

Abstract
The authors investigated the efficacy of an interactive Web site, MyStudentBody.com: Alcohol (MSB:Alcohol) that offers a brief, tailored intervention to help heavy drinking college students reduce their alcohol use. They conducted a randomized, controlled clinical trial to compare the intervention with an alcohol education Web site at baseline, postintervention, and 3-month follow-up. Students were assessed on various drinking measures and their readiness to change their drinking habits. The intervention was especially effective for women and persistent binge drinkers. Compared with women who used the control Web site, women who used the intervention significantly reduced their peak and total consumption during special occasions and also reported significantly fewer negative consequences related to drinking. In addition, persistent heavy binge drinkers in the experimental group experienced a more rapid decrease in average consumption and peak consumption compared with those in the control group. The authors judged MSB:Alcohol a useful intervention for reaching important subgroups of college binge drinkers.
Keywords: alcohol, binge drinking, brief intervention, college, Web site
Despite the proliferation of prevention and intervention programs devoted to college binge drinking, student consumption patterns have remained relatively impervious to change. Eighty percent of college students drink alcohol.1 The term binge drinking, defined as consumption of 5 or more drinks for men or 4 or more drinks for women per drinking occasion at least once in the past 2 weeks, has been applied to this population.2 Using this definition, large-scale college surveys indicate that about 40% of college students report binge drinking.1 In the past year, about 30% of college students met criteria for alcohol abuse, and 6% for alcohol dependence.3 Drinking-related consequences among college students include alcohol-related health problems, sexual and physical assault, vandalism, unintentional injuries, and academic problems.1,4 Recent studies have demonstrated that female college students may experience particularly negative effects of alcohol use by themselves and by others,5 but research evaluating the effects of interventions with this population is rare.
Aside from publicity and extensive surveys about drinking on college campuses, we found surprisingly few well-researched interventions. Recent reviews indicate that educational and values clarification approaches appear to have minimal impact, whereas interventions aimed at altering attitudes or improving personal skills have had greater effect.6,7 One of the most surprising findings is that the duration of the intervention is not related to outcome and that some of the briefest programs achieve positive results.7
A growing literature describes the effectiveness of brief intervention programs that provide students with individualized normative feedback regarding their alcohol consumption patterns and perceptions of drinking, as well as drinking moderation strategies. Baer and associates8 found that a single session of feedback for college freshmen produced significant reductions in negative consequences of drinking over a 4-year follow-up. Several studies have found that mailing feedback about their drinking to students leads to reduced alcohol consumption.9–11
Dimeff and associates,12 who formulated the Brief Alcohol Screening and Intervention for College Students (BASICS) program, developed the best known use of feedback as a brief intervention. BASICS consists of 2 50-minute sessions in which the student is asked to complete questionnaires tapping his or her drinking patterns, high-risk situations, and beliefs about drinking. The student is then provided with personalized, motivational feedback related to alcohol use consequences and risk factors. This feedback juxtaposes the student’s drinking habits and expectancies against college student population norms. At follow-up assessments over a 2-year period, students who received the intervention showed significant reductions in both drinking rates and harmful consequences.
The BASICS program has been delivered in various ways, including individual12–14 and group sessions,15 individual peer-delivered feedback,16 and computer-based interventions.17,18 These studies generally show modest effects in lighter drinkers, but BASICS appears to be more effective in reducing alcohol consumption in heavier college drinkers (at least 20 drinks per week).13 As a result, the Task Force on College Drinking19 strongly supports the use of interventions that comprise individualized normative and motivational feedback.
Unfortunately, brief interventions suffer from the same limitations as other college alcohol interventions, including low response rates to recruitment, low completion rates, and modest effects on drinking and related risk behaviors.6 Students with the greatest need (ie, heavier drinkers) are generally not interested in any type of program.20 Surveys show that most college students want unassisted, self-directed, or minimal-contact methods to address alcohol misuse; group and individual counseling programs are the least preferred programs.20 Motivational interventions designed to be delivered to identified individuals in person or by mail may limit student participation because of confidentiality concerns. The scope of brief interventions is also limited by staffing shortages and the sheer number of students, thus preventing campus-wide delivery. An anonymous, population-based approach to brief intervention is therefore suggested.
Because of the increased availability of computers on campus, college health professionals have begun using computer programs to educate students about alcohol and its effects. The confidential and nonjudgmental quality of computers may increase the potential for students to divulge personally relevant information, which may facilitate knowledge, attitudes, or behavior change. Compared with paper-and-pencil questionnaires, computerized programs for young people increase self-disclosure in sensitive areas, such as risky sexual behavior, excessive alcohol use, marijuana use, and family problems.21,22
These advantages multiply when applied through the Internet, which is ubiquitous on college campuses. College students are probably the most “wired” of all demographic groups. Indeed, the Internet is increasingly important to students’ education about health. In a recent survey of 15- to 24-year-olds, two thirds of respondents reported that they had received health information online and one quarter sought information about drug or alcohol problems.23 Rather than target individuals or small groups of college students, the Internet potentially allows transmission to thousands of students. In addition, the database capacities of Internet programs allow for more personal tailoring and feedback.
Our purpose in conducting this study was to evaluate the efficacy of an Internet-based brief intervention program called MyStudentBody.com: Alcohol (MSB:Alcohol), which we developed to provide students with tailored motivational feedback about high-risk drinking. Because of growing concerns about the drinking among college women, we also evaluated the effect of the intervention according to gender. Compared with a control group that received standard online text-based information about high-risk drinking, we hypothesized that the experimental MSB:Alcohol group participants would show (1) significantly less alcohol use, (2) a decrease in problematic alcohol behaviors, and (3) significantly greater readiness to change.
METHOD
Design
We designed a single-blind randomized, controlled clinical trial to assess the effect of MSB:Alcohol on the alcohol use, alcohol-related problems, and readiness to change of students who binge drink, compared with a text-based education-only Web site. Although we designed the intervention for use by the general college student population, we chose to focus evaluations on binge drinkers because they are clearly a priority population in college alcohol programming.1,4 We chose a Web site as a control to avoid the potential confounding effects of the method of delivery of the intervention that also provides a more rigorous control comparison than that of an assessment-only group.
To access an adequate sample size that represents the target population, we undertook a screening for college binge drinkers. Five public and private, 2-year and 4-year colleges and universities in Massachusetts (University of Massachusetts–Dartmouth; Boston University; Middlesex Community College–Bedford and Lowell; Tufts University, Med-ford; and Northeastern University–Boston), took part in the screening. Potential participants were enrolled in the study through college newspaper ads, flyers, recruitment tables placed in high traffic areas on campus, and during key events such as Alcohol Awareness Week. Inflexxion’s Institutional Review Board (IRB) and IRBs at each of the participating sites approved the study.
