

Abstract
Parents have traditionally relied on health care professionals for advice and treatment for most orthopaedic conditions, including clubfoot. However, the unprecedented access to health care information offered by the Internet is changing how parents gather information and make treatment choices. This study was designed to evaluate the effect of the Internet in the treatment of clubfoot. We performed a retrospective review of the clinical census, statistics of the Virtual Hospital web pages on clubfoot, web sites, and web based support-groups related to clubfoot from 1995 to 2002. There were 157 patients that came to our clinic for treatment, a dramatic increase compared to previous years. There were a total of 790,084 hits to the Virtual Hospital web pages, with information requested from all states and 72 countries. Interestingly, the referrals also changed with patients coming from 30 states and 8 different countries, compared to previous years when the majority came from our own state. In addition, 75% of the patients were self-referred, many of them while on treatment at outside institutions. There were 160 web sites providing information on clubfoot and 5 large support groups. There were approximately 30,000 messages (average 1000 messages/month) posted into the support clubfoot websites. After visiting Internet support groups, 125 parents transferred or initiated the care of their children to a doctor practicing the Ponseti method. In conclusion, the Internet provides a mean for parents to obtain disease-specific information in a timely manner. Parents used the support-groups to find and proffer information, share experiences and opinions, and provide encouragement. This sharing of information is affecting how parents make their treatment choices and also has the potential to induce unexpected changes in clinical orthopaedic practice.
INTRODUCTION
The digitalization of information, the ability to network, and the rapid electronic interchange of information on a worldwide basis are recognized hallmarks of today's society. The Internet, with 130,000,000 users and growing at a rate of 2% per month, is a global, independent but cooperative network system that allows remote access to data and permits its quick access in unprecedented volume.
The world of medicine has not escaped the impact of the Internet, and health-related sites are among the most frequently accessed information resources. A recent survey indicated that 70,000,000 US adults had accessed the Internet to obtain health or medical information in 200118. At least 100,000 health and medical sites are on the World Wide Web, and are maintained by entities ranging from academic medical centers and professional organizations to individuals. Thousands of other online self-help and support groups, bulletin boards, and mailing lists also are available. However, how this unprecedented access to health care information is affecting the way parents make decisions on treatment options, and how those decisions could impact clinical practice are not well understood3–6,13,16,17. Interestingly, in 1998, a web page with information on the treatment of clubfoot as described by Ponseti was posted in the Virtual Hospital of the University of Iowa. Since then, we have witnessed a dramatic change in our referral patterns. This study was designed to evaluate the effect of the Internet in clubfoot clinical practice at our institution and how web-based information and supports groups influence parent choices for the treatment of clubfoot.
MATERIALS AND METHODS
We performed a retrospective reviewed of the clinical census at our institution for the diagnosis of clubfoot from January 1991 to December 2001. Demographic data was evaluated with respect to living address, referral entity (self-referral or physician referral), age of the patient at presentation, previous treatment and type of treatment at the outside institution. We also performed a review of the statistics of the Virtual Hospital web pages for the treatment of clubfoot. Total number of hits, number of pages visited, and total visits were recorded. In addition, location of the request was also recorded.
We also performed a review of the public web sites providing information on clubfoot, as well as parent-support groups for clubfoot from October 1998 to December 2001. From the 5 most active sites, total number of members, new members per month, and total number of messages posted were recorded. In addition, evaluation of the content of the messages was performed, specifically information on decision making by the parents about treatment choices.
RESULTS
From the initial posting of the web pages on clubfoot in the Virtual Hospital in October 1998 through December 2001, there were 790,084 hits, with an average of 27,334 hits/month (Figure 1). Information was requested from all states and 72 countries. These included countries such as India, Singapore, Spain, Egypt, Australia, etc.
Figure 1.
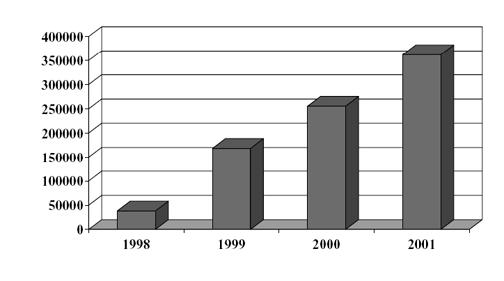
Number of hits at the Virtual Hospital clubfoot web page. Note the increase over the short period of time, to a total of 790,084.
