

Abstract
We tested the hypothesis that a computerized intervention would be as efficacious as an in-person, small-group intervention in reducing sexual risk behaviors. The sexual behavior of high-risk adolescents in 3 intervention conditions was examined: (1) computer based, (2) small groups, and (3) control. Adolescents in the computerized intervention were significantly less likely to engage in sexual activity and reported significantly fewer partners. For some youths, computers are a viable way to deliver prevention information and promote skill development.
Delinquent youths (defined as youths involved with the juvenile justice system) are at substantial risk for contracting HIV because they engage in unprotected sexual behavior, and their sexual activity is often associated with substance use. Although delinquent youths are similar to their peers in knowledge and attitudes about AIDS,1,2 they are more likely to be sexually active, initiate sexual activity at younger ages, and have more sexual partners.1–3 Therefore, delinquent youths are a subgroup in which successful interventions are needed.
An intervention with established efficacy is Project LIGHT (Living in Good Health Together).4 This intervention targeted both adults and adolescents who recently engaged in high-risk behaviors and produced increases in condom use of 160% and increases in consistent condom use of 45%. Given the intervention’s success with this target population and with adolescents,5 we hypothesized that it would be an efficacious program for delinquent youths.
However, interventions need to be designed a priori for implementation with fidelity and in natural adolescent settings, such as schools. Computers are becoming more accessible to disadvantaged populations,6–8 youths enjoy and are easily engaged by computer-based interventions,9,10 and the delivery of educational material via computer can be far more effective than traditional methods of instruction.10–12 Computerized interventions offer a vehicle to reach youths easily, free the intervention from reliance on the teacher, and maintain fidelity. As a result of these successes, computer-based interventions have been widely advocated in the fields of health education and prevention.13–17 We tested the hypothesis that a computerized version of Project LIGHT would be as efficacious as the interpersonal, small-group delivery of the intervention in reducing the sexual risk behaviors of delinquent youths.
METHODS
Participants
Students aged 14 to 18 years attending 3 alternative education schools were recruited and assessed at baseline and 3 months. These students had been unsuccessful in a mainstream school setting and were at risk for becoming involved with or were currently involved with the juvenile justice system. Participants were paid $25 for completing the 1.5-hour baseline and 3-month follow-up assessments. This compensation level is standard for this type of research with adolescents.5,9,13 A total of 219 students were approached. Of those approached, 18 (8%) declined participation, and 68 (31%) did not complete parental consent. Consequently, 133 students (61%) were enrolled in the study.
Measures
The primary outcome was sexual behavior4: that is, whether the student had sexual intercourse (0=no; 1=yes) in the previous 3 months and the type of sexual activity the student had in the past 3 months (number and sex of sexual partners, occasions, types of acts, and frequency of condom use).
Students self-reported demographic variables (Table 1 ▶), including age, gender, race/ethnicity, living situation, criminal behavior, and substance use.4
TABLE 1—
Sexual Behavior of High-Risk Adolescents in 3 Intervention Conditions: Demographic Variables at Baseline
| Control Group (n = 38), % | Computer Group (n = 38), % | Small Group (n = 31), % | Overall (N = 107), % | P | |
| Mean age (SD) | 15.6 (1.3) | 16.4 (1.0) | 16.2 (1.5) | 16.0 (1.3) | .03 |
| Gender | .36 | ||||
| Female | 53 | 45 | 36 | 45 | |
| Male | 47 | 55 | 65 | 55 | |
| Race/Ethnicity | .07 | ||||
| Black | 61 | 34 | 52 | 49 | |
| Latino | 32 | 63 | 45 | 47 | |
| Other | 8 | 3 | 3 | 5 | |
| Financial situation | .01 | ||||
| Very poor or poor | 0 | 11 | 10 | 7 | |
| Have necessities | 5 | 5 | 26 | 11 | |
| Comfortable | 95 | 84 | 65 | 82 | |
| Living situation | .24 | ||||
| With parents | 71 | 84 | 84 | 79 | |
| With other relatives | 13 | 13 | 13 | 13 | |
| In a group home | 11 | 0 | 0 | 4 | |
| Other | 15 | 3 | 3 | 4 | |
| Lifetime criminal behavior | |||||
| Arrested | 39 | 42 | 84 | 52 | < .01 |
| Time in jail | 16 | 26 | 23 | 22 | .53 |
| Time in juvenile hall | 29 | 26 | 77 | 42 | < .01 |
| Currently on probation | 26 | 29 | 74 | 41 | < .01 |
| Substance use | |||||
| Alcohol | 61 | 71 | 74 | 68 | .83 |
| Marijuana | 50 | 47 | 55 | 51 | .88 |
| Hard drugs | 21 | 29 | 19 | 23 | .63 |
Statistical Methods
To examine the intervention effect on sexual behavior from baseline to 3 months, logistic, linear, and Poisson random-effects regression models were fit to binomial, continuous, and count outcomes, respectively. Regression models included covariates for time (measured in months), assigned intervention condition, and a 2-way time-by-intervention interaction. Models also included person-level random effects to account for correlation between repeated measurements at baseline and 3 months. All models were fit in the SAS Proc Mixed procedure (SAS Institute Inc, Cary, NC) for continuous data and SAS GLIMMIX macro for discrete outcomes.
