

Abstract
This article reports recent findings from a program of experimental research examining the effects of adapting judicial supervision to the risk level of drug-abusing offenders. Prior studies revealed that high-risk participants with (1) antisocial personality disorder or (2) a history of drug abuse treatment performed significantly better in drug court when they were scheduled to attend frequent, bi-weekly judicial status hearings in court. Low-risk participants performed equivalently regardless of the schedule of court hearings. The current study prospectively matched misdemeanor drug court clients to the optimal schedule of court hearings based upon an assessment of their risk status, and compared outcomes to those of clients randomly assigned to the standard schedule of court hearings. Results confirmed that high-risk participants graduated at a higher rate, provided more drug-negative urine specimens at 6 months post-admission, and reported significantly less drug use and alcohol intoxication at 6 months post-admission when they were matched to bi-weekly hearings as compared to the usual schedule of hearings. These findings yield practical information for enhancing the efficacy and cost-efficiency of drug court services. Directions for future research on adaptive programming for drug offenders are discussed.
Keywords: Adaptive intervention, Drug court, Crime, Criminal justice, Antisocial personality disorder
1. Introduction
1.1. Adaptive interventions for offenders
Adaptive interventions adjust the dosage and type of services that are administered to clients in response to clients’ clinical presentation or performance in treatment (e.g., Collins et al., 2004; Murphy, 2005). Matching services to clients’ pretreatment characteristics is perhaps the simplest form of adapting treatment to the needs of the individual. For example, tailoring services to the specific needs of females, youths, or minorities is a basic approach to adapting treatment for the client. Similarly, a history of negative outcomes in previous treatment episodes might lead a program to prescribe a higher dosage or greater variety of services for a new client than would ordinarily be provided to new admissions. This, too, is a simple form of adapting treatment to the needs of the individual.
At a more sophisticated level of adaptive programming, the nature and intensity of services is continuously re-adjusted as a consequence of the client’s ongoing performance in treatment. For example, if a client fell below an effective threshold for engagement in treatment (by, for example, missing a predetermined number of scheduled counseling appointments), he or she might be re-assigned to a motivational-enhancement intervention or might be encouraged to try a different and more desired form of treatment. The term “matching” is commonly used to describe strategies that tailor treatment to clients’ baseline characteristics whereas the term “adaptive” is commonly used for strategies that continually re-adjust the interventions during the course of treatment. Conceptually, therefore, matching strategies are a subset of adaptive strategies.
This article reports outcomes from a program of experimental research aimed at adapting judicial supervision to the risk level of drug-abusing offenders. According to the criminological paradigm of the “risk principle,” intensive interventions are theorized to exert the greatest effects for high-risk offenders who have more severe antisocial propensities or drug-use histories, but may be ineffective or contraindicated for low-risk offenders (Andrews and Bonta, 1998; Taxman and Marlowe, 2006). The rationale is that low-risk offenders are less likely to be on a fixed antisocial trajectory and are apt to “adjust course” following a run-in with the law. Therefore, intensive treatment and supervision may offer little incremental benefit at a substantial cost (e.g., DeMatteo et al., 2006). In contrast, high-risk offenders are likely to require intensive interventions to dislodge their entrenched behavioral patterns.
Among drug-abusing offenders, the greatest risk factors for failure in rehabilitation include (1) being younger, (2) being male, (3) an earlier onset of crime or drug abuse, (4) multiple prior criminal arrests, (5) a co-morbid diagnosis of antisocial personality disorder (APD) or psychopathy, or (6) having previously failed in treatment (e.g., Gendreau et al., 1996; Marlowe et al., 2003a; Peters et al., 1999). It is unclear, however, whether these risk factors simply correlate with treatment outcomes or whether they moderate the effects of specific types of interventions. For example, although a younger age during treatment reliably predicts poorer performance in correctional rehabilitation, this finding yields little practical information about how to intervene effectively with youthful offenders. If it were shown that younger offenders performed better in treatment when they were closely supervised by criminal justice authorities, this finding would yield practical information for treatment planning.
1.2. The risk principle in drug courts
Drug courts represent one of the most intensive community-based programs for offenders with drug problems. Drug courts are special criminal court dockets that administer a judicially supervised regimen of treatment and case management services in lieu of prosecution or incarceration. Participants are required to satisfy a range of obligations, including attending routine status hearings in court, completing a standard sequence of counseling sessions, providing random weekly urine samples, and receiving progressively escalating negative sanctions for infractions and positive rewards for achievements (National Association of Drug Court Professionals, 1997).
Substantial evidence from experimental and quas-iexperimental studies reveals that drug courts can significantly increase treatment retention and reduce substance use, crime, and unemployment while participants are enrolled in the program, and can reduce criminal recidivism for 2-3 years post-admission (US Government Accountability Office, 2005). Few studies, however, have isolated the effects of specific components of the drug court model or determined whether such an intensive regimen is necessary for all drug offenders (Goldkamp, 2001; Marlowe et al., 2003b). It might be most effective or cost-efficient to reserve drug courts for high-risk offenders and assign low-risk individuals to less intensive and less costly probation or pre-trial monitoring programs. Alternatively, it might be advisable to refer most or all drug offenders to drug court programs, but to assign them to different “service tracks” within the drug court based upon an assessment of their risk status and clinical needs. This would permit staff to transfer clients between tracks within drug courts or to adapt the service requirements as a consequence of clients’ ongoing conduct in the program.
Judicial status hearings are among the most expensive and time consuming components of drug courts (e.g., Finigan, 1999). Apart from their obvious cost implications, some commentators have suggested that the intrusion of a judge into the treatment process could be disruptive or harmful to the therapeutic alliance (e.g., Schottenfeld, 1989). Clients may be hesitant to confide important information to their counselors for fear the information would be disclosed to the court and used against their legal interests. Moreover, being “treated like a criminal” by being brought into court on a regular basis might elicit counterproductive feelings of resistance or reactance. Under such circumstances, judicial monitoring could both waste scarce resources and elicit iatrogenic effects. On the other hand, high-risk offenders often fail to meet their obligations and may pose a continuing threat to public safety if they are not closely monitored and do not face immediate and consistent consequences for noncompliance in treatment (e.g., Marlowe and Kirby, 1999; Satel, 1999). It is important to determine which drug offenders require intensive monitoring by a judge and which ones can be adequately supervised by clinicians, case managers or probation officers.