When evaluating patient referrals to the clinic, we observed there was an increase in the number of patients per year that paralleled the hits to the Virtual Hospital clubfoot web pages (Figures 1 and 2). In the years prior to 1998, there were an average of 5 patients seen in clinic by the senior author (IVP). This number increased to about 60 patients per year by 2001 (for a total of 157 patients). Interestingly, 75% of patients attending the clinic were self-referrals, with 71% having had treatment or currently on treatment at an outside institution.
Figure 2.
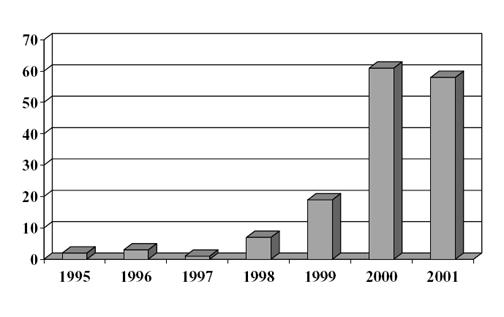
Number of patients seen in clinic from 1995 to 2001. Note the dramatic increase since 1998 when the Virtual Hospital clubfoot web pages were posted.
Age at presentation demonstrated a significant difference between pre and post Internet web page posting. Patients in the early 90's were seen usually in their first month of life. After 1998, the average age at presentation was 3 months, with a range from newborn to 22 months of age. Eighteen per cent of the patients were older that 6 months at presentation (data not shown).
With regard to the parents-support groups, there were over 160 web sites providing information on clubfoot and 5 large support groups. There are sites and support groups for General Information, Surgery, Ponseti method, French Physiotherapy method, as well as parental sites in the UK, Australia, France, Germany and other countries. In the past few years, the fastest growing sites and topics have been related to conservative methods such as the Ponseti method (Figure 3). We have observed an increased number of people using group sites to obtain information and advice, with the growth of 40 new members per month.
Figure 3. Total number of members at Internet sites.
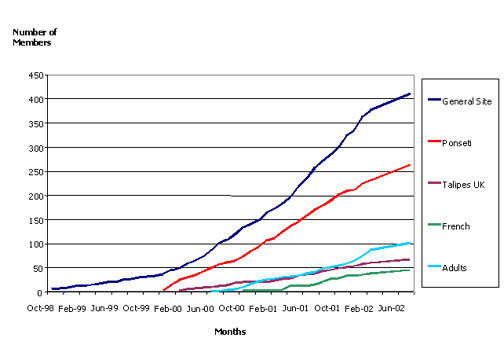
Note the exponential increase in the number in the general web sites and in the Ponseti method.
There were approximately 30,000 messages (average 1,000 messages/month) posted on these websites and the messages are publicly available (Figure 4). Compared to the other sites, the Ponseti site had the greatest increase in number of messages. Importantly, after visiting the support groups and talking with active members in the groups, 125 parents brought their children to our institution, or to another institution where there are professionals practicing the Ponseti method. Interestingly, only 3 of these children required extensive corrective surgery after they were treated by the Ponseti method.
Figure 4.
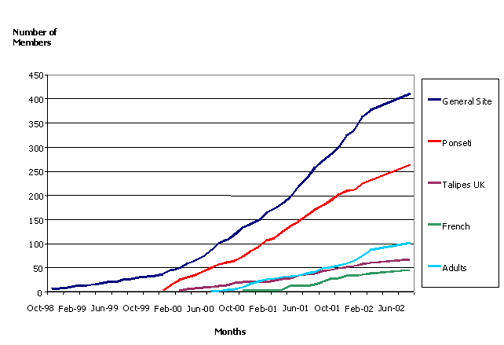
Number of messages posted at the different web sites. Note the correlation between the number of messages in the general site and the Ponseti web site (four months weighted average).
DISCUSSION
The results of this study, using clubfoot as a model, demonstrate that the Internet can have a profound effect in clinical practice patterns, and in the patient physician relationship. Since the introduction of information about clubfoot on the Virtual Hospital by the senior author (IVP), we have seen a dramatic increase in the number of patients attending our clinic, with the majority of them coming from out of state and a significant number having been treated at an outside institution. In addition, general information and parent support groups for clubfoot have grown almost exponentially. Importantly, many parents decided to change treating physicians after consulting and sharing information on the web.