Screening
Students self-administered the Daily Drinking Questionnaire12 and completed a brief demographic survey to screen for binge drinkers. Although criteria that best express college students’ risky drinking24 have been widely debated, we adapted the Wechsler definition of binge drinker because of its broad use in major alcohol use surveys.25,26 On the basis of previous positive results of brief intervention approaches with heavy drinkers, we adopted a more stringent definition of binge drinking than that used by Wechsler: 5 or more drinks for men or 4 or more drinks for women, per drinking occasion, at least once in the past week. Of the 538 potential volunteers screened, 317 (59%) of responding students met the study’s binge drinking criteria; of these, 265 (84%) gave written informed consent to participate in the study. Students received $5 for the screening.
Efficacy Trial
Study Sample
We randomized the 265 participants to either MSB:Alcohol or a control condition. To ensure sufficient power to explore the effects of these interventions on gender, we preselected 50% representation of women in both groups. We used the urn system of random assignment to condition27 and to ensure equivalence of the groups on age and race.
Interventions
MSB:Alcohol is an interactive Web site that offers college students motivational feedback as a means of helping them identify potential problems and encourages risk-reduction behaviors. As a program for the general student population, it includes both primary (eg, general information, drinking-related risks, helping fellow students who drink too much) and secondary (eg, Rate Myself) prevention elements. Rate Myself, a brief intervention based on the BASICS model, is the centerpiece of the site. Students complete 4 sets of questions: (1) beliefs regarding alcohol; (2) lifestyle issues (Greek and athletic involvement, residence type); (3) the risks they take when they drink (driving, other substance use, vandalism, violence, and sexual risk-taking); and (4) the consequences they suffer as a result of drinking (dependence on alcohol, interpersonal problems, poor grades). These questions are based on the items most predictive of excessive drinking that we gleaned from standardized instruments and factor analyses.28–30 The student receives immediate tailored feedback and has the option of printing out a personal report. His or her responses to Rate Myself highlight Web-site content that represents personal risk factors, thus allowing students to receive a tailored site experience. Students can update this information as frequently as they wish.
MSB:Alcohol offers a variety of college-specific articles, strategies, and interactive tools related to alcohol and drinking on campus. The site includes weekly updates of peer stories (Student Voices), Ask the Expert (answers from a college alcohol expert to frequently asked alcohol questions), and college health news. Students can use a state law calculator, a social norm calculator (comparing drinking pattern to peers on the basis of gender, race or ethnic group, Greek membership, and athletic participation), and tools with information about street-drug effects and alcohol-medication interactions. Strategies include moderation tips, how to stay safe during spring beak, how to communicate with roommates about drinking problems, and ways to cope with Greek life. A prominently featured emergency area helps students recognize effective ways to deal with alcohol poisoning and find local resources in the event of urgent medical problems.
The control group (Alcohol and You) was intended to provide a comparison with the educational content found at many Web sites. Students visited and read research-based articles about the effects of excessive drinking once a week on 4 consecutive weeks.31–34 Unlike MSB:Alcohol, the articles had no tailored, interactive, motivational, or skill-building elements.
Measures
We used 2 different measures to assess patterns of drinking. The Daily Drinking Questionnaire (DDQ)12 provided measures of peak consumption, quantity, and frequency over a typical drinking week. From the DDQ data, we compiled a composite score that consisted of past-week average consumption, binge episodes, and maximum drinks consumed on a drinking day. The second measure was an enhancement of the DDQ that included the use of calendars, modeled on the Alcohol Timeline Followback method,35 to assess students’ drinking over time on special occasions (eg, homecoming, holidays, pub nights). At each assessment point, a trained clinical evaluator administered the enhanced DDQ to the student. We measured alcohol-related problems with the Rutgers Alcohol Problem Index (RAPI).36 In addition, we gathered information about students’ readiness to change their drinking habits through the Readiness to Change Questionnaire.37
Procedure
Students in the MSB:Alcohol and control groups used personal computers at home or at school to access the appropriate Web site, using personal log-in codes assigned to them. On the basis of these codes, we were able to identify who logged on, the date or dates and duration of their Internet activity, as well as areas of the Web site that were visited during each visit.
Research assistants met with students in an orientation session to explain access to their assigned conditions and provide each student with a personal log-in code. They told students how to access the appropriate Web site for 4 weekly 20-minute sessions. Both sites were available for 24 hours a day, 7 days a week, so students had flexible access, but they could not advance to the next session until they completed the current session. If students were unable to complete a session on a particular day or their session was interrupted for some reason, they simply logged on at another time. After they completed each week’s protocol, we sent them reminder e-mails to return for the next week’s session.
To maintain consistency in the Web-site experience, each MSB:Alcohol student received a session-by-session protocol for navigating the site. The protocol consisted of completing all Rate Myself questions, reading through all 3 updated areas, reviewing highlighted risk areas, and visiting any other areas of interest. We asked control students to visit the control Web site and read the assigned online article each week. Research assistants were available by telephone or e-mail and provided assistance only with Web-site navigational or access issues.
All participants received the assessment battery at baseline, postintervention (approximately 1 month after baseline), and 3-months postintervention. Except for the interviewer-administered enhanced DDQ, all assessments were self-administered. Students were paid a total of $135 for attending the orientation session and completing the 3 assessment batteries.
Student Evaluation of Intervention
After completing the trial, participants were asked to complete a 9-item survey tapping their perceptions of key elements of the interventions. We rated items on a 7-point Likert-type scale (1 = very poor, 7 = excellent) and included the quality of information, enhancement of alcohol-related knowledge, potential influence on drinking, likelihood of recommending it to a friend, and overall satisfaction.
Statistical Analysis
The primary analyses were repeated measures analyses of variance (ANOVAs) with 2 factors— intervention and gender. The primary dependent variables were readiness to change, RAPI score, and drinking behaviors generated from the DDQ and its enhancement. The typical past-week drinking behaviors that we analyzed were total quantity, frequency of consumption, average drinks per drinking day, peak consumption (binges and maximum number of drinks consumed on a drinking day), and a composite score comprising average consumption, frequency of binge episodes, and maximum drinks consumed on a drinking day. When appropriate, we log-transformed skewed data so that we could undertake inferential statistics. We z-transformed composite score components before summing them. We conducted analyses of covariance (ANCOVAs) for the drinking behavior outcomes when only 2 data points were analyzed (ie, special occasion drinking and RAPI scores at follow-up), controlling for baseline values.