1.3. Current program of research
Beginning in 1999, we initiated a planned sequence of experimental studies to determine whether the effects of judicial status hearings in drug courts are moderated by client characteristics in accordance with the risk principle. In the first study, consenting participants in a misdemeanor drug court were randomly assigned to attend status hearings on a bi-weekly basis throughout their enrollment in the program (“bi-weekly” condition) or to be monitored by their treatment case managers who petitioned the drug court for status hearings only as needed in response to serious or repeated infractions (“as-needed” condition). The results revealed no main effects of status hearings on counseling attendance, substance use or criminal activity during participants’ enrollment in drug court (Marlowe et al., 2003c), in graduation rates (Festinger et al., 2002), or in substance use, criminal activity, or psychosocial functioning at 12 months post-admission (Marlowe et al., 2005). Importantly, however, planned interaction analyses confirmed that high-risk participants who (1) met DSM-IV diagnostic criteria for APD or (2) had a history of drug abuse treatment provided more drug-negative urine specimens and were more likely to graduate when they were assigned to bi-weekly hearings (Festinger et al., 2002). Presumably, the prior treatments were relatively unsuccessful for these individuals, given that they were subsequently arrested for a drug crime.
We replicated several of these interaction effects using the same research design in two new jurisdictions located in rural and urban communities and serving misdemeanor and felony offenders. Specifically, misdemeanor participants with a drug treatment history provided more drug-negative urine samples during the first 14 weeks of drug court when they were assigned to bi-weekly status hearings as opposed to as-needed hearings (Marlowe et al., 2003d). Similarly, felony participants with APD reported engaging in significantly more alcohol intoxication when they were assigned to as-needed hearings as compared to bi-weekly hearings (Marlowe et al., 2004).
The current study brought these interaction effects under experimental control. The aim was to match high-risk participants to bi-weekly judicial status hearings and match low-risk participants to as-needed hearings, and to compare their outcomes to those of participants randomly assigned to the standard schedule of hearings. In a prior article (Marlowe et al., 2006), we reported results from urine screens and structured interviews during the first 14 weeks of the program. Results confirmed that high-risk participants had significantly better during-treatment outcomes when they were matched to bi-weekly hearings. The current article reports discharge and 6-month outcomes on a larger cohort.
2. Methods
2.1. Human subjects protections
This study was approved and monitored by the Institutional Review Boards (IRBs) of the Treatment Research Institute and the Delaware State Department of Health and Social Services. A DHHS Confidentiality Certificate was obtained, which shielded the research data from a court order or subpoena. Monthly oversight meetings were held for the study that were regularly attended by the drug court judge and by representatives of the attorney general’s office, public defender’s office, criminal defense bar, substance abuse treatment program, and the State Division of Substance Abuse and Mental Health. In these meetings, we reviewed the study procedures and were prepared to correct any untoward reactions that might have been experienced by research participants or project staff. No study-related adverse event was reported to date. The presence of defense counsel and treatment providers ensured that participants’ legal rights and clinical needs were continuously addressed.
2.2. Recruitment
Consecutive admissions to a misdemeanor drug court located in Wilmington, DE were approached about participation over a 33-month recruitment interval (November 2002-July 2005). Defendants in this drug court were charged with possession or consumption of cannabis, possession of drug paraphernalia, possession of hypodermic syringes, or driving under the influence (DUI) and could not have a history of a violent offense involving serious injury to a victim or use of a deadly weapon. The drug court has jurisdiction over offenders who are at least 18 years of age and who are a resident of New Castle County, DE or committed their offense in New Castle County.
Upon entry into the drug court, the judge routinely ordered defendants to report to a specific treatment program, which handles all misdemeanor drug court cases in that county, on a specified date the following week for an intake appointment. If the defendant did not arrive for the appointment or reschedule within 24 h, a bench warrant was issued for his or her arrest. At the treatment program, following a group orientation session conducted by clinical staff, a research staff member provided a brief oral description of the study, including participation requirements, payment incentives, confidentiality protections, and the right to refuse or withdraw from the study at any time without negative consequences. Defendants who indicated a potential interest in the study went through a formal, individualized informed consent procedure that was approved by the IRBs.
Ninety-three percent of individuals who entered the drug court arrived at the treatment program for their intake appointment (i.e., 7% absconded or were re-arrested prior to intake). Of those who arrived for an intake, we were able to approach 96% about potential participation in the study. Eleven defendants were unable to consent to the study due to a language barrier or severe psychiatric impairment and were not included in the calculation of the consent rate. Thirty-nine percent of eligible defendants consented to participate in the study and 61% refused to participate. This recruitment rate was anticipated given that the defendants were being asked to potentially increase the number of times they would be required to appear in court before a judge. The baseline cohort was predominantly male (75%), Caucasian (60%) or African American (35%), unmarried (94%), young adult (M = 25.13, S.D. = 8.36 years), high school educated (M = 11.31, S.D. = 1.65 years), and employed (66%). The participants reported currently abusing cannabis (68%), alcohol to intoxication (47%), stimulants or cocaine (14%), opiates (13%), sedatives (5%), or hallucinogens (3%).
To monitor selection bias in the sample, demographic information and baseline assessment data and criminal records were obtained on a randomly selected sample of 252 defendants who declined to participate in the research study. These data were received in aggregate batches from the treatment program and were purged of client-identifying information. There were no differences between individuals who consented to participate in the study and those who refused to participate in terms of current criminal charge(s), age, race, marital status, education, employment, legal problems, family/social problems, medical problems, or psychiatric problems. However, females consented to participate at a higher rate than males, X2(d.f. = 1) = 13.54, p < 0.0001. In addition, individuals who consented to participate reported significantly more days of drug problems in the previous 30 days, t(516) = 1.96, p < 0.05, and had significantly fewer prior criminal convictions, t(516) = 3.45, p = 0.001. This suggests that females were over-represented in the study sample and individuals with more severe drug problems and less severe criminal histories were more likely to have participated.
2.3. Brief description of the drug court program
In this pre-adjudication drug court, defendants are required to plead guilty to the initial charge(s) and the guilty plea is held in abeyance pending graduation or termination from the program. Successful graduates have their criminal charges formally dropped and are eligible to have their original arrest record expunged if they remain arrest-free for an additional 6 months. Record expungement ordinarily entitles the individual to respond truthfully on an employment application or similar document that he or she was not arrested for a drug offense (e.g.,Festinger et al., 2005). If the defendant fails to complete the program, the guilty plea is formally entered as a conviction. This can have serious consequences for such matters as employment or government subsidies and the offender loses his or her driver’s license for a term of 2 years. Convicted offenders are typically sentenced to probation in the community with conditions similar to those of drug court (e.g., drug abuse counseling and urine monitoring). Therefore, dropping out of the drug court does not necessarily result in lesser treatment or supervisory obligations.
The drug court program is scheduled to be a minimum of 14 weeks in length; however, clients require an average of approximately 9 months to satisfy all of the conditions for graduation and virtually all clients graduate within 12 months if they graduate at all. The minimum requirements for graduation include attending at least 12 weekly group-counseling sessions, providing at least 14 consecutive weekly drug-negative urine specimens, remaining arrest-free, obeying program rules and procedures, and paying a $200 court fee. The group sessions are psycho-educational in format and cover a standard sequence of topics, including the pharmacology of drug and alcohol use, progression from substance use to dependence, the impact of addiction on the family, treatment options, HIV/AIDS risk reduction, and relapse prevention strategies.