RESULTS
After we adjusted for baseline differences, we found varying rates of behavior change across intervention conditions from baseline to 3 months on sexual activity rates (F2,104 = 3.11; P=.05) and the number of sexual partners (F2,104 = 3.90; P =.02). Adolescents in the computer-based condition were less likely to engage in sexual activity (t104 = 2.43; P =.02) compared with those in the small-group condition over time (Figure 1 ▶). Adolescents in the computer-based (t104 = 2.67; P <.01) and small-group (t104 = 2.15; P =.03) conditions had fewer sexual partners than did those in the control condition over time. Although the results were not significant, the computer-based condition reported reductions in the percentage of unprotected sexual intercourse, whereas the control and small-group conditions reported increases in unprotected sexual intercourse.
FIGURE 1—
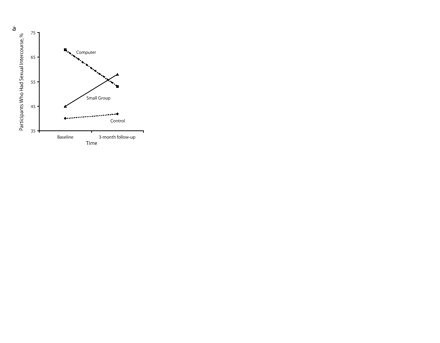
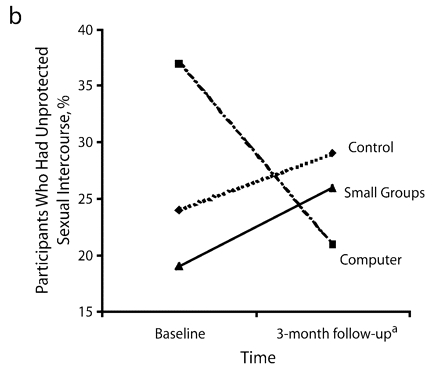
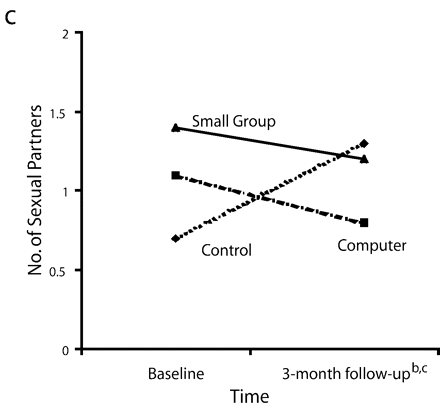
Sexual behavior outcomes: baseline and follow-up comparisons of (a) percentage of students who had sexual intercourse, (b) percentage of the students who had unprotected sexual intercourse, and (c) number of sexual partners.
aSmall group vs computer group difference.
bComputer group vs control group difference.
cSmall group vs control group difference.
CONCLUSIONS
Some youths may require the traditional in-person, therapist-led format to reduce sexual risk behaviors successfully. However, this study suggested that for youths who are outside mainstream schools and who may respond poorly to didactic instruction, computers are a viable way to deliver prevention information and promote skill development.15 Computer-assisted instruction has been used to treat phobias, depression, obesity, eating disorders, and diabetes18–23 yet is rarely used in HIV prevention. Our results support the use of computers as a tool for HIV prevention. Youths receiving the computerized intervention were successful in reducing their sexual risk behaviors.
