

Abstract
Recently, the authors have used the computer generated three-dimensional (3-D) CT moving images for preoperative planning and screw/pin insertion in more than 28 cases involving plate and screw fixation of complex acetabular fractures. The authors also used stereolithography (wax or plastic 3-D model of bony anatomy) to develop a computer-generated "clip on" interpositioning template for accurate placement of plate and screws. Application of these new technologies gives the surgeon precise information about the fracture patterns and provides an effective means for preoperative planning and accurate fixation of acetabular fractures. The accuracy of the 3-D virtual presentation of the anatomy is impressive and was substantiated by phantom studies. Postoperation CT revealed no case of screw penetration in the joint. Among other benefits over conventional surgical technique, the computer-assisted surgery provided decreased operative time and morbidity, decreased radiation exposure, and obviated the need for oblique, inlet and outlet roentgen views of the pelvis for preoperative planning. A case report specifically demonstrates preoperative planning for reconstruction of acetabular fracture.
INTRODUCTION
Recent studies emphasize the need for improvement over less-than-ideal techniques presently used in orthopaedic surgery for insertion of surgical implants.2, 8, 11 The placement of screws with inadvertent penetration of the hip joint has been well documented both for complex acetabular fractures and posterior wall fractures.1, 5 A technique for precise plate and screw placement requires knowledge of the three-dimensional anatomy of the patient. Surgeons cannot be expected to improve without accurate evaluation of their performance.
Orthopaedic surgeons are just beginning to consider the advantages of the computer in three-dimensional guidance for insertion of pins, screws and correction of the bony anatomy. Advances in radiology combined with the advances in computer technology have made the 3-D representation of anatomic structures in living subjects easily obtainable using CT and MRI. Despite these advances, the application of this technology for improving surgical precision in orthopaedic procedures has not yet been widely applied to clinical practice. Computer-assisted surgery has been utilized for such procedures as pedicle screw placement in spine surgery, total joint arthoplasty, knee ligament reconstruction, percutaneous fixation of minimally displaced transverse acetabular fractures, anterior column fractures and iliosacral fractures.2–4, 7, 10, 11, 14–16 Surgical applications using arising technologies in stereolithography (wax or plastic 3-D model of bony anatomy) have recently been explored in other specialty areas such as maxillofacial surgery.9, 12, 13, 17, 19
Recently, the authors have used computer image guidance for preoperative planning and screw/pin insertion in more than 28 cases involving plate and screw fixation of complex acetabular fractures.2 The authors also used stereolithography to develop a computer-generated "clip on" interpositioning template for accurate placement of plate and screws. The templates can be used, among many other applications, for surgery of the spine, pelvis and bones of the extremity. In the past two years the authors have been working closely with the Human Assisted Technology Division of the Sandia National Laboratory on techniques to replicate the exact bony anatomy using sterolithography-modeling technologies.
In this study we first report on the advantages of the computer-generated 3-D moving representations of the bony anatomy over traditional x-ray evaluation in surgery of the acetabulum. This will be followed with a case report that specifically demonstrates preoperative planning for reconstruction of acetabular fracture. This case report will also demonstrate a technique to produce total hip replacement acetabular components with personalized template guidance. A system like this may increase the indications for primary total hip arthroplasty after acetabular fracture, recently outlined by Mears and Velyvis,20 by improving techniques for component stabilization.
MATERIALS AND METHODS
This study used computer-generated 3-D moving representations of the bony anatomy to plan the screw trajectories and to carry out the surgical stabilization procedure after fracture reduction. A preoperative 3mm spiral CT scan of the pelvis was obtained using a Picker CT 5000 scanner. The images were transferred via Picker 2000 workstation and Exabyte 820 tape drive to a personal computer. Materialise Interactive Medical Image Control System (MIMICS) software (Materialise USA, Ann Arbor, MI) allows interface of the 3-D CT information with the stereolithography equipment to produce a plastic/wax model of the deformed or fractured bony anatomy. In addition, the software has segmentation capabilities that were used to subtract the proximal femurs and extraneous bowel or bladder dye. The accuracy of the 3-D virtual presentation of the anatomy was substantiated by a phantom study. Multiple 2mm lead spheres (BBs) were glued to the pelvic surface, and the model was CT scanned using standard 3mm helical collection of data. The computer data was transferred into the ViewPoint/Voyger™ Image Guidance System, and both 4.0 and 6.0 versions of the software were tested for accuracy of the predicted target registration error.6
The authors also used stereolithography to develop a computer-generated "clip on" interpositioning template for accurate placement of plate and screws. The implant positioning template was designed based on creation of mirror image of the 3-D computer representations of the patient's anatomy along with virtual surgery procedure, and the template was fabricated from methyl methacrylate using rapid prototyping techniques. This template was then placed on the patient's anatomy as a guide to precisely locate and direct the hardware (implant) into the bony structure. Because the template would fit the patient's anatomy, the surgeon would have a hands-on simple method of guiding surgical tools in 3-D space.