Participants are also assigned to a clinical case manager who coordinates any indicated treatment referrals and the case manager or a court liaison submits monthly progress reports to the judge and appears at all status hearings. Participants provide urine specimens on a random, weekly basis in direct observation of a same-gender treatment staff person. The urine drug screens are performed by an independent certified laboratory using the enzyme multiplied immunoassay technique (EMIT) with gas chromatography/mass spectrometry (GC/MS) confirmation of positive results on a five-panel screen for cannabis, opiates, amphetamines, cocaine, and phencyclidine (PCP). Finally, the judge is authorized to administer sanctions or remedial interventions to participants for poor performance. These include verbal reprimands, written homework assignments, additional treatment or supervisory obligations, daylong attendance in court as an observer, or community service. The judge or treatment team may also administer rewards for good performance, including verbal praise, token gifts, certificates of recognition, and reductions in treatment or supervisory obligations.
2.4. Adaptive research design
The adaptive research design is depicted in Fig. 1. Consenting participants were randomly assigned at intake to be matched (n = 137) or unmatched (n = 142). Unmatched participants were scheduled to attend judicial status hearings every 4-6 weeks, which is standard practice for this drug court program. Matched participants were scheduled either to attend bi-weekly judicial status hearings or as-needed hearings depending upon whether they met criteria for APD or had a drug treatment history. Thus, high-risk participants who were matched to bi-weekly hearings were required to attend more status hearings than participants in the unmatched control condition, and low-risk participants who were matched to as-needed hearings were required to attend fewer hearings than participants in the non-matched control condition. The base rate for high risk in the sample was 33%; therefore, a greater proportion of matched participants were assigned to as-needed hearings.
Fig. 1.
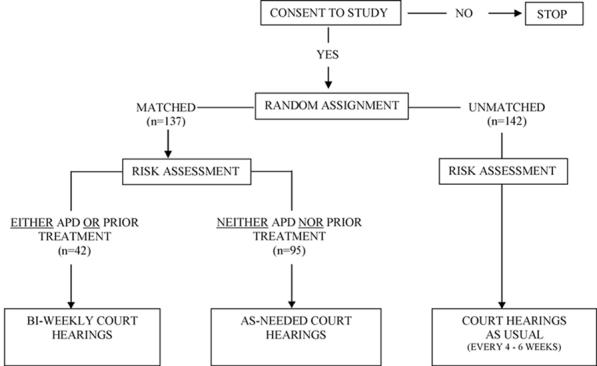
Adaptive research design.
The a priori decision rule for assessing risk level was derived from two dichotomous measures that were employed on an either/or basis. If participants either met DSM-IV-R criteria for APD (yes or no) or had a history of at least one prior drug abuse treatment episode (yes or no), they were determined to be high risk. If they had neither APD nor a prior treatment episode, they were determined to be low risk. The instruments used to make these assessments are described below.
If a participant revoked consent after initially agreeing to participate in the study, he or she was re-assigned to the standard schedule of status hearings, which, as noted, is every 4-6 weeks. One participant who was assigned to the unmatched condition (<1%) and 10 participants (7%) assigned to the matched condition elected to drop out of the study. This left a final cohort for outcome analyses of 268 participants (see Table 1). The 10 participants who dropped out of the matched condition had all been assigned to bi-weekly status hearings. As a result, there was 24% attrition from the matched bi-weekly cell. This differential attrition was not surprising, given that bi-weekly hearings place substantially more onerous time demands on participants, and the participants who were assigned to bi-weekly hearings tended to have the most serious antisocial predispositions or drug-use histories.
Table 1.
Flow of participants in the study
| Low risk |
High risk |
Total | |||
|---|---|---|---|---|---|
| Matched | Unmatched | Matched | Unmatched | ||
| Randomly assigned at baseline | 95 | 92 | 42 | 50 | 279 |
| Dropped out of study | -0 | -1 | -10 | -0 | -11 |
| Remained in assigned condition and eligible for follow-up (% of original sample) | 95 (100%) | 91 (99%) | 32 (76%) | 50 (100%) | 268 (96%) |
| Completed 6-month follow-up ASI (% of eligible sample) | 75 (79%) | 79 (87%) | 27 (84%) | 38 (76%) | 219 (82%) |
| Provided 6-month urine specimen (% of eligible sample) | 34 (36%) | 33 (36%) | 12 (37%) | 14 (28%) | 93 (35%) |
The relatively small number of dropouts limited our statistical power for detecting attrition bias. However, we compared the dropouts to the remainder of the high-risk participants on a range of demographic variables (age, race, gender, marital status, education, employment), current criminal charges, criminal history (prior convictions and incarcerations), and problem severity-ratings from their baseline assessments. We set a liberal p-value of p < 0.15 to detect attrition bias due to the small cell sizes for these analyses. Results indicated that the dropouts did not differ from the remainder of the high-risk participants on any of these baseline characteristics. Regardless, it is possible that high-risk participants who were performing poorly in the drug court program might have dropped out of the bi-weekly condition at a relatively higher rate to reduce the likelihood that the judge would detect their infractions. Thus, it is possible that the results could have over-estimated positive outcomes for the matched bi-weekly participants.
As noted previously, monthly oversight meetings were held for the study, which were regularly attended by the drug court staff members and the research team. After conferring with program staff and the researchers, the judge had the authority to overrule any research assignment. Importantly, there was no instance in which a research assignment was overruled by the court.
2.5. Data sources
Participants were scheduled to complete a battery of structured interviews administered by trained research technicians at baseline, monthly during the first 3 months of drug court, and at 6 and 12 months post-admission to the drug court. We are also monitoring state criminal justice databases for 24 months post admission to assess rates of re-arrests and convictions. An earlier article reported urine drug-screen results, counseling attendance, and self-reported substance use and crime during the first 14 weeks of drug court (Marlowe et al., 2006). The current analyses focus on participants’ discharge status and 6-month follow-up assessments. Future reports will address 12- and 24-month outcomes.
The baseline assessment battery included the addiction severity index (ASI) (McLellan et al., 1992), which assesses current (past 30 days) and lifetime drug problems, alcohol problems, legal problems, medical problems, family and social problems, employment problems, and psychiatric problems. “Composite scores” are calculated from the ASI, which are global indicators of problem-severity in each domain. A lower composite score indicates lesser self-reported problems. The composite scores are based exclusively on events occurring during the preceding 30 days. Multiple examinations of ASI composite scores and lifetime items have yielded impressive evidence of reliability, concurrent validity, predictive validity, and discriminative utility across groups of clients characterized by age, race, gender, and primary drug of abuse (e.g., Alterman et al., 1998; Cacciola et al., 1999; McDermott et al., 1996; McLellan et al., 1980,1985,1992). Additional items were appended to the ASI that assessed participants’ involvement in criminal activities during the preceding 6 months, regardless of whether those activities were detected by authorities or resulted in formal criminal charges. For these items, criminal activity did not include simple drug use or drug possession, but did include drug dealing or manufacturing, property offenses, theft offenses, violent offenses, and weapons offenses.