A limitation of the current study was the use of self-report data. To ensure veracity of reports, assessments used audio computer-assisted interviewing. Previous research indicates that risky behaviors are more likely to be reported by adolescents when this technique is used.24–29 This research was limited by the small sample size and short follow-up period. Randomized controlled trials with larger sample sizes that follow students longitudinally for a longer time are needed to explore fully the potential of using technology for engaging youths in prevention activities.
Several interventions have successfully reduced the HIV transmission risk behaviors of adolescents.30 However, these interventions face challenges in implementation in real-world settings. The design of future interventions must acknowledge the need for accessible and sustainable programs. Computerized interventions, which are relatively easy to implement and sustain, appear to be a potentially effective means of promoting reductions in HIV-related sexual risk behaviors. This program was implemented in schools, increasing the likelihood of access for youths who are often difficult to reach, particularly minorities. Furthermore, interactive computer programs may help youths learn skills to prevent HIV infection and instill in these youths the self-efficacy to apply these new skills. This is particularly important given the probable cost-effectiveness and ease in dissemination and use of computerized programs.
Acknowledgments
This research was supported by the National Institute of Mental Health to M. Lightfoot (grant R21 MH062272).
The authors would like to thank the students and teachers for their generous participation in this research.
Human Participant Protection This study was approved by University of California’s institutional review board.
Peer Reviewed
Contributors M. Lightfoot supervised all aspects of the intervention study and served as lead writer. W. Scott Comulada performed the statistical analyses for the study. G. Stover was project director for the intervention study and assisted with writing.
References
- 1.DiClemente RJ, Lanier M, Horan P, Lodico M. Comparison of AIDS knowledge, attitudes, and behaviors among incarcerated adolescents and a public school sample in San Francisco. Am J Public Health. 1991;81:628–630. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Nader PR, Wexler DB, Patterson TL, McKusick L, Coates T. Comparison of beliefs about AIDS among urban, suburban, incarcerated, and gay adolescents. J Adolesc Health. 1989;10:413–418. [DOI] [PubMed] [Google Scholar]
- 3.Morris RE, Harrison EA, Knox GW, Tromanhauser E, Marquis DK, Watts LL. Health risk behavioral survey from 39 juvenile correctional facilities in the United States. J Adolesc Health. 1995;17:334–344. [DOI] [PubMed] [Google Scholar]
- 4.The National Institute of Mental Health (NIMH) Multisite HIV Prevention Trial Group. The NIMH Multisite HIV Prevention Trial: reducing HIV sexual risk behavior. Science. 1998;280:1889–1894. [DOI] [PubMed] [Google Scholar]
- 5.Rotheram-Borus MJ, Murphy DA, Fernandez I, Srinivasan S. A brief HIV intervention for adolescents and young adults. Am J Orthopsychiatry. 1998;68: 553–564. [DOI] [PubMed] [Google Scholar]
- 6.US Dept of Commerce. Falling through the net: toward digital inclusion. A report on Americans’ access to technology tools. Available at: http://www.ntia.doc.gov/ntiahome/fttn00/falling.htm#1. Accessed March 8, 2004.
- 7.Shriver J Jr. Survey finds 1 in 3 homes has a computer; poll: responses show the gender gap in PC use has narrowed, but education and income are pronounced factors in the increased demand for information technology. Los Angeles Times. May 24, 1994; Business Section:D1.
- 8.Sanchez R. Poor, minority students lack access to computers: report also suggests that few teachers are trained to use PCs as learning tools. Washington Post. May 15, 1997:A13.11647160
- 9.Paperny DM. Computerized health assessment and education for adolescent HIV and STD prevention in health care settings and schools. Health Educ Behav. 1997;24:54–70. [DOI] [PubMed] [Google Scholar]
- 10.Meier ST. Alcohol education through computer-assisted instruction. J Couns Dev. 1988;66:389–390. [Google Scholar]
- 11.Soe K, Koki S, Chang JM. Effect of computer-assisted instruction (CAI) on reading achievement: a meta-analysis. Available at: http://www.prel.org/products/Products/effect-cai.htm. Accessed May 31, 2005.