The ability to create proposed trajectories for screw insertion prior to surgical intervention has become a standard for stabilization of acetabular fractures in the senior author's practice. The current image-guided surgical equipment, such as the ViewPoint/Voyger™ IGS (Z-KAT, Inc., Florida), provides capabilities for virtual creation of these trajectories. The Picker 2000 and 6000 workstations give adequate 3-D representations of the anatomy, but segmentation is not as easy and trajectory planning is not a true option.
Screw trajectory planning was performed using two of the object features of the MIMICS software. The point feature was used to select entrance and target points on each fracture fragment. This provides x, y, z location of these two points in the 2-D and 3-D CT data and can be modified in increments of 0.001 mm. The trajectories were created by transferring the x, y, z location of the two points to the cylinder creation option of the software. This would create a cylinder of a desired radius (3mm in the case report) connecting the entrance and target points. Lengthening the trajectories, as is shown in this example case, is possible through data extrapolation.
CASE STUDY
A 30-year-old male fell 30 feet, sustaining a transverse and posterior hemitransverse and anterior column acetabular fracture-classified as a 62-B3.3,a1 type fracture by the Orthopaedic Trauma Association.18 In addition to the fixation obtained from the screws inserted in pre-assigned trajectories, a pre-contoured plate was used to further stabilize the anterior column, and two percutaneous screws were inserted into the superior fracture fragment. The virtual acetabular replacement trajectories suggested by Figures 3B and 4A, 4B, 4C were not used in the fixation of this young 30-year-old patient but would be a consideration if this patient were to be treated with total hip replacement. The ideal radius for the spherical acetabular replacement cup was taken from the contralateral nonfractured acetabulum and was matched to the radius of the remaining arc of the fracture segments on the fractured side. The virtual screw trajectories were created using the x, y, z location of the center of the sphere as the entrance point, and the x, y, z locations of the target points were chosen in the most secure location within each of the fractured segments. All three trajectories were aimed toward the center of the acetabular component while maximizing fixation within each of the major fracture fragments.
Figure 3.
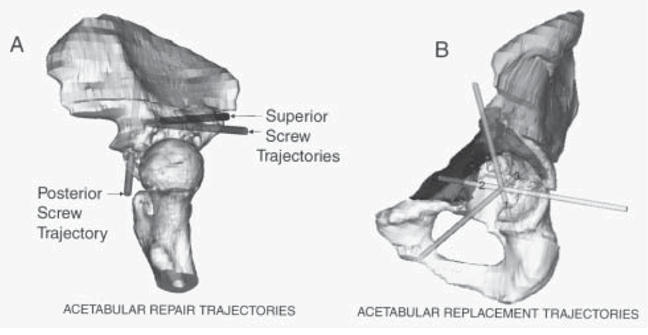
Isolated views of hemisphere pelvis demonstrating proposed trajectories for acetabular repair and acetabular replacement. (A) Enlarged views of the three proposed repair screw trajectories. The ischial and anterior column segments are removed and the proximal femur reinserted to demonstrate that all screw trajectories would easily be extra-articular after fracture reduction. (B) Transfemoral head view of the fractured acetabulum to show the three proposed trajectories for fixation if a primary total hip replacement would have been considered for this patient.
Figure 4.