At baseline, participants also completed an “antisocial personality disorder interview” (APDI) and a “prior treatment questionnaire” (PTQ) for purposes of matching them to the study conditions. The APDI is a 30-item, true/false structured interview modeled after the SCID-II (First et al., 1997) that assesses DSM-IV-R (American Psychiatric Association, 2000) diagnostic criteria for APD. A dichotomous (yes or no) diagnosis of APD generated from this instrument was used as one of the two risk-assessment variables. In inter-rater reliability scoring trials, we had 100% exact agreement for dichotomous diagnoses of APD among our research technicians. A single dichotomized (yes or no) item from the PTQ inquiring whether the participant experienced any prior drug abuse treatment episode was also used to match participants to the study conditions. Inter-rater reliability and test-retest stability for this item were consistently above 95% in prior studies. As noted previously, these two variables were employed in an either/or manner. That is, if participants either met DSM-IV-R criteria for APD or had a history of at least one prior drug abuse treatment episode, they were determined to be high risk. If they had neither APD nor a prior treatment episode, they were determined to be low risk.
Participants were scheduled to complete a confidential, follow-up version of the ASI and provide a urine specimen at 6 months post-admission to the drug court. The follow-up urine drug screens were performed using a handheld device, the Roche Test-Cup 5©, for cannabis, opiates, amphetamines, cocaine, and PCP. Participants received a $40 check for completing the 6-month assessment.
2.6. Follow-up rates and representativeness
Participants were strongly encouraged to complete their follow-up assessments in person at the research office or at a mutually agreeable location in the community. However, due to the reluctance of many of these drug-abusing offenders to return in person for a research appointment, some of the ASIs had to be completed over the telephone after verifying the participant’s identity. Those participants received a partial incentive payment because they did not provide a urine specimen. The 6-month follow-up rate was 82% (n = 219) for the ASIs and 35% (n = 93) for the urine specimens. Thus, although the follow-up rate was good for the ASIs, it is uncertain whether the urine drug-screen results may be expected to generalize to the intent-to-treat cohort. For this reason, statistical analyses on the urine results were conducted both by using only complete cases, and also by using the most conservative approach which assumed all missing urine screens to be drug-positive.
To examine the representativeness of the follow-up samples to the baseline cohort, participants who completed their 6-month follow-up assessments were compared to those who did not on a range of demographic variables (age, race, gender, marital status, education, employment), current criminal charges, criminal history (past convictions and incarcerations), and baseline ASI composite scores. There were no significant differences on these variables between those who completed the 6-month ASI and those who did not. However, participants who provided a 6-month urine specimen had significantly higher ASI drug composite scores at baseline than those who did not provide a urine specimen, t(264) = 2.16, p < 0.05. This suggests that the more drug-involved individuals were more likely to have provided a follow-up urine specimen. It is possible these individuals may have had more time available to attend in-person follow-up appointments because, for example, they may have been less likely to be employed or in school. Alternatively, they might have been in greater need of the research payment incentives.
To determine whether the follow-up samples were equivalently representative across conditions, matched and unmatched participants who completed their 6-month follow-up were compared on the same range of demographic variables, criminal charges, criminal history variables, and ASI composite scores. These analyses were conducted separately for the high-risk and low-risk groups because the study design intended the two risk groups to have different levels of problem-severity at baseline. The results revealed one significant difference. Among those participants who completed a 6-month follow-up, high-risk participants assigned to the matched condition were older than high-risk participants assigned to the unmatched condition, t(63) = 2.33, p < 0.05. Therefore, age was entered as a covariate in the outcome analyses. Given the large number of comparisons that were conducted for this purpose, it is possible this difference was encountered by chance. However, we elected to use the most conservative approach and enter the lone variable of age as a covariate in the models. This would have the effect of reducing type 1 error at the expense of type 2 error.
2.7. Data analyses
Table 1 summarizes the flow of participants in the study accounting for attrition and follow-up rates. Analyses involving graduation rates were performed on the entire eligible cohort at follow-up (n = 268). The remaining analyses were performed on 219 participants who completed a 6-month follow-up ASI or 93 participants who provided a 6-month follow-up urine specimen.
The primary outcome measure for this phase of the study was graduation rates within 12 months of admission to the drug court. As was noted earlier, clients in this drug court require an average of approximately 9 months to satisfy the requirements for graduation and the large majority of clients graduate within 12 months if they graduate at all. Therefore, graduation rates were assessed over a 12-month window. We specified graduation rate as the primary dependent measure because (1) it is objectively measurable, (2) data analyses can be performed on the entire eligible cohort, and (3) it reflects a sum total of multiple performance indicators, including counseling attendance, urine results and compliance with program rules and regulations.
Secondary dependent measures were urine drug-screen results at 6 months post-admission to the drug court and ASI drug composite scores at 6 months post-admission. Finally, tertiary dependent measures included composite scores in the other ASI domains, individual ASI items assessing days of illicit drug use and alcohol intoxication during the preceding 30 days, and ASI items assessing numbers of criminal charges and criminal activities irrespective of detection during the preceding 6 months.
Logistic regression analyses were used to examine effects on the dichotomous outcomes of graduation rates and urine drug-screen results, accounting for the covariate of age. The baseline and 6-month ASI drug composite scores were analyzed via repeated-measures, mixed-effects analysis of variance (ANOVA) using SAS Proc Mixed (Littell et al., 1996), with age entered as a covariate in the model. The models included terms for matching (matched versus unmatched), risk level (high versus low), time (baseline versus 6 months, where applicable), and their interactions. Because the composite scores were not normally distributed, log-transformed scores were used in the analysis. The two-way interaction effect of matching-by-risk and the three-way interaction of matching-by-risk-by-time are of primary relevance to the research hypotheses. The main effects for risk and time and the risk-by-time interaction were also assessed and are reported in the tables; however, they are not discussed in text because they do not address the key study hypotheses.
Additional analyses were performed on other ASI composite scores and selected ASI items. These composite scores and items were not normally distributed; therefore, log-transformed scores were used for the analyses. Changes from baseline to 6 months were assessed using repeated measures, mixed-effects ANOVA for continuous items and generalized estimating equations (GEE) (SAS Institute, 2001) for dichotomous items. GEE analyses can accommodate a dichotomous dependent variable that is assessed longitudinally (Diggle et al., 1994). Age was entered as a covariate in the models and the models included terms for matching, risk, and time as well as their interactions.