Increasing use of the Internet by consumers in general is being reflected in greater reliance on this medium for health information and health care. In part, the use of the Internet to find answers to health-related questions has been linked to several issues affecting existing practice patterns. Many people are using the Internet due to the belief that today's doctor-patient relationship lacks attention to detail and the personal touch that was present in the past. Patients also desire more involvement in and control over the management of their own health. Furthermore, there are alternatives to traditional providers and methods of treatment, and patients can not only find them on the Internet, but also retrieve information that is stated objectively and many times, non-technically. Finally, the Internet also offers a means to get a "second opinion" without the hassles of a referral and can provide a way to communicate with others patients or families in similar situations or with similar problems3–6,13,16,17.
In the case of clubfoot, several of these issues seemed to be responsible for the changes observed in our practice. Until recently, non-surgical methods of correction have demonstrated a low success rate, with up to 90% of the patients requiring extensive corrective surgery. However, clubfoot surgery is frequently associated with persistent stiffness of the foot, and may lead to many complications (up to 25% of cases) and the need for secondary procedures (up to 47% of cases). Acceptance of these poor results, however, has been the "norm" because clubfoot has been viewed as a surgical deformity, very difficult to correct1,2,7,9,10,11,12,14,15, 19,20,23–28.
Given that the results of surgical treatment can be so discouraging, parents looked for alternative treatments. Traditionally, parents would have relied on health care professionals for advice and treatment. However, the development of the Internet and the explosion of health care information allowed them to obtain disease-specific information in a timely manner. In addition, parents created and actively used Internet support- groups on clubfoot to find and proffer information, share experiences and opinions, and provide encouragement to other parents.
From information available through the Internet, parents became aware of the Ponseti method, and of the controversy that existed over the need or not for extensive surgical treatment for the correction of the deformity. Interestingly, clubfoot is a very "visual" deformity, i.e., it is very easy for the parents to see and assess the results of any treatment. The fact that the Ponseti method allows full correction of the deformity in a very short period of time and without the need for extensive surgery is of critical importance8,21,22. Parents realized the benefit of this treatment modality and share their experience with others. As a result, the number of messages on the Ponseti method at the different clubfoot web sites and parents support groups increased exponentially. This also resulted on many parents transferring the care of their child to a physician with knowledge on the Ponseti method (75 % of our referral population and 125 parents in the support groups).
In conclusion, the Internet provides a mean for parents to obtain disease-specific information in a timely manner. Parents use the support-groups to find and proffer information, share experiences and opinions, and provide encouragement. This sharing of information is affecting how parents make their treatment choices and also has the potential to induce unexpected changes in clinical practice. The implications of these effects deserve further investigation.
Footnotes
Investigation performed at the Department of Orthopaedic Surgery, University of Iowa, Iowa City, IA
References
- 1.Aronson J, Puskarich CL. Deformity and disability from treated clubfoot. J Pediatr Ortho. 1990;10:109–112. [PubMed] [Google Scholar]
- 2.Atar D, Lehman WB, Grant AD. Complications in clubfoot surgery. Orthop Rev. 1991;20:233–239. [PubMed] [Google Scholar]
- 3.Bader SA, Braude RM. "Patient Informatics": creating new partnerships in medical decision making. Acad Med. 1998;73:408–411. doi: 10.1097/00001888-199804000-00014. [DOI] [PubMed] [Google Scholar]
- 4.Ball MJ, Lillis J. E-health: transforming the physician/patient relationship. Int J Med Inf. 2001;61:1–10. doi: 10.1016/s1386-5056(00)00130-1. [DOI] [PubMed] [Google Scholar]
- 5.Beall MS, Golladay GJ, Greenfield ML, Hesinger RN, Biermann JS. Use of the Internet by Pediatric Orthopaedic outpatients. J Ped Ortho. 2002;22:261–264. [PubMed] [Google Scholar]
- 6.Blumenthal D. Doctors in a wired world: can professionalism survive connectivity? Milbank Q. 2002;80:525–546. doi: 10.1111/1468-0009.00021. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Bradish CF, Noor S. The Ilizarov method in the management of relapsed club feet. J Bone Joint Surg. (Br) 2000;82:387–391. doi: 10.1302/0301-620x.82b3.9689. [DOI] [PubMed] [Google Scholar]
- 8.Cooper DM, Dietz FR. Treatment of Idiopathic Clubfoot. A thirty-year follow-up. J Bone