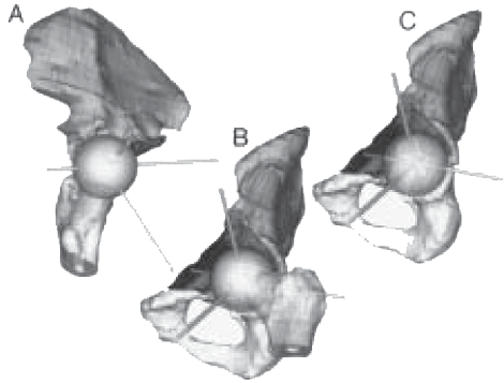
Three rotated views of the segmented rendered 3-D pelvis with a sphere representing the proposed size and ideal location for an acetabular replacement component. (A) Same view as Figure 3A with proposed acetabular replacement trajectories instead of acetabular repair trajectories. (B) Same view as Figure 3B with sphere and femoral head. (C) Same view as Figure 3B with femoral head removed.
RESULTS
Figure 1 is a rendered 3-D image of the segmented pelvis with a left acetabular fracture dividing the joint into four parts. Rotation and segmentation capabilities of the 3-D data allowed precise understanding of the fracture anatomy before surgery. This eliminated the need for oblique, inlet and outlet roentgen views of the patient prior to surgery. The accuracy of the 3-D virtual presentation of the anatomy was impressive and was substantiated by the phantom study.6 Computer predicted target registration error was a close representation of the actual error for predicted target registration error values of less than 2mm.2, 6
Figure 1.
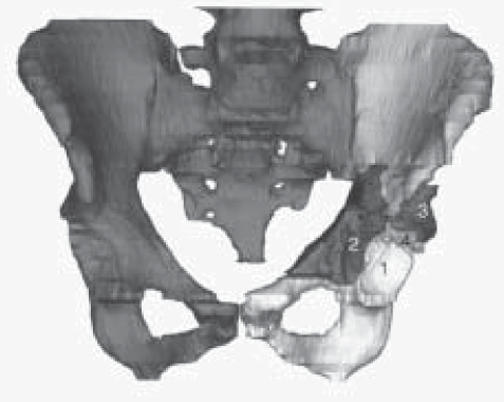
Rendered 3-D CT images of the pelvis from the case patient who fell 30 feet, sustaining a transverse and posterior hemitransverse and anterior column acetabular fracture. The four components of the fracture are (1) ischial, (2) anterior column, (3) superior wall and (4) iliac. Bowel and bladder dye and both proximal femurs are removed to better demonstrate the fracture.
In all cases, intraoperative postfixation fluoroscopy confirmed the precise plate placement and demonstrated that the screw trajectories missed the hip joint by a safe distance. The accuracy of plate and screw placement supports the technique of using computer reversed contralateral intact anatomy and application of the interpositioning template. Fluoroscopy was only needed for confirmation of fracture reduction and screw location. Post-operation CT also revealed no case of screw penetration in the joint. Furthermore, the software capabilities easily allowed elimination of the metal artifact. Among other benefits over conventional surgical technique, the computer-assisted surgery provided decreased operative time and morbidity, decreased radiation exposure,2 and obviated the need for oblique, inlet and outlet roentgen views of the pelvis for preoperative planning.
DISCUSSION
Accurate reduction of fractures, smaller incisions and less invasive techniques for surgery have universal appeal from the patient's aspect and have been shown quite advantageous for patient care. Application of computer-generated 3-D CT moving images and fixation trajectory planning for complex acetabular fractures gives the surgeon precise information about the fracture patterns and provides an effective means for preoperative planning and accurate fixation of acetabular fractures. It also helps to better fix acetabular components used for reconstruction when total hip replacement is needed.
The authors have used computer-generated 3-D moving representations of the bony anatomy to plan screw trajectories and to carry out surgical stabilization procedures after fracture reduction in patients with complex acetabular fractures. In more than 50 consecutive cases, intraoperative evaluation of the fracture patterns has confirmed the improvement in this technology over those obtained using traditional radiology techniques. Intraoperative fluoroscopy confirmed precise plate placement and demonstrated that all screw trajectories missed the hip joint. Fluoroscopy time during surgery was reduced significantly because it is only needed for confirmation of fracture reduction and screw location. The accuracy of the 3-D virtual presentation of the anatomy using 3-D CT is impressive and has a number of benefits when compared to conventional surgical technique. The computer-assisted surgery provides decreased operative time and morbidity, decreased fluoroscopic radiation exposure during surgery,2 and obviates the need for oblique, inlet and outlet roentgen views of the pelvis for preoperative planning.