3. Results
3.1. Judicial status hearings
A manipulation check confirmed that we maintained strong experimental control over the dosage of judicial status hearings. There were significant differences in the number of status hearings that were attended by participants in the four conditions, F(3,264) = 135.91, p < 0.0001. As intended, high-risk participants who were matched to the bi-weekly condition attended significantly more status hearings (M = 6.31, S.D. = 2.95) than did participants in any of the other conditions. Conversely, low-risk participants who were matched to the as-needed condition attended significantly fewer hearings (M = 0.71, S.D. = 0.85) than participants in the other conditions. Finally, among participants who were assigned to the unmatched condition, there was no difference in the number of status hearings attended by those who were high-risk (M = 2.22, S.D. = 1.07) or low-risk (M = 2.24, S.D. = 1.03).
3.2. Graduation rates
A logistic regression analysis compared the proportions of participants in the four study conditions who graduated within 12 months of entering the drug court. Results revealed a significant matching-by-risk interaction effect, X2(1) = 3.96, p < 0.05. Graduation rates were significantly lower for high-risk participants assigned to the unmatched condition (56%) as compared to high-risk participants assigned to the matched condition (75%) and low-risk participants assigned to either the matched condition (72%) or the unmatched condition (75%) (see Table 2).
Table 2.
Discharge status, substance use, and criminal recidivism by time and condition: percent endorsing or mean (S.D.)
| Variable | Time | Low risk |
High risk |
Total sample | ||
|---|---|---|---|---|---|---|
| Matched | Unmatched | Matched | Unmatched | |||
| Graduation rateM×R | 12 months | 72% | 75% | 75% | 56% | 72% |
| UA drug positiveM×R | 6 months | 50% | 44% | 8% | 64% | 45% |
| UA positive for cannabis only | 6 months | 35% | 36% | 0% | 50% | 33% |
| Days of drug use (past 30 days)T,R | Baseline | 13.53 (15.74) | 10.97 (12.44) | 22.85 (17.12) | 20.66 (16.98) | 15.00 (15.59) |
| 6 months | 4.32 (9.30) | 3.50 (8.41) | 8.00 (11.90) | 9.51 (13.87) | 5.37 (10.47) | |
| Any drug use (past 30 says)T,R | Baseline | 84% | 73% | 85% | 87% | 81% |
| 6 months | 35% | 28% | 56% | 51% | 38% | |
| Only cannabis use (past 30 days)T | Baseline | 63% | 49% | 41% | 39% | 51% |
| 6 months | 23% | 18% | 15% | 27% | 21% | |
| Days of alcohol Intoxication (past 30 days)T,M×T | Baseline | 2.32 (3.12) | 2.44 (4.02) | 3.59 (5.21) | 3.13 (6.04) | 2.66 (4.33) |
| 6 months | 1.30 (2.52) | 2.02 (3.27) | 1.40 (3.27) | 2.67(5.98) | 1.80 (3.68) | |
| Any alcohol intoxication (past 30 days)T,M×T | Baseline | 55% | 46% | 48% | 39% | 48% |
| 6 months | 33% | 45% | 20% | 36% | 36% | |
| Any criminal activity (past 6 months)T,R | Baseline | 8% | 4% | 19% | 29% | 12% |
| 6 months | 4% | 6% | 12% | 6% | 6% | |
| Any criminal charge (past 6 months)T | Baseline | 79% | 69% | 63% | 74% | 72% |
| 6 months | 3% | 4% | 0% | 11% | 4% | |
Notes: Continuous data reflect the non-transformed, non-adjusted means. Alcohol intoxication = consumed five drinks in one day or drank until felt the effects of alcohol. Criminal activity = drug dealing/manufacturing, property offenses, theft offenses, violent offenses, or weapons offenses. All of the reported effects are statistically significant with p-values of <0.05 or lower. Superscripts in bold font are directly relevant to the study hypotheses. T: main effect of time. R: Main effect of risk level. M: main effect of matching. M×R: interaction effect of matching-by-risk. M×T: interaction effect of matching-by-time.
3.3. Urine drug-screen results
Urine drug-screen results at 6 months post-admission are also presented in Table 2. A logistic regression analysis revealed a significant matching-by-risk interaction effect, X2(1) = 4.30, p < 0.05. High-risk participants were more likely to provide a drug-positive urine specimen if they were assigned to the unmatched condition (64%) as compared to the matched condition (8%). Table 2 further separates out cannabis use when not used in combination with other drugs. Disaggregating the data for cannabis in no way reflects a value judgment about the clinical or legal seriousness of cannabis ingestion. Practitioners and policymakers frequently inquire about the proportion of drug use that reflects cannabis ingestion. As can be seen from the table, a substantial proportion of positive urine tests for all participants were attributable to cannabis metabolites alone.
As mentioned previously, due to the low follow-up rate for the urine screens (35%), we conducted a further analysis coding missing urine specimens as drug-positive for all participants who were eligible for a follow-up (n = 268). This is the most conservative approach and provides an upper limit estimate of the influence of client-matching on drug use. The results mirrored those of the former analysis, with a significant matching-by-risk interaction effect, X(1) = 5.15, p < 0.02. High-risk participants were more likely to provide a drug-positive urine specimen when counting missing specimens as positive if they were assigned to the unmatched condition (90%) as compared to the matched condition (66%). Low-risk participants did not differ in the likelihood of providing a drug-positive urine specimen whether they were assigned to the matched condition (82%) or the unmatched condition (80%).
3.4. ASI drug composite scores
Table 3 presents ASI composite scores for each condition at baseline and 6-month follow-up. The analyses were performed on log-transformed scores; however, the non-adjusted means and standard deviations are reported in the table. Results of a repeated-measures ANOVA revealed a trend towards a matching-by-risk-by-time interaction effect on the drug composite score, F(1,204) = 3.38, p = 0.07. Given the complexity of the statistical model, which examined a three-way interaction plus a covariate, this trend is noteworthy and arguably interpretable.
Table 3.
Addiction severity index (ASI) composite scores by time and condition: mean (S.D.)