Scoring for the readiness to change measure created 3 ordered categories: Precontemplation, Contemplation, and Action. We used both a continuous and nonparametric analysis of stage progression to assess differences between the 2 groups.38 In the first approach, we considered the number of stages progressed through and the outcome, ranging from −2 (loss of 2 stages) to 2 (gain of 2 stages). We then performed an ANOVA. In the second approach, we assessed a dichotomized outcome: progress or no progress. We considered forward stage movements “progress,” whereas no movement or regression counted as “no progress.” However, if participants started in the Action category and maintained or returned to the Action category by the end of the study, they were grouped with those who had progressed. We then conducted a logistic regression analysis to assess whether the intervention was a predictor of stage progress.
We used an intent-to-treat design so that, once randomized, all subjects were followed and evaluated, regardless of whether they adhered to the study protocol. At baseline, 21 students (7.9%) reported they had no binge drinking episodes in the past week, thus technically making them ineligible for study participation. Because these 21 students had already been randomized into the study and reported alcohol consumption but no binge episodes, they completed the study and we included their data in the following analyses.
We tested for possible moderator variables, including race, site of recruitment, baseline readiness to change, and age, using a Type I error of .10. If moderator variables were identified, we entered them into the repeated measures analyses, as appropriate. For the intervention evaluation, we carried out z tests of proportions to determine statistically significant differences between students’ satisfaction with the sites. We conducted all significance tests at the p < .05 level and reported them alongside their 95% confidence intervals. We also reported eta squares (η2) as estimates of effect size. We performed analyses with the SPSS software package, Version 11.0.39
RESULTS
Study Sample
The data in Table 1 describe the study population, illustrating that randomization succeeded in balancing intervention assignments and ensuring equal representation of important characteristics in the study population. Over the course of the trial, 53 students were either lost to follow-up (n = 23) or dropped out (n = 30) of the study, for an overall response rate of 80%. Eighty-six percent of the MSB:Alcohol students and 89% of control group students completed all 4 sessions, a difference that did not achieve statistical significance.
TABLE 1.
Characteristics of Study Participants, by Randomly Assigned Condition
| MSB:Alcohol (n = 131)
|
Control (n = 134)
|
All (N = 265)
|
||||
|---|---|---|---|---|---|---|
| Characteristic | n | % | n | % | n | % |
| Race | ||||||
| White | 92 | 70.2 | 102 | 76.1 | 194 | 73.2 |
| Asian | 17 | 13.0 | 13 | 9.7 | 30 | 11.3 |
| Black | 5 | 3.8 | 4 | 3.0 | 9 | 3.4 |
| Latino/Hispanic | 11 | 8.4 | 9 | 6.7 | 20 | 7.5 |
| Other | 6 | 4.6 | 6 | 4.5 | 12 | 4.5 |
| Age M/SD | 20.0/1.7 | 19.8/1.4 | 19.9/1.6 | |||
| Gender | ||||||
| Female | 71 | 54.2 | 72 | 53.7 | 143 | 54.0 |
| Male | 60 | 44.8 | 62 | 46.3 | 122 | 46.0 |
| Year in school | ||||||
| 1st | 46 | 35.1 | 44 | 33.1 | 90 | 34.1 |
| 2nd | 42 | 32.1 | 44 | 33.1 | 86 | 32.6 |
| 3rd | 21 | 16.0 | 29 | 21.8 | 50 | 18.9 |
| 4th /5th | 22 | 16.8 | 16 | 12.0 | 38 | 14.4 |
| Institution type | ||||||
| 2-year | 39 | 29.8 | 43 | 32.1 | 82 | 30.9 |
| 4-year | 92 | 70.2 | 91 | 67.9 | 183 | 69.1 |
| Residence type | ||||||
| Dorm/on-campus | 68 | 51.5 | 64 | 48.1 | 132 | 50.0 |
| Off-campus housing | 26 | 19.8 | 25 | 18.8 | 51 | 19.3 |
| At home | 28 | 21.4 | 40 | 30.0 | 68 | 25.8 |
| Fraternity or other | 9 | 6.9 | 4 | 3.0 | 13 | 4.9 |
| Greek involvement | ||||||
| Involved | 9 | 6.9 | 10 | 7.6 | 19 | 7.3 |
| Not involved | 121 | 93.1 | 121 | 92.4 | 242 | 92.7 |
| Athletic involvement | ||||||
| Involved | 30 | 22.9 | 24 | 18.2 | 54 | 20.5 |
| Not involved | 101 | 77.1 | 108 | 81.8 | 209 | 79.5 |
We conducted a logistic regression analysis to assess the independent effects of variables we found in bivariate analyses to be significantly related to study incompletion, as well as of other substantive variables that could be related to not completing the study. Study site (one 2-year and one 4-year institution) and baseline stage of readiness for change designation (contemplation) were the only independent predictors of not completing the study.
Alcohol Use Behaviors
Results from all outcome data collected at each time point are reported in Table 2. Overall, the number of binge drinking episodes, the amount of alcohol students drank, how frequently they drank, and the quantity of alcohol they drank on special occasions decreased over time in both groups. Effects of the MSB:Alcohol were evident in several alcohol-use behavior outcomes.
TABLE 2.