A number of image-guided surgical systems now offer implant trajectory guidance and segmentation capabilities. The MIMICS software, which was developed as an interface between the CT/MRI data and solid model producing (rapid prototyping) equipment, is quite useful for preoperative planning. Postoperatively, the software provides precise 3-D moving visualization of the metal hardware location within the anatomic structure. Furthermore, it allows elimination of the metal artifact. We are currently using life-size wax stereolithographic replicas of the fractured pelvis, interpositioning screw trajectory guidance templates, and computer models of the reversed nonfractured contralateral hemi-pelvis for reconstruction of all surgically treated acetabular fractures with excellent results.
Figure 2.
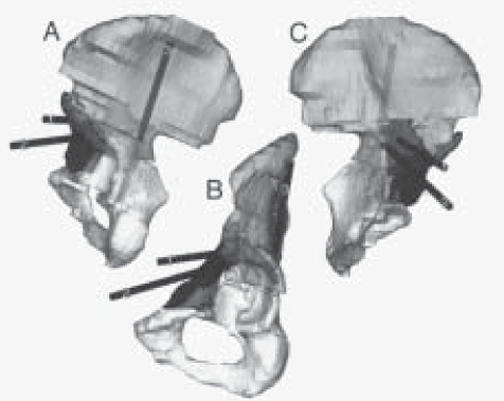
Three rotated rendered 3-D CT images of the case study pelvis. Further segmentation allowed removal of the sacrum and contralateral hemi-pelvis. Three proposed screw trajectories (labeled 1, 2 and 3) have been added to the images and are visible through the translucent bone.
(A) Posterior view. (B) Transfemoral head inferior-lateral view. (C) Medial view. (1) Superior-posterior screw trajectory, (2) Superioranterior screw trajectory, (3) Posterior column screw trajectory.
ACKNOWLEDGMENTS
The authors would like to thank Mark K. Crawford, M.D., Thomas A. DeCoster, M.D., and Moheb S. Moneim, M.D., for their contributions during the course of this study. The authors are also indebted to Clinton L. Atwood, Mark Ensz, Ph.D., and Daryl Reckaway, Ph.D., from Sandia National Laboratory for their technical assistance in fabrication of the stereolithographic models of the patient's pelvis and the interpositioning templates.
Footnotes
This study was supported, in part, by the Dedicated Health Research Funds of the University of New Mexico School of Medicine.
Part of this study was presented at the Fifth Biennial Johnston Lectureship in Hip Reconstruction, University of Iowa Hospitals and Clinics, Iowa City, Iowa, October 20-21, 2000.
Part of this study was accepted for presentation at the 1st Annual Meeting of International Society for Computer Assisted Orthopaedic Surgery (CAOS), Davos, Switzerland, February 7-10, 2001.
References
- 1.Baumgaertner MR. Fractures of the Posterior Wall of the Acetabulum. J Am Acad Orthop Surg. 1999;7:54–65. doi: 10.5435/00124635-199901000-00006. [DOI] [PubMed] [Google Scholar]
- 2.Brown GA, Willis M, Firoozbakhsh K, Barmada A. Computed Tomography Image Guided Surgery in Complex Acetabular Fracture. Clin Orthop Rel Research. 2000;370:219–226. doi: 10.1097/00003086-200001000-00022. [DOI] [PubMed] [Google Scholar]
- 3.Brown GA, Firoozbakhsh K, Willis M, Milner B. Advances of Computer-Assisted Surgery in Complex Acetabular Fracture and Intramedullary Nailing. Poster #PE112; AAOS 68th Annual Meeting; 2001. [Google Scholar]
- 4.Brown GA, Willis M, Firoozbakhsh K, Barmada A. Image-Guided Surgery in Complex Acetabular Fractures and in Percutaneous Placement of Iliosacral Screws Using the ViewPoint System. Syllabus CAOS/USA. 1999. pp. 155–161.