| ASI domain | Time | Low risk |
High Risk |
||
|---|---|---|---|---|---|
| Matched | Unmatched | Matched | Unmatched | ||
| DrugT,R,M×R×T | Baseline | 0.08 (0.09) | 0.08 (0.09) | 0.14 (0.12) | 0.11 (0.11) |
| 6 months | 0.04 (0.07) | 0.02 (0.06) | 0.06 (0.07) | 0.07 (0.09) | |
| AlcoholT | Baseline | 0.09 (0.10) | 0.10 (0.11) | 0.09 (0.12) | 0.08 (0.10) |
| 6 months | 0.06 (0.09) | 0.06 (0.08) | 0.06 (0.11) | 0.08 (0.16) | |
| LegalT | Baseline | 0.12 (0.10) | 0.13 (0.11) | 0.19 (0.15) | 0.23 (0.20) |
| 6 months | 0.08 (0.11) | 0.09 (0.12) | 0.09 (0.14) | 0.13 (0.15) | |
| PsychiatricR | Baseline | 0.09 (0.14) | 0.07 (0.14) | 0.15 (0.24) | 0.19 (0.23) |
| 6 months | 0.07 (0.15) | 0.07 (0.15) | 0.13 (0.21) | 0.18 (0.24) | |
| EmploymentR | Baseline | 0.42 (0.30) | 0.34 (0.26) | 0.58 (0.34) | 0.53 (0.27) |
| 6 months | 0.43 (0.32) | 0.30 (0.28) | 0.54 (0.32) | 0.51 (0.33) | |
| FamilyT,M×T,R,R × T | Baseline | 0.04 (0.11) | 0.04 (0.10) | 0.11 (0.15) | 0.10 (0.17) |
| 6 months | 0.03 (0.09) | 0.05 (0.09) | 0.02 (0.06) | 0.06 (0.14) | |
| MedicalT | Baseline | 0.17 (0.29) | 0.10 (0.22) | 0.20 (0.29) | 0.16 (0.24) |
| 6 months | 0.08 (0.23) | 0.07 (0.17) | 0.13 (0.31) | 0.08 (0.20) | |
Notes: Statistical analyses were conducted on log-transformed scores; however, the data presented in the table reflect the non-transformed, non-adjusted means. Composite scores range from 0.00 to 1.00. Lower scores indicate less self-reported problems. All of the reported effects are statistically significant. Superscripts in bold font are directly relevant to the study hypotheses. T: main effect of time: p < 0.001. R: main effect of risk: p < 0.05. M × T: interaction effect of matching-by-time: p < 0.05. R × T: interaction effect of risk-by-time: p < 0.01. M × R × T: interaction effect of matching-by-risk-by-time: p = 0.07.
Because the significance of the model could have been influenced by a lack of fit of the regression, we empirically examined the fit of the model. Given that there are only two time points, the measured effects could only be linear. We examined influence diagnostics and determined there were no overly influential data points. We also conducted a residual analysis of the observed and predicted values of the scores and the residuals were small and there were no obvious patterns in the residual plots. For these reasons, the model fit appears to be adequate and the analysis was retained for reporting.
To assist with interpretation of the three-way interaction, ASI drug composite scores are depicted in Fig. 2 by condition and time of assessment. The log-transformed adjusted means are depicted to best illustrate the nature of the effect. The scores declined for participants in all conditions from baseline to 6 months, revealing a main effect for time. In addition, participants in the two high-risk cells had more severe drug problems than the low-risk participants, revealing an expected main effect for risk level. Finally, the drug composite score declined more readily for high-risk participants assigned to bi-weekly status hearings as compared to high-risk participants assigned to the usual schedule of court hearings, reflecting a marginal trend towards a three-way interaction (p = 0.07).
Fig. 2.
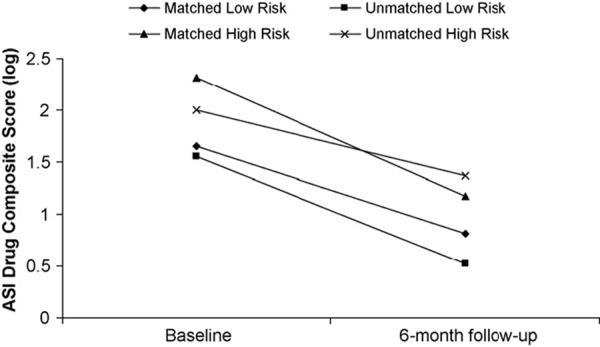
Addiction severity index (ASI) drug composite scores at baseline and 6 months post-admission for misdemeanor drug court participants assigned to different schedules of judicial status hearings. A lower composite score indicates lesser self-reported drug problems. Statistical analyses were performed on log-transformed scores, which are depicted for ease of interpretation. The non-transformed means and standard deviations are presented in Table 3. Matching-by-risk-by-time interaction effect, co-varying for age: p = 0.07.
3.5. Tertiary analyses
Data on tertiary outcome measures are reported in the lower sections of Tables 2 and 3. Most of the analyses revealed expected main effects for time and risk level. Relevant to the study hypotheses, there was a significant matching-by-time interaction effect on self-reported alcohol intoxication (p < 0.05) (Table 2). Participants who were assigned to the matched condition (regardless of risk level) reported greater reductions in alcohol intoxication from baseline to follow-up than participants assigned to status hearings as usual. There was also a significant matching-by-time interaction effect on the ASI family composite score (p < 0.05) (Table 3). Participants assigned to the matched condition reported greater reductions in family problems from baseline to follow-up than those assigned to status hearings as usual.
4. Discussion
The results of this experimental prospective matching study provide further confirmation of the risk principle in a drug court context. High-risk participants - defined as those with APD or a history of drug abuse treatment - performed significantly better in drug court when they were required to attend frequent, biweekly judicial status hearings in court. Specifically, high-risk participants graduated at a substantially higher rate, provided more drug-negative urine specimens, and reported less illicit drug use and alcohol intoxication when they were matched to bi-weekly hearings. On the other hand, outcomes were generally equivalent for low-risk participants regardless of how often they were required to appear before the judge in court.
These findings underscore the importance of moving beyond simply evaluating baseline predictors of outcomes for drug offenders and identifying variables that differentially predict outcomes in various modalities or intensities of supervision. It has long been known that offenders with APD or prior treatment failures generally have poorer outcomes (e.g., Marlowe et al., 2003a); however, this finding offered little practical instruction for intervening effectively with these difficult-to-treat individuals. Determining how such moderator variables interact with the schedule of court hearings to influence outcomes yields immediate and self-evident guidance for treatment planning.
4.1. Future directions for adaptive programming
This program of research represents only a first step in tailoring adaptive interventions for drug-abusing offenders. More research is needed to improve upon the procedures and to elicit more robust treatment effects. For one thing, our ability to measure baseline risk variables is far from ideal. The accuracy of measurement is influenced by a number of factors, including possible dissimulation on the part of offenders as well as limitations in the reliability and validity of the assessment tools. Most assessment instruments, including the ASI and DSMIV-congruent interviews, contain items that are self-evident in content. Offenders are often capable of figuring out the “correct” answers that will permit them to avoid intensive scrutiny by authorities. It would probably not take them long to realize that endorsing antisocial attitudes and behaviors elicits closer supervision. Over time, the savvier individuals could be expected to manipulate their responses convincingly to avoid such monitoring and coach other participants to do the same.
In addition, no measurement tool is perfectly valid and reliable. There will undoubtedly be an appreciable number of false positives and false negatives in any program. Some offenders with poor prognoses will be mis-assigned to low-intensity conditions and others with good prognoses will be mis-assigned to high-intensity conditions. Some mechanism must be in place to alter the initial placement as a consequence of participants’ ongoing conduct in treatment. For example, if a participant is performing poorly on a reduced schedule of as-needed court hearings, this should trigger a case review by the team to reconsider the initial disposition. Conversely, if a participant who was assigned to bi-weekly hearings demonstrates a sustained interval of sobriety and compliance with treatment, this, too, should prompt a case review and re-consideration of the program requirements. Such an approach requires the specification of standardized performance indicators for determining whether a client is demonstrating progress or lack of progress in the program, plus a set of a priori decision rules for determining how to respond to these clinical presentations. The utility of the decision rules for improving outcomes would then need to be validated in controlled research studies.