Means and 95% Confidence Intervals (95% CIs) for All Primary Study Outcomes at Each Time Point, by Condition and Gender, in MSB:Alcohol, a High-Risk Drinking-Prevention Web Site
| MSB:Alcohol Mean (n = 105)
|
MSB:Alcohol Women (n = 63)
|
MSB:Alcohol Men (n = 42)
|
Control Mean (n = 110)
|
Control Women (n = 60)
|
Control Men (n = 50)
|
|||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| M | 95% CI | M | 95% CI | M | 95% CI | M | 95% CI | M | 95% CI | M | 95% CI | |
| Peak consumption (binge drinking days/wk) | ||||||||||||
| Baseline | 2.3 | 2.0, 2.5 | 1.9 | 1.6, 2.2 | 2.7 | 2.3, 3.1 | 2.4 | 2.2, 2.7 | 2.4 | 2.0, 2.7 | 002.5 | 002.1, 002.9 |
| Post | 1.6 | 1.3, 1.9 | 1.3 | 1.0, 1.7 | 1.9 | 1.5, 2.3 | 1.9 | 1.6, 2.1 | 1.8 | 1.5, 2.2 | 1.9 | 1.5, 2.3 |
| 3 months | 1.2 | 0.92, 1.5 | 0.9 | 0.5, 1.2 | 1.5 | 1.1, 1.9 | 1.5 | 1.2, 1.7 | 1.5 | 1.1, 1.8 | 1.4 | 1.0, 1.8 |
|
| ||||||||||||
| Peak consumption (Maximum number of drinks consumed/drinking day)* | ||||||||||||
| Baseline | 2.0 | 1.9, 2.0 | 1.8 | 1.6, 1.9 | 2.2 | 2.0, 2.3 | 2.0 | 1.9, 2.1 | 1.8 | 1.7, 2.0 | 2.2 | 2.0, 2.3 |
| Post | 1.56 | 1.4, 1.7 | 1.3 | 1.1, 1.5 | 1.8 | 1.6, 2.0 | 1.74 | 1.6, 1.9 | 1.6 | 1.4, 1.8 | 1.9 | 1.7, 2.1 |
| 3 months | 1.4 | 1.2, 1.6 | 1.1 | .85, 1.3 | 1.7 | 1.5, 2.0 | 1.3 | 1.1, 1.5 | 1.2 | 1.0, 1.4 | 1.4 | 1.2, 1.6 |
|
| ||||||||||||
| Quantity of consumption (drinks/wk) | ||||||||||||
| Baseline | 19.6 | 16.6, 22.7 | 13.9 | 10.0, 17.7 | 25.4 | 20.7, 30.1 | 23.3 | 20.4, 26.2 | 17.9 | 14.0, 21.9 | 28.7 | 24.4, 33.1 |
| Post | 14.6 | 12.0, 17.2 | 9.9 | 6.7, 13.2 | 19.2 | 15.3, 23.2 | 17.5 | 15.0, 19.9 | 14.8 | 11.5, 18.1 | 20.2 | 16.5, 23.8 |
| 3 months | 12.4 | 9.8, 15.1 | 8.2 | 4.8, 1.5 | 16.7 | 12.6, 20.8 | 13.7 | 11.1, 16.2 | 11.5 | 8.1, 15.0 | 15.8 | 12.0, 19.6 |
|
| ||||||||||||
| Frequency of consumption (drinking days/wk) | ||||||||||||
| Baseline | 3.0 | 2.8, 3.3 | 2.6 | 2.3, 3.0 | 3.4 | 3.0, 3.8 | 3.4 | 3.2, 3.7 | 3.1 | 2.7, 3.4 | 3.8 | 3.4, 4.2 |
| Post | 2.6 | 2.3, 2.9 | 2.3 | 2.0, 2.7 | 2.9 | 2.5, 3.4 | 2.9 | 2.7, 3.2 | 2.7 | 2.3, 3.0 | 3.2 | 2.8, 3.7 |
| 3 months | 2.4 | 2.0, 2.7 | 2.2 | 1.8, 2.7 | 2.5 | 2.0, 3.1 | 2.6 | 2.3, 3.0 | 2.4 | 2.0, 2.8 | 2.8 | 2.3, 3.3 |
|
| ||||||||||||
| Average consumption/drinking day* | ||||||||||||
| Baseline | 1.8 | 1.7, 1.8 | 1.5 | 1.4, 1.7 | 1.9 | 1.8, 2.1 | 1.8 | 1.7, 1.9 | 1.7 | 1.6, 1.8 | 1.9 | 1.7, 2.0 |
| Post | 1.4 | 1.3, 1.5 | 1.1 | 1.0, 1.3 | 1.6 | 1.4, 1.8 | 1.5 | 1.4, 1.7 | 1.5 | 1.3, 1.6 | 1.6 | 1.5, 1.8 |
| 3 months | 1.2 | 1.1, 1.4 | .91 | .71, 1.1 | 1.5 | 1.3, 1.7 | 1.1 | 1.0, 1.3 | 1.1 | .88, 1.3 | 1.2 | 1.0, 1.4 |
|
| ||||||||||||
| Alcohol composite score (sum of z scores) | ||||||||||||
| Baseline | −.09 | −.55, .37 | −1.2 | −1.7, −.57 | .98 | .26, 1.7 | .23 | −.23, .69 | −.25 | −.87, .36 | .72 | .04, 1.4 |
| Post | −.32 | −.85, .22 | −1.2 | −1.9, −.50 | .55 | −.28, 1.4 | .39 | −.13, .91 | −.03 | −.73, .67 | .81 | .03, 1.6 |
| 3 months | .15 | −.39, .69 | −.85 | −1.5, −.16 | 1.2 | .31, 2.0 | .22 | −.32, .75 | .01 | −.71, .72 | .43 | −.36, 1.2 |
|
| ||||||||||||
| Total consumption during special occasion drinking past 3 months | ||||||||||||
| Baseline | 80.2 | 64.1, 96.3 | 61.0 | 39.2, 82.9 | 99.4 | 75.7, 123 | 109.0 | 93.3, 124.8 | 91.4 | 69.6, 113.3 | 126.6 | 103.9, 149.3 |
| 3 months | 53.5 | 43.0, 64.0 | 54.2 | 41.7, 66.7 | 69.9 | 54.7, 85.1 | 67.1 | 55.9, 78.3 | 67.7 | 55.1, 80.31 | 55.1 | 41.0, 69.3 |
|
| ||||||||||||
| Peak consumption during special occasion drinking over past 3 mo† | ||||||||||||
| Baseline | 8.1 | 6.9, 9.4 | 7.6 | 5.9, 9.3 | 8.8 | 7.0, 10.6 | 10.7 | 9.2, 12.2 | 11.3 | 9.1, 13.6 | 10.0 | 8.2, 11.9 |
| 3 months | 5.8 | 4.8, 6.9 | 6.4 | 5.1, 7.7 | 6.8 | 5.2, 8.4 | 7.2 | 6.0, 8.4 | 7.7 | 6.3, 9.0 | 5.5 | 14.1, 7.0 |
|
| ||||||||||||
| Percentage in action stage | ||||||||||||
| Baseline | 35.9 | 33.8 | 38.3 | 28.4 | 26.4 | 30.6 | ||||||
| Post | 39.3 | 34.8 | 45.1 | 34.8 | 29.7 | 41.2 | ||||||
| 3 months | 42.3 | 38.7 | 47.6 | 42.7 | 40.0 | 46.0 | ||||||
Log transformed.
n = 173. One site not included because of unexplained high variability.
Peak Consumption: Binge Drinking Days and Maximum Number of Drinks/Drinking Day, Past Week
The average number of binge episodes in a typical drinking week significantly decreased during the study for all participants (within-groups change, F[1, 213] = 124.03, p < .001). We found no significant interactions for binge episodes. For maximum drinks per drinking day, MSB:Alcohol students reported a significantly higher rate of reduction in the maximum number of drinks consumed on a drinking day, F(1, 208) = 6.28, quadratic effect, p = .013, partial η2 = .029, although students in both groups significantly reduced this type of peak consumption over the course of the study, Thus, the experimental group decreased their maximum number of drinks consumed on a drinking day sooner (ie, from baseline to postassessment) and more profoundly than controls. By follow-up, however, both groups reported similar values of maximum drinks per drinking day. Neither the linear nor quadratic interactions of time-by-condition-by gender for maximum drinks per drinking day were significant.