- 12.Thompson AD, Simonson MR, Hargrave CP. Educational Technology: A Review of the Research. 2nd ed. Washington, DC: Association for Educational Communications and Technology; 1996.
- 13.Schinke SP, Di Noia J, Glassman JR. Computer-mediated intervention to prevent drug abuse and violence among high-risk youth. Addict Behav. 2004;29: 225–229. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Burnett KF, Magel PE, Harrington S, Taylor CB. Computer assisted behavioral health counselling for high school students. J Couns Psychol. 1989;36:63–67. [Google Scholar]
- 15.Orlandi MA, Dozier CE, Marta MA. Computer-assisted strategies for substance abuse prevention: opportunities and barriers. J Consult Clin Psychol. 1990; 58:425–431. [DOI] [PubMed] [Google Scholar]
- 16.Sampson JP, Kruboltz JD. Computer assisted instruction: a missing link in counseling. J Couns Dev. 1991;69:395–397. [Google Scholar]
- 17.Schinke SP, Orlandi MA, Gordon AN, Weston RE, Moncher MS, Parms CA. AIDS prevention via computer-based intervention. Comput Hum Serv. 1990;5:147–156. [Google Scholar]
- 18.Agras WS, Taylor CB, Feldman DE, Losch M, Burnett K. Developing computer assisted therapy for the treatment of obesity. Behav Ther. 1990;21:99–109. [Google Scholar]
- 19.Andrewes DG, O’Connor R, Mulder C, McLennan HD, Weigall S, Sy S. Computerised psychoeducation for patients with eating disorders. Aust N Z J Psychiatry. 1996;30:492–497. [DOI] [PubMed] [Google Scholar]
- 20.Glasgow RE, Toobert DJ, Hampson SE, Noell JW. A brief office-based intervention to facilitate diabetes dietary self-management. Health Educ Res. 1995;10: 467–478. [DOI] [PubMed] [Google Scholar]
- 21.Gosh A, Greist JH. Computer treatment in psychiatry. Psychiatr Ann. 1988;18:246–250. [Google Scholar]
- 22.Gosh A, Marks IM. Self-treatment of agoraphobia by exposure. Behav Ther. 1987;18:3–16. [Google Scholar]
- 23.Selmi PM, Klein MH, Greist JH, Sorrell SP, Erdman HP. Computer-administered cognitive-behavioral therapy for depression. Am J Psychiatry. 1990;147: 51–56. [DOI] [PubMed] [Google Scholar]
- 24.Burnett KF, Magel PE, Harrington S, Taylor CB. Computer assisted behavioral health counseling for high school students. J Consult Clin Psychol. 1989;36: 63–67. [Google Scholar]
- 25.Jones EF, Forrest JD. Underreporting of abortion in surveys of U.S. women: 1976 to 1988. Demography. 1992;29:113–127. [PubMed] [Google Scholar]
- 26.Tourangeau R, Smith TW. Asking sensitive questions: the impact of data collection mode, question format, and question context. Public Opin Q. 1996;60: 275–304. [Google Scholar]
- 27.Turner CF, Ku L, Rogers SM, Lindberg LD, Pleck JH, Sonenstein FL. Adolescent sexual behavior, drug use, and violence: increased reporting with computer survey technology. Science. 1998;280:867–873. [DOI] [PubMed] [Google Scholar]
- 28.Turner CF, Danella RD, Rogers SM. Sexual behavior in the United States 1930–1990: trends and methodological problems. Sex Transm Dis. 1995;22: 173–190. [DOI] [PubMed] [Google Scholar]
- 29.Turner CF, Lessler JT, Devore J. Effects of mode of administration and wording on reporting of drug use. In: Turner CF, Lessler JC, Gfroerer JC, eds. Survey Measurement of Drug Use: Methodological Issues. Washington, DC: Government Printing Office; 1992: 77–220.
- 30.Rotheram-Borus MJ, O’Keefe Z, Kracker R, Foo HH. Prevention of HIV among adolescents. Prev Sci. 2000; 1:15–30. [DOI] [PubMed] [Google Scholar]