It must also be recognized that the effects of baseline matching in this study left considerable room for improvement. High-risk participants did perform significantly better in the matched condition; however, over one-half of them reported engaging in illicit drug use, roughly one-fifth reported engaging in alcohol intoxication, and over 10% reported criminal activity at the 6-month follow-up (see Table 2). For these individuals, the program requires further tailoring to achieve public health and public safety objectives. For example, some of the high-risk participants might have been noncompliant with the program by failing to appear for counseling sessions. For them, it might be necessary to further ratchet up the intensity of judicial supervision or to impose negative sanctions, such as home curfews, anklet monitoring, or residential detention. In contrast, other high-risk participants might have been compliant with program requirements, but still failed to achieve abstinence due to the severity of their drug addiction or a related psychosocial impairment, such as a co-occurring mental health disorder, family dysfunction, unemployment, or homelessness. For these individuals, ratcheting up judicial monitoring or criminal sanctions would not be expected to improve outcomes. Instead, increasing the dosage or scope of treatment services would be indicated. This necessitates the development of standardized performance indicators that differentiate between offenders who are noncompliant as opposed to non-responsive in the program, as well as a priori decision rules for intervening with these different clinical presentations. Again, the utility of the performance indicators and decision rules would need to be validated through controlled clinical trials.
Finally, although the present study revealed improvements for the high-risk participants as a function of matching, no such benefits were elicited for the low-risk participants who comprised roughly two-thirds of the sample. The low-risk clients performed equivalently regardless of the schedule of court hearings. At a minimum, this suggests that reducing the dosage of court hearings for these individuals could permit a program to conserve costly resources without sacrificing client outcomes or public safety. More research is needed, however, to elicit better outcomes for low-risk offenders. Increasing the schedule of court hearings might not yield incremental benefits for these individuals; however, superior outcomes might be achieved by enhancing the quality of counseling services or employing secondary-prevention strategies (e.g., DeMatteo et al., 2006). Hitting a ceiling effect on one intervention should not be interpreted as ruling out potential gains that could be elicited from other interventions that employ different mechanisms of action.
4.2. Limitations
There were several methodological limitations to the current study that must be borne in mind when interpreting the results. The recruitment rate was 39% and study participants had more severe drug problems and less severe criminal histories than individuals who refused to be in the study. There is no way to know whether this selection bias affected the generalizability of the findings. It is possible, for example, that the highest-risk offenders systematically excluded themselves from the research, which would leave open the question of whether bi-weekly hearings can improve outcomes for the most unmotivated or antisocial drug offenders. The only way to get around this issue would be for the drug court to adopt the matching procedures as a routine part of standard practice. This would permit all clients to be exposed to the adaptive intervention. If the adaptive procedures were phased-in with randomly selected clients, outcomes for those individuals could be compared to outcomes for the remainder of the clients. This would allow an effect size for matching to be estimated for the entire target population.
A more serious problem relates to differential attrition from the matched bi-weekly cell. As noted previously, it was not surprising that relatively more participants dropped out of this condition because it placed onerous demands on the most seriously antisocial clients. Regardless, it is possible that these individuals were performing poorly in the program and they may have dropped out of the study to avoid detection by the judge. If so, the results could have systematically over-estimated positive outcomes for the matched bi-weekly participants. Again, there is no way to avoid this potential confound other than to have the drug court adopt the matching procedures in standard practice.
Although it may be concluded that APD and drug treatment history are reliable risk factors in drug courts, this does not necessarily mean that they are the only risk factors or the most robust risk factors. Other variables that were never measured in our studies, such as co-morbid axis I psychiatric diagnoses or cognitive impairments, might have greater utility for predicting success in various types or levels of drug court interventions. Further research is needed to identify other variables that may contribute to better treatment-matching strategies for drug court clients.
Finally, questions remain about how to interpret the influence of prior drug treatment. On one hand, this variable may simply have reflected the severity of participants’ drug problems. That is, participants with more severe or longer-term drug problems may have had more opportunities to be referred or mandated into treatment. Alternatively, it could reflect past negative experiences with drug abuse treatment services. These individuals might have been exposed to prior treatment regimens that lacked credibility in terms of monitoring and responding to their conduct. If so, they might have approached drug court with lowered expectations about being held accountable for their actions. More intensive monitoring by the court might have been necessary to counteract this jaded attitude. Further research is needed to gain a better handle on the nature of this moderator effect.
4.3. Summary
In summary, building on a program of prior experimental research (Festinger et al., 2002; Marlowe et al., 2003c,d,2004,2005,2006), the results of this study provide further evidence for the utility and potential cost-effectiveness of prospectively matching drug offenders to different dosages of judicial supervision based upon an assessment of their risk status or clinical needs. More research is required to determine whether additional benefits can be achieved by continually readjusting the intensity of judicial supervision or treatment services in response to clients’ progress or lack thereof in the program.
Acknowledgements
This research was supported by grant #R01-DA-13096 from the National Institute on Drug Abuse (NIDA). The views expressed are those of the authors and do not reflect the views of NIDA. Portions of these data were presented at the 14th World Congress of Criminology, Philadelphia, PA, and the 67th Annual Scientific Meeting of the College on Problems of Drug Dependence, Orlando, FL.
The authors gratefully acknowledge the continuing collaboration of the New Castle County Court of Common Pleas, Delaware State Attorney General’s Office, Delaware Public Defender’s Office, Delaware Association of Criminal Defense Lawyers, Delaware State Division of Substance Abuse and Mental Health, Treatment Access Center, and Brandywine Counseling, Inc.