Typical Alcohol Consumption
We found significant decreases in the 3 indicators of typical alcohol consumption over the study period (within-group changes, p < .001), signifying that consumption generally decreased for all students in the study, but found no significant interactions for any of the indicators.
Upon closer inspection of the typical drinking data, the baseline observations of the quantity and frequency indicators for the 215 participants who completed the assessments were significantly different from those of the 50 participants who did not complete all assessments (ie, dropped out or were lost to follow-up). We decided to explore the potential impact of this discrepancy on the quantity and frequency indicators. To adjust for this observed difference and preserve statistical power, we conducted several missing value analyses, applying the most statistically economical and conservative approach and using an individual’s available observations to predict and replace the missing values.40 In using this approach, we found no significant differences between experimental groups in baseline frequency and quantity of typical drinking values. However, the repeated measures analyses of quantity and frequency outcomes were unchanged from those presented earlier.
Alcohol Use Composite Score
The alcohol use composite outcome revealed a significant overall increase (ie, worsening) in drinking indicators over time, but also suggested a quadratic trend favoring MSB:Alcohol, F(1, 206) = 3.23, quadratic effect, p = .074, partial η2 = .015. Initially, the experimental group decreased (ie, improved) their composite drinking behavior from base-line to postassessment, whereas the control group continued to worsen. By follow-up, however, the experimental group’s composite score resembled that of the control groups’ elevated follow-up alcohol composite score. These data suggest that, compared with controls, MSB:Alcohol may produce a protective effect, delaying the increase in composite score drinking experienced by this high-risk population.
Alcohol Use Among Persistent Heavy Binge Drinkers
Sixty-seven percent (n = 178) of the students continued to report consuming alcohol at follow-up. Students who continued to drink were significantly (all p < .05) older (mean age 20 [1.6 SD] vs 19.3 [1.4 SD]), more frequent binge drinkers (2.4 [1.3 SD] vs 1.7 [1.2 SD] binges per week at baseline), and heavier consumers of alcohol (2.0 [.48 SD] vs 1.8 [.55 SD] log of baseline maximum drinks consumed per week) than were those who did not continue to report drinking at follow-up. Nevertheless, both groups consumed comparable quantities of alcohol per average drinking day and were otherwise similar on sociodemographic characteristics.
When we focused on the group of persistent heavy drinkers, we found notable differences in drinking behaviors for MSB:Alcohol participants. Persistent heavy drinkers in the experimental group experienced a more rapid decrease in average consumption (average drinks per drinking day, F[1, 171[ = 8.18, quadratic effect, p = .005, partial η2 = .046; Figure 1) and peak consumption (maximum number of drinks/drinking day, F[1, 171] = 8.2, quadratic effect, p = .005, partial η2 = .046, Figure 2) than their control group counterparts. Both outcome decreases were maintained through follow-up, and both analyses produced no significant 3-way interactions with gender, time, and condition, suggesting that this effect of the intervention program was the same for men and women. For the alcohol composite score, persistent heavy drinkers in the MSB:Alcohol group exhibited the same delayed increase described above, which achieved statistical significance in this subgroup, F(1, 170) = 4.77, quadratic effect, p = .03, partial η2 = .027 (Figure 3). Of borderline statistical significance was the precipitous drop from baseline to post assessment, compared with controls, in the quantity of alcohol consumed among persistent heavy binge drinking women in the MSB:Alcohol group, F(1, 171) = 3.62, p = .059, partial η2 = .021.
FIGURE 1.
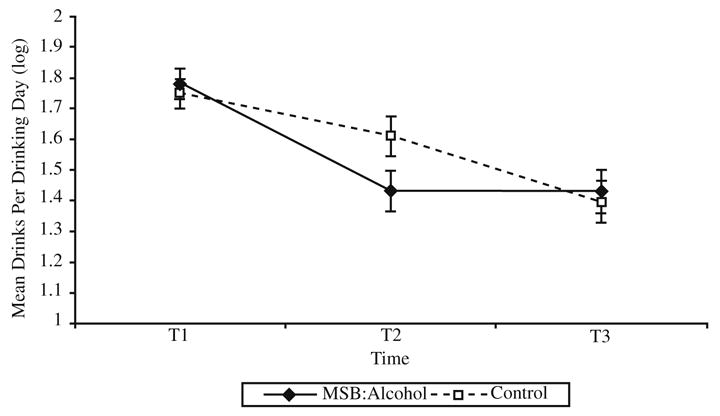
Average alcohol consumption among persistent heavy drinkers, by condition.
FIGURE 2.
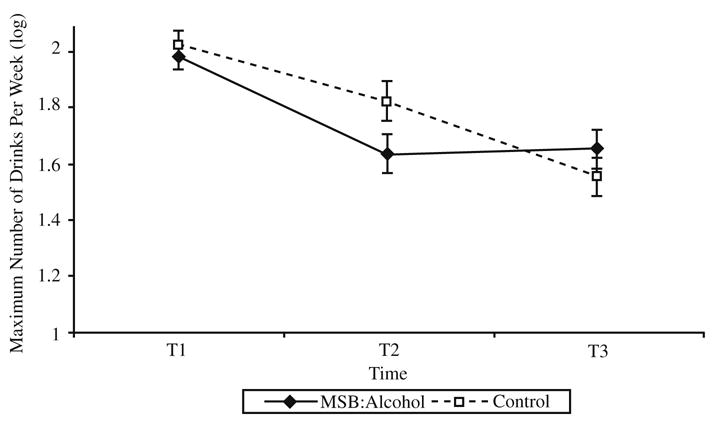
Peak alcohol consumption among persistent heavy drinkers, by condition.
FIGURE 3.
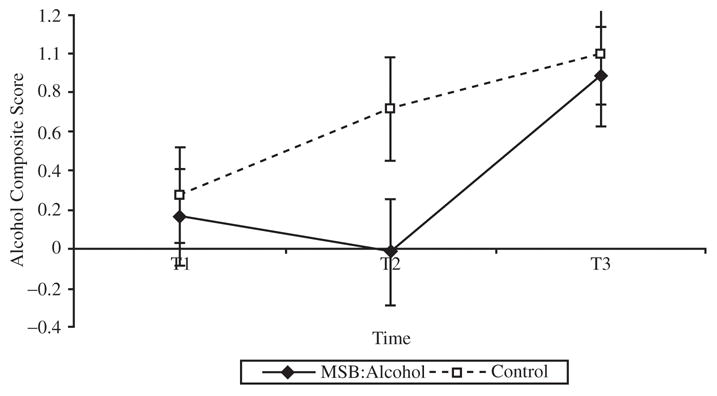
Alcohol composite scores among persistent heavy drinkers, by condition.