- 5.Browner BD, Helfet DL. Internal Fixation of a Fractured Acetabulum. Strategies in Orthopaedic Surgery. 1991;10(2):1–16. [Google Scholar]
- 6.Firoozbakhsh K, Brown GA, Milner B. Pelvis Image-Guided Surgery Phantom Study. Poster #0974; 47th Annual Meeting of Orthopaedic Research Society; 2001. [Google Scholar]
- 7.Glossop ND, Hu RW, Steven D, Randle J. Image Guided Placement of Iliosacral Lag Screws. Computer Assisted Orthopedic Surgery. CAOS/USA Syllabus. 1998. pp. 184–186.
- 8.Hoppenfeld S, Deboer P. Philadelphia: JB Lippincott Company; 1984. Surgical Exposures in Orthopaedics: The Anatomic Approach; pp. 327–343. [Google Scholar]
- 9.Kaci GM, Zanetti M, Amgwerd M, Trentz O, Seifert B, Stucki H, Holder J. Rapid Prototyping (Stereolithography) in the Management of Intra-Articular Calcaneal Fractures. European Radiology. 1997;7(2):187–191. doi: 10.1007/s003300050132. [DOI] [PubMed] [Google Scholar]
- 10.Kahler DM, Zura R. Evaluation of a computer integrated surgical technique for percutaneous fixation of tranverse acetabular fractures. Lecture notes. Comput Sci. 1997;1205:565–572. [Google Scholar]
- 11.Kahler DM. Early Experience with Computer Assisted Technique for Iliosacral Screw Placement in Posterior Pelvic Ring Disruptions. Computer Assisted Orthopedic Surgery. CAOS/USA Syllabus. 1998. pp. 180–182.
- 12.Kelly PJ. Volumetric Stereotactic Surgical Resection of Intra-axial Brain Mass Lesions. Mayo Clin Protocol. 1988;63:1186–1198. doi: 10.1016/s0025-6196(12)65405-6. [DOI] [PubMed] [Google Scholar]
- 13.Keman BT, Wimsatt JA. Use of a Stereolithography Model for Accurate Preoperative Adaptation of a Reconstruction Plate. J Oral Maxil Surg. 2000;58(3):349–351. doi: 10.1016/s0278-2391(00)90071-5. [DOI] [PubMed] [Google Scholar]
- 14.Langlotz F, Stucki M, Bachler R, Scheer C, Ganz R, Berlemann U, Nolte L. The First Twelve Cases of Computer Assisted Periacetabular Osteotomy. Comp Aid Surg. 1997;2:317–326. doi: 10.1002/(SICI)1097-0150(1997)2:6<317::AID-IGS1>3.0.CO;2-2. [DOI] [PubMed] [Google Scholar]
- 15.League D. Interactive image-guided stereotactic neurosurgery systems. AORN J. 1995. pp. 360–370. [DOI] [PubMed]
- 16.MacDonald SJ, Hersche O, Ganz R. Periacetabular Osteotomy in Treatment of Neutrogena Acetabular Dysplasia. JBJS. 1999;81-B:6. doi: 10.1302/0301-620x.81b6.9700. [DOI] [PubMed] [Google Scholar]
- 17.Migaud H, Cortet B, Assaker R, Fontaine C, Kulk JF, Duquennoy A. A Value of a Synthetic Osseous Model Obtained by Stereolithography for Preoperative Planning. Correction of a Complex Femoral Deformity Caused by Fibrous Dysplasia. Rev Chir Orthop Repractice Appar Mot. 1997;83(2):156–159. [PubMed] [Google Scholar]
- 18.Orthopaedic Trauma Association Committee for Coding and Classification. Fracture and Dislocation Compendium. J of Orthopaedic Trauma. 1996;10(1):71–75. [PubMed] [Google Scholar]
- 19.Thomas W, Schuster C, Schuster L. Custom-made Knee Endoprosthetics Using Subtraction Data of 3-D CT Scans. A New Approach. Orthopedics. 2000;29(7):641–644. doi: 10.1007/s001320050505. [DOI] [PubMed] [Google Scholar]
- 20.Mears DC, Velyvis JH. Primary Total Hip Arthroplasty after Acetabular Fracture. J Bone Joint Surg. 2000;82(A):1328–1353. [Google Scholar]