References
- Alterman AI, McDermott PA, Cook TG, Metzger D, Rutherford MJ, Cacciola JS, Brown LS. New scales to assess change in the Addiction Severity Index for the opioid, cocaine, and alcohol dependent. Psychol.Addict. Behav. 1998;12:233–246. [Google Scholar]
- American Psychiatric Association . Diagnostic and Statistical Manual of Mental Disorders. 4th ed. American Psychiatric Association; Washington, DC.: 2000. text revision. [Google Scholar]
- Andrews DA, Bonta J. The Psychology of Criminal Conduct. 2nd ed. Anderson; Cincinnati, OH.: 1998. [Google Scholar]
- Belenko S. Research on drug courts: a critical review. Natl. Drug Court Inst. Rev. 1998;1:1–42. [Google Scholar]
- Belenko S. Research on drug courts: a critical review: 1999 update. Natl. Drug Court Inst. Rev. 1999;2:1–58. [Google Scholar]
- Belenko S. Research on Drug Courts: A Critical Review: 2001 Update. National Center on Addiction and Substance Abuse at Columbia Univ.; New York: 2001. [Google Scholar]
- Cacciola JS, Koppenhaver JM, McKay JR, Alterman AI. Test-retest reliability of the lifetime items on the addiction severity index. Psychol.Assess. 1999;11:86–93. [Google Scholar]
- Collins LM, Murphy SA, Bierman KA. A conseptual framework for adaptive preventive interventions. Prevention Science. 2004;5:185–196. doi: 10.1023/b:prev.0000037641.26017.00. [DOI] [PMC free article] [PubMed] [Google Scholar]
- DeMatteo DS, Marlowe DB, Festinger DS. Secondary prevention services for clients who are low risk in drug court: a conceptual model. Crime Delinquency. 2006;52:114–134. doi: 10.1177/0011128705281746. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Diggle PJ, Liang KY, Zeger SL. Analysis of Longitudinal Data. Oxford University Press; New York: 1994. [Google Scholar]
- Festinger DS, DeMatteo DS, Marlowe DB, Lee PA. Expungement of arrest records in drug court: Do clients know what they’re missing. Drug Court Rev. 2005;5:1–21. [Google Scholar]
- Festinger DS, Marlowe DB, Lee PA, Kirby KC, Bovasso G, McLellan AT. Status hearings in drug court: when more is less and less is more. Drug Alcohol Depend. 2002;68:151–157. doi: 10.1016/s0376-8716(02)00187-4. [DOI] [PubMed] [Google Scholar]
- Finigan MW. Assessing cost off-sets in a drug court setting. Natl. Drug Court Inst. Rev. 1999;2:59–91. [Google Scholar]
- First MB, Gibbon M, Spitzer RL, Williams JBW. Structured Clinical Interview for DSM-IV Axis II Personality Disorders. American Psychiatric Press; Arlington, VA.: 1997. [Google Scholar]
- Gendreau P, Little T, Goggin C. A meta-analysis of the predictors of adult offender recidivism: What works. Criminology. 1996;34:575–596. [Google Scholar]
- Goldkamp J. Do drug courts work? Getting inside the drug court blackbox. J. Drug Issues. 2001;31:27–72. [Google Scholar]
- Littell RC, Milliken GA, Stroup WW, Wolfinger RD. SAS System for Mixed Models. SAS Institute; Cary, NC.: 1996. [Google Scholar]
- Marlowe DB, DeMatteo DS, Festinger DS. A sober assessment of drug courts. Fed. Sent. Rep. 2003b;16:153–157. [Google Scholar]
- Marlowe DB, Festinger DS, Dugosh KL, Lee PA. Are judicial status hearings a “key component” of drug court? Six and twelve months outcomes. Drug Alcohol Depend. 2005;79:145–155. doi: 10.1016/j.drugalcdep.2005.01.019. [DOI] [PubMed] [Google Scholar]
- Marlowe DB, Festinger DS, Lee PA. The role of judicial status hearings in drug court. Offender Subst. Abuse Rep. 2003d;3:33–46. [Google Scholar]
- Marlowe DB, Festinger DS, Lee PA. The judge is a key component of drug court. Drug Court Rev. 2004;4:1–34. [Google Scholar]
- Marlowe DB, Festinger DS, Lee PA, Dugosh KL, Benasutti KM. Matching judicial supervision to clients’ risk status in drug court. Crime Delinquency. 2006;52:52–76. doi: 10.1177/0011128705281746. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Marlowe DB, Festinger DS, Lee PA, Schepise MM, Hazzard JER, Merrill JC, Mulvaney FD, McLellan AT. Are judicial status hearings a key component of drug court? During-treatment data from a randomized trial. Crim. Justice Behav. 2003c;30:141–162. [Google Scholar]
- Marlowe DB, Kirby KC. Effective use of sanctions in drug courts: Lessons from behavioral research. Natl. Drug Court Inst. Rev. 1999;2:1–31. [Google Scholar]
- Marlowe DB, Patapis NS, DeMatteo DS. Amenability to treatment of drug offenders. Fed. Probation. 2003a;67:40–46. [Google Scholar]
- McDermott PA, Alterman AI, Brown L, Zaballero A, Snider EC, McKay JR. Construct refinement and confirmation for the addiction severity index. Psychol. Assess. 1996;8:182–189. [Google Scholar]
- McLellan AT, Cacciola J, Kushner H, Peters R, Smith I, Pettinati H. The fifth edition of the addiction severity index: cautions, additions and normative data. J. Subst. Abuse Treat. 1992;9:461–480. doi: 10.1016/0740-5472(92)90062-s. [DOI] [PubMed] [Google Scholar]
- McLellan AT, Luborsky L, Cacciola JC, Griffith J, Evans F, Barr HL, O’Brien CP. New data from the addiction severity index: reliability and validity in three centers. J. Nerv. Ment. Dis. 1985;173:412–423. doi: 10.1097/00005053-198507000-00005. [DOI] [PubMed] [Google Scholar]
- McLellan AT, Luborsky L, O’Brien CP, Woody GE. An improved diagnostic instrument for substance abuse clients: the addiction severity index. J. Nerv. Ment. Dis. 1980;168:26–33. doi: 10.1097/00005053-198001000-00006. [DOI] [PubMed] [Google Scholar]
- Murphy SA. An experimental design for the development of adaptive treatment strategies. Stat. Med. 2005;24:1455–1481. doi: 10.1002/sim.2022. [DOI] [PubMed] [Google Scholar]
- National Association of Drug Court Professionals . Defining Drug Courts: The Key Components. Office of Justice Programs, US Dept. of Justice; Washington, DC.: 1997. [Google Scholar]
- Peters RH, Haas AL, Murrin MR. Predictors of retention and arrest in drug court. Natl. Drug Court Inst. Rev. 1999;2:33–60. [Google Scholar]
- SAS Institute . SAS/STAT Software: Changes and Enhancements Through Release 8.02. SAS Institute, Inc.; Cary, NC.: 2001. [Google Scholar]
- Satel SL. Drug Treatment: The Case for Coercion. American Enterprise Institute; Washington, DC.: 1999. [Google Scholar]
- Schottenfeld RS. Involuntary treatment of substance abuse disorders—impediments to success. Psychiatry. 1989;52:164–176. doi: 10.1080/00332747.1989.11024441. [DOI] [PubMed] [Google Scholar]
- Taxman FS, Marlowe DB, editors. Risk, needs, responsivity: in action or inaction? [Introduction to special issue] Crime Delinquency. 2006;52:3–6. [Google Scholar]
- US Government Accountability Office . Adult Drug Courts: Evidence Indicates Recidivism Reductions and Mixed Results for Other Outcomes. US Government Accountability Office; Washington, DC.: 2005. [No. GAO-05-219] [Google Scholar]