Total Consumption During Special Occasion Drinking
Both male and female participants reduced their total alcohol consumption on special occasions, and MSB:Alcohol female participants showed more significant reductions than did those in the control group, F(1, 171) = 4.28, p = .04, η2 = .025. Female participants in the experimental group reported 32.5 fewer drinks at special occasions in the prior 3 months, compared with 18.9 for females in the control condition.
Peak Consumption During Special Occasion Drinking
Women in the MSB:Alcohol group experienced fewer binge drinking episodes during special occasions, compared with those in the control group, controlling for baseline consumption, F(1, 172) = 3.08, p = .08, a finding of borderline statistical significance. Men in both experimental groups decreased their binge episodes equally.
Alcohol-Related Problem Behavior
Results of the ANCOVA for the RAP scores at follow-up indicated that women in the experimental group reported significantly fewer negative consequences related to drinking than their control group counterparts (condition by gender, F[1, 212] = 4.00, p = .047, η2 = .019). Men in both groups reported similar RAPI scores at follow-up.
Readiness to Change
As the data in Table 2 demonstrate, the proportion of participants in the Action stage increased over time, but this change was not significantly different between groups. In the ANOVA and logistic regression analyses, we found no significant differences between groups on the number of stages of change or the proportion progressing through stages of change, respectively.
Moderators
Baseline Readiness to Change
We also explored baseline readiness to change as a potential moderator of primary drinking behavior outcomes. In an exploratory analysis, a significant, F(1, 82) = 3.88, p = .05, partial η2 = .045, quadratic within-group change revealed that low-motivation drinkers (Precontemplation stage) in the MSB:Alcohol group reduced their average consumption during a typical drinking week at a significantly faster rate 5.1 (4.4, 5.9) to 3.5 (2.2, 4.8) drinks, than low-motivation drinkers in the control group, 5.7 (5.1, 6.4) to 4.2 (3.1, 5.3), see Figure 4.
FIGURE 4.
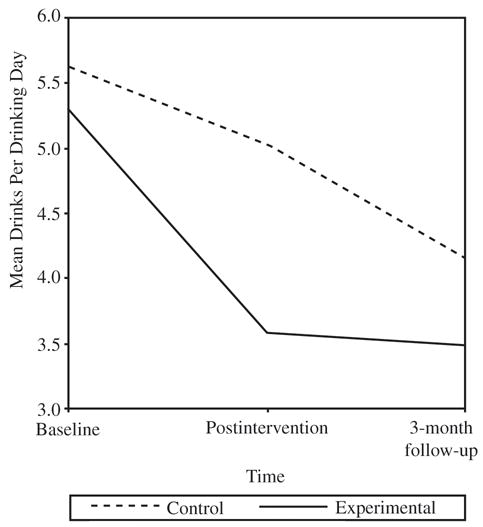
Mean drinks per drinking day among low-motivation drinkers (Precontemplation stage), by condition. be likely to refer friends to the site (45% vs 28% rated 5–7, z = 2.39, p = .02).
Site of Recruitment
We observed differences between sites, with some significant 2-way within-group quadratic change (ie, participants at some schools appeared to decrease their drinking at a faster rate than participants at other schools), but none differed between experimental groups. Site of recruitment was highly associated with several demographic variables, specifically gender and age. Including recruitment site, therefore, neither greatly influenced the models nor reduced overall variability. Thus, in the interest of parsimony, we did not include site in the repeated measures analyses.
Race and Age
Similarly, a dichotomized race variable (ie, White, non-White) suggested 2-way within-group quadratic changes (ie, non-White students seemed to reduce their drinking more quickly than White students), with no significant between-group differences. Age did not significantly moderate any of the observed differences between or within groups.
Student Evaluation of Intervention
When we dichotomized the ratings into 1 to 4 (poor to neutral) or 5 to7 (good to excellent), we found that students in the clinical trial indicated a significant difference in overall satisfaction with the MSB:Alcohol site compared with the control site (77% vs 65% rated 5–7, z = 2.35, p = .02). Significantly more users of the intervention rated the site as successful in addressing health issues relevant to college students (84% vs 64% rated 5–7, z = 3.30, p = .001). Relative to the reports of controls, significantly more MSB:Alcohol participants indicated that they would
COMMENT
We believe that this study represents the first randomized, controlled investigation of an Internet-based health program for college binge drinkers. The positive outcomes in our study suggest that MSB:Alcohol offers a potentially effective means of delivering brief interventions to college student binge drinkers.
Reductions in alcohol use occurred in all groups; however, MSB:Alcohol resulted in positive findings for 3 important subgroups—women, persistent heavy drinkers, and low-motivation drinkers. The female students who used this experimental intervention significantly reduced their peak and total consumption during special occasions and reported significantly fewer negative consequences related to drinking, compared with female students who used the control Web site.
The need for an effective intervention for college women has become more acute in recent years because rates of female and male students’ alcohol use are now comparable at the college level.5 In addition, some researchers provide evidence that women progress from regular alcohol use to abuse at faster rates than do men, are more likely to experience negative health consequences from alcohol consumption, and show the largest increases in drinking when making the transition from high school to college.5 A recent study found that college women decreased risky alcohol behaviors in response to a brief alcohol intervention (printed feedback reports) at a significantly greater rate than their male peers.41
In terms of persistent heavy drinkers, two thirds of the study participants reported that they were still drinking at follow-up. Compared with abstainers, these students were older, engaged in binge drinking more frequently, and drank more than they did at baseline. Despite their continued drinking, participants who received the MSB:Alcohol intervention showed evidence of significantly more rapid decreases in average and peak consumption and composite alcohol scores. Thus, it appears that the experimental intervention affected the rate of change in drinking. This group has been particularly difficult for college health educators to reach—they continue drinking despite repeated educational efforts. A harm-reduction approach seems most suited to these individuals, and our findings showing a change in the rate of drinking may represent an important first step in helping these students attain moderate drinking practices.
For students who were less willing to change their drinking behavior (low motivation), those who used the intervention reduced the number of drinks they consumed per day significantly faster than those in the control group. This is a key finding—a Web site designed to motivate student heavy drinkers should have an effect on those students who are most likely to resist change. However, because of the presence of multiple intervention components in the experimental intervention (educational, motivational, skill-building), it is not clear that the brief intervention feature (Rate Myself) accounted for the change. We can make no conclusive statements in the absence of a controlled component analysis of the Web site.
The positive outcomes with female participants in the MSB:Alcohol intervention may reflect a greater response among women than among men. Internet surveys suggest that women may be more active Internet health information seekers than men are and women are more likely than men are to base medical decisions on their searches.42 However, the high variability in the men’s alcohol use measures suggests that analysis by gender only may be inadequate in capturing the effects of the experimental intervention on college men’s student drinking. Future studies might consider using gender as a between-groups factor as well as exploring the heterogeneity of risk and alcohol use among college-aged men and women.
