, NE 68131, USA.
Prema Rapuri, Bone Metabolism, Creighton University, Omaha, NE 68131, USA.
Lynette Smith, Dept Preventive Medicine, University Nebraska Medical Center, Omaha, NE68131, USA.
References
- 1.Gallagher JC, Fowler SE, Detter JR, Sherman SS. Combination treatment with estrogen and calcitriol in the prevention of age-related bone loss. J Clin Endocrinol Metab. 2001;86:3618–3628. doi: 10.1210/jcem.86.8.7703. [DOI] [PubMed] [Google Scholar]
- 2.Gallagher JC. The effects of calcitriol on falls and fractures and physical performance tests. J Steroid Biochem Mol Biol. 2004;89–90:497–501. doi: 10.1016/j.jsbmb.2004.03.059. [DOI] [PubMed] [Google Scholar]
- 3.Dukas L, Bischoff HA, Lindpaintner LS, Schacht E, Birkner-Binder D, Damm TN, Thalmann B, Stahelin HB. Alfacalcidol reduces the number of fallers in a community-dwelling elderly population with a minimum calcium intake of more than 500 mg daily. J Am Geriatr Soc. 2004;52:230–236. doi: 10.1111/j.1532-5415.2004.52060.x. [DOI] [PubMed] [Google Scholar]
- 4.Dukas L, Schacht E, Mazor Z, Stahelin HB. Treatment with alfacalcidol in elderly people significantly decreases the high risk of falls associated with a low creatinine clearance of <65 ml/min. Osteoporos Int. 2005;16:198–203. doi: 10.1007/s00198-004-1671-9. [DOI] [PubMed] [Google Scholar]
- 5.Dukas L, Schacht E, Stahelin HB. In elderly men and women treated for osteoporosis a low creatinine clearance of <65 ml/min is a risk factor for falls and fractures. Osteoporos Int. 2005;16:1683–1690. doi: 10.1007/s00198-005-1903-7. [DOI] [PubMed] [Google Scholar]
- 6.Dukas LC, Schacht E, Mazor Z, Stahelin HB. A new significant and independent risk factor for falls in elderly men and women: a low creatinine clearance of less than 65 ml/min. Osteoporos Int. 2005;16:332–338. doi: 10.1007/s00198-004-1690-6. [DOI] [PubMed] [Google Scholar]
- 7.Cockcroft DW, Gault MH. Prediction of creatinine clearance from serum creatinine. Nephron. 1976;16:31–41. doi: 10.1159/000180580. [DOI] [PubMed] [Google Scholar]
- 8.Levey AS, Bosch JP, Lewis JB, Greene T, Rogers N, Roth D. A more accurate method to estimate glomerular filtration rate from serum creatinine: a new prediction equation. Modification of Diet in Renal Disease Study Group. Ann Intern Med. 1999;130:461–470. doi: 10.7326/0003-4819-130-6-199903160-00002. [DOI] [PubMed] [Google Scholar]
- 9.Moreland JD, Richardson JA, Goldsmith CH, Clase CM. Muscle weakness and falls in older adults: a systematic review and meta-analysis. J Am Geriatr Soc. 2004;52:1121–1129. doi: 10.1111/j.1532-5415.2004.52310.x. [DOI] [PubMed] [Google Scholar]
- 10.Bischoff HA, Stahelin HB, Tyndall A, Theiler R. Relationship between muscle strength and vitamin D metabolites: are there therapeutic possibilities in the elderly? Z Rheumatol. 2000;59(Suppl 1):39–41. doi: 10.1007/s003930070037. [DOI] [PubMed] [Google Scholar]
- 11.Bischoff HA, Stahelin HB, Dick W, Akos R, Knecht M, Salis C, Nebiker M, Theiler R, Pfeifer M, Begerow B, Lew RA, Conzelmann M. Effects of vitamin D and calcium supplementation on falls: a randomized controlled trial. J Bone Miner Res. 2003;18:343–351. doi: 10.1359/jbmr.2003.18.2.343. [DOI] [PubMed] [Google Scholar]
- 12.Dhesi JK, Jackson SH, Bearne LM, Moniz C, Hurley MV, Swift CG, Allain TJ. Vitamin D supplementation improves neuromuscular function in older people who fall. Age Ageing. 2004;33:589–595. doi: 10.1093/ageing/afh209. [DOI] [PubMed] [Google Scholar]
- 13.Pfeifer M, Begerow B, Minne HW, Abrams C, Nachtigall D, Hansen C. Effects of a short-term vitamin D and calcium supplementation on body sway and secondary hyperparathyroidism in elderly women. J Bone Miner Res. 2000;15:1113–1118. doi: 10.1359/jbmr.2000.15.6.1113. [DOI] [PubMed] [Google Scholar]
- 14.Bischoff HA, Borchers M, Gudat F, Duermueller U, Theiler R, Stahelin HB, Dick W. In situ detection of 1,25-dihydroxyvitamin D3 receptor in human skeletal muscle tissue. Histochem J. 2001;33:19–24. doi: 10.1023/a:1017535728844. [DOI] [PubMed] [Google Scholar]
- 15.Simpson RU, Thomas GA, Arnold AJ. Identification of 1,25-dihydroxyvitamin D3 receptors and activities in muscle. J Biol Chem. 1985;260:8882–8891. [PubMed] [Google Scholar]
- 16.Kinyamu HK, Gallagher JC, Petranick KM, Ryschon KL. Effect of parathyroid hormone (hPTH[1–34]) infusion on serum 1,25-dihydroxyvitamin D and parathyroid hormone in normal women. J Bone Miner Res. 1996;11:1400–1405. doi: 10.1002/jbmr.5650111005. [DOI] [PubMed] [Google Scholar]
- 17.Bischoff-Ferrari HA, Borchers M, Gudat F, Durmuller U, Stahelin HB, Dick W. Vitamin D receptor expression in human muscle tissue decreases with age. J Bone Miner Res. 2004;19:265–269. doi: 10.1359/jbmr.2004.19.2.265. [DOI] [PubMed] [Google Scholar]
- 18.Bischoff-Ferrari HA, Dawson-Hughes B, Willett WC, Staehelin HB, Bazemore MG, Zee RY, Wong JB. Effect of Vitamin D on falls: a meta-analysis. JAMA. 2004;291:1999–2006. doi: 10.1001/jama.291.16.1999. [DOI] [PubMed] [Google Scholar]
- 19.Gillespie LD, Gillespie WJ, Robertson MC, Lamb SE, Cumming RG, Rowe BH. The Cochrane Collaboration. John Wiley and Sons Ltd; 2006. Interventions for preventing falls in elderly people. [Google Scholar]