Our study adds to the existing literature in several important ways and has implications for program development and research methods. In terms of program development, these findings in this study support the feasibility of providing motivational interventions on a large-scale, anonymous basis. The drinking reductions achieved by MSB: Alcohol provide further support for motivational interventions that are used in other studies, albeit with more labor-intensive face-to-face and mail-based brief interventions.8–16 These results are important for college prevention programs because individual interventions can be delivered to the entire student population. This overcomes a potential barrier in the BASICS program, which relies on face-to-face intervention or mass mailings with identified students.
Less intrusive interventions, such as this experimental effort, might be essential for the two thirds of student heavy drinkers who do not recognize a need to change their drinking habits.43 In addition, students might be more responsive to a Web site that is designed specifically for their needs. Students’ evaluation data indicated that participants would be more likely to refer friends to the intervention than to the control Web site and that they regard the experimental intervention as more successful at addressing binge drinking as an important health problem.
In terms of methodology, we used a large sample that generated power to detect effects and to provide confidence that no significant findings represent nonexistent or negligible effects. The use of an ethnically diverse participant pool; systematic evaluation of gender effects; and the use of community, private, and public colleges suggests that positive results might be generalizable to different types of students and academic settings. Focusing on college students who actually exceeded the accepted criteria for binge drinking addresses outcomes in an important population.
These students may be more difficult to reach for alcohol prevention and education programs like MSB:Alcohol and more resistant to changing their behavior. Finally, the use of an online attention and activity control intervention suggests that the study’s positive effects may have resulted from the superiority of a brief intervention-based Web site rather than to a general student preference for an Internet-based format. Given the quality of the research-based educational materials provided to the control group, we found it noteworthy that those students rated the experimental intervention significantly higher in areas of content and message delivery.
Limitations
We should note several limitations to our study. First, some study sites manifested more outcome effects than others. Although we set strict intervention protocols and thoroughly trained staff to administer the assessment battery, some unknown or unmeasured environmental variables may explain this variance. This limitation does not affect the internal validity of the study, but suggests that there could be considerable variability in outcome effects among different types of colleges, student groups, and institutional settings. Second, the quality of the data we gathered depended on students’ self-reports, which may have influenced the categorization of problematic and binge drinking and recall of drinking episodes. In addition, we ran the study during a 6-month period and student self-reports may have been affected by academic, social, or seasonal events. However, we found no evidence of differential reporting across research groups. Third, a longer follow-up might allow firmer conclusions to be drawn about the stability of change. Future intervention studies may benefit from such extended follow-up.
Because Internet-based interventions are still in their infancy, it will be important for researchers to address additional questions in future research. What role does tailoring play in outcomes and which tailoring variables provide the most potent effects in an Internet-based format? How does MSB:Alcohol compare with a face-to-face BASICS program? Which elements are effective for particular subgroups (eg, women, heavier drinkers, or racial and ethnic groups)? Would the program have a greater effect if introduced at high-risk periods in a student’s college career (eg, at the beginning of the first year)? Interventions such as MSB:Alcohol expand the potential for motivational and tailored interventions, and spur important fundamental research to the betterment of college student health programs.
Acknowledgments
A Small Business Innovation Research Grant # 4R44AA12713-02 from the National Institute on Alcohol Abuse and Alcoholism (NIAAA) supported this work. The Inflexxion Institutional Review Board and the IRBs of the 5 participating colleges approved the study. We also acknowledge the assistance of Kim Fromme, PhD, University of Texas, who served as our primary consultant.
References
- 1.Wechsler H, Lee JE, Kuo M, et al. Trends in college binge drinking during a period of increased prevention efforts: findings from four Harvard School of Public Health study surveys, 1993–2001. J Am Coll Health. 2002;50:203–217. doi: 10.1080/07448480209595713. [DOI] [PubMed] [Google Scholar]
- 2.Wechsler H, Dowdal GW, Maenner G, et al. A gender-specific measure of binge drinking among college students. Am J Pub Health. 1995;85(7):982–985. doi: 10.2105/ajph.85.7.982. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Knight JR, Wechsler H, Kuo M, et al. Alcohol abuse and dependence among US college students. J Stud Alcohol. 2002;63(3):263–270. doi: 10.15288/jsa.2002.63.263. [DOI] [PubMed] [Google Scholar]
- 4.Hingson RW, Heeren T, Zakocs RC, et al. Magnitude of alcohol-related mortality and morbidity among US college students ages 18–24. J Stud Alcohol. 2002;63(2):136–144. doi: 10.15288/jsa.2002.63.136. [DOI] [PubMed] [Google Scholar]
- 5.Center on Addiction and Substance Abuse. The Formative Years: Pathways to Substance Abuse Among Women Ages 8–22. New York, NY: CASA Columbia; 2003. [Google Scholar]
- 6.Larimer ME, Cronce JM. Identification, prevention, and treatment: a review of individual-focused strategies to reduce problematic alcohol consumption by college students. J Stud Alcohol Suppl. 2002;14:148–163. doi: 10.15288/jsas.2002.s14.148. [DOI] [PubMed] [Google Scholar]
- 7.Walters ST, Bennett ME. Addressing alcohol use among college students: a review of the empirical literature. Alc Treat Q. 2000;18(1):61–77. [Google Scholar]
- 8.Baer JS, Kivlahan DR, Blume AW, et al. Brief intervention for heavy drinking college students: four-year follow-up and natural history. Am J Pub Health. 2001;91(8):1310–1316. doi: 10.2105/ajph.91.8.1310. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Agostinelli G, Brown JM, Miller WR. Effects of normative feedback on consumption among heavy-drinking college students. J Drug Educ. 1995;25(1):31–40. doi: 10.2190/XD56-D6WR-7195-EAL3. [DOI] [PubMed] [Google Scholar]
- 10.Walters ST. In praise of feedback: notes on an effective intervention for heavy drinking college students. J Am Coll Health. 2000;48:235–238. doi: 10.1080/07448480009599310. [DOI] [PubMed] [Google Scholar]
- 11.Collins SE, Carey KB, Sliwinski MJ. Mailed personalized normative feedback as a brief intervention for at-risk college drinkers. J Stud Alcohol. 2002;63(5):559–567. doi: 10.15288/jsa.2002.63.559. [DOI] [PubMed] [Google Scholar]
- 12.Dimeff LA, Baer JS, Kivlahan DR, Marlatt GA. Brief Alcohol Screening and Intervention for College Students. New York, NY: Guilford; 1999. [Google Scholar]
- 13.Murphy J, Duchnick J, Vuchinich R, et al. Relative efficacy of a brief motivational intervention for college student drinkers. Psych Addict Behav. 2001;15(4):373–379. doi: 10.1037//0893-164x.15.4.373. [DOI] [PubMed] [Google Scholar]
- 14.Roberts LJ, Neal DJ, Kivlahan DR, et al. Individual drinking changes following a brief intervention among college students. J Consult Clin Psych. 2000;68(3):500–505. doi: 10.1037//0022-006x.68.3.500. [DOI] [PubMed] [Google Scholar]
- 15.Borsari B, Carey KB. Effects of a brief motivational intervention with college student drinkers. J Consult Clin Psych. 2000;68(4):728–733. [PubMed] [Google Scholar]
- 16.Larimer ME, Turner AP, Anderson BK, et al. Evaluating a brief alcohol intervention with fraternities. J Stud Alcohol. 2001;62(3):370–380. doi: 10.15288/jsa.2001.62.370. [DOI] [PubMed] [Google Scholar]
- 17.Dimeff LA, McNeely M. Computer-enhanced primary care practitioner advice for high-risk college drinkers in a student primary health–care setting. Cognitive Behav Pract. 2000;7(1):82–100. [Google Scholar]
- 18.Walters ST. [accessed 10/23/03];e-CHUG http://www.e–chug.com.
- 19.Task Force on College Drinking. A Call to Action: Changing the Culture of Drinking at US Colleges. Bethesda, MD: National Institute on Alcohol Abuse and Alcoholism; 2002. [Google Scholar]
- 20.Black DR, Coster DC. Interest in a Stepped Approach Model (SAM): identification of recruitment strategies for university alcohol programs. Health Ed Q. 1996;23(1):98–114. doi: 10.1177/109019819602300107. [DOI] [PubMed] [Google Scholar]
- 21.Paperny DM, Ayono JY, Lehman RM, et al. Computer–assisted detection and intervention in adolescent high-risk health behaviors. J Pediatrics. 1990;116(3):456–462. doi: 10.1016/s0022-3476(05)82844-6. [DOI] [PubMed] [Google Scholar]
- 22.Turner CF, Ku L, Rogers SM, et al. Adolescent sexual behavior, drug use, and violence. Science. 1998;280(5365):867–873. doi: 10.1126/science.280.5365.867. [DOI] [PubMed] [Google Scholar]
- 23.Kaiser Family Foundation. Generation Rx.com: How young people use the Internet for health information. [accessed March 27, 2003];http://www.kff.org/content/2001/20011211a/GenerationRx.pdf.
- 24.DeJong W. Finding common ground for effective campus-based prevention. Psych Addict Behav. 2001;15(4):292–296. doi: 10.1037//0893-164x.15.4.292. [DOI] [PubMed] [Google Scholar]
- 25.Johnston LD, O’Malley PM, Bachman JG. NIH Publication No. 02–5107. Bethesda, MD: National Institute on Drug Abuse; 2002. Monitoring the Future National Survey Results on Drug Use, 1975–2001 Volume II: College Students and Adults Ages 19–40. [Google Scholar]
- 26.Presley CA, Leichliter JS, Meilman PW. Alcohol and Drugs on American College Campuses: Findings From 1995, 1996, and 1997. Carbondale, IL: Southern Illinois University; 1999. [Google Scholar]
- 27.Wei LJ. An application of an urn model to the design of sequential controlled trials. J Am Stat Assoc. 1978;73:559–563. [Google Scholar]
- 28.Fromme K, Stroot E, Kaplan D. Comprehensive effects of alcohol: development and psychometric assessment of a new expectancy questionnaire. Psych Assess. 1993;5(1):19–26. [Google Scholar]
- 29.Fromme K, Katz E, Rivet K. Outcome expectancies and risk-taking behavior. Cognitive Ther Res. 1997;21(4):421–442. [Google Scholar]
- 30.White HR, Labouvie EW. Toward the assessment of adolescent problem drinking. J Stud Alcohol. 1989;50(1):30–37. doi: 10.15288/jsa.1989.50.30. [DOI] [PubMed] [Google Scholar]
- 31.Miller WR. Alcohol and you. In: Miller WR, Zweben A, DiClemente CC, et al., editors. Motivational Enhancement Therapy Manual. Rockville, MD: NIAAA; 1995. pp. 101–107. [Google Scholar]
- 32.NIAAA. How to Cut Down Your Drinking. Bethesda, MD: NIAAA; 1996. [Google Scholar]
- 33.NIAAA. Alcohol: What You Don’t Know Can Harm You. Bethesda, MD: NIAAA; 2002. [Google Scholar]
- 34.NIAAA. Alcoholism: Getting the Facts. Bethesda, MD: NIAAA; 2001. [Google Scholar]
- 35.Sobell LC, Sobell MB. Alcohol Timeline Followback User’s Manual. Toronto, Canada: Addiction Research Foundation; 1995. [Google Scholar]
- 36.White HR, Labouvie E. Rutgers Alcohol Problem Index (RAPI) Piscataway, NJ: Center of Alcohol Studies, Rutgers University; 1989. [Google Scholar]
- 37.Rollnick S, Heather N, Gold R, Hall W. Development of a short “Readiness to Change” Questionnaire for use in brief opportunistic interventions. Br J Addict. 1992;87(5):743–754. doi: 10.1111/j.1360-0443.1992.tb02720.x. [DOI] [PubMed] [Google Scholar]
- 38.Rossi JS. Analysis of Stage of Change: Summary and Recommendations for BCC. Kingston, RI: Cancer Prevention Research Center, University of Rhode Island; 2000. [Google Scholar]
- 39.SPSS, Inc. SPSS for Windows, Rel. 11.5.1. Chicago: SPSS Inc; 2002. [Google Scholar]
- 40.Schafer JL, Graham JW. Missing data: our view of the state of the art. Psych Methods. 2002;7(2):147–177. [PubMed] [Google Scholar]
- 41.Saunders JB, Kypri K, Walters ST, Laforge RG, Larimer ME. Approaches to brief intervention for hazardous drinking in young people. Alcoholism: Clin Exp Res. 2004;20:322–329. doi: 10.1097/01.alc.0000113418.12889.08. [DOI] [PubMed] [Google Scholar]
- 42.Pew Internet and American Life Project. The Online Health Care Revolution. Washington, DC: Pew Internet and American Life Project; 2000. [Google Scholar]
- 43.Vik PW, Culbertson KA, Sellers K. Readiness to change drinking among heavy-drinking college students. J Stud Alcohol. 2000;61(5):674–680. doi: 10.15288/jsa.2000.61.674. [DOI] [PubMed] [Google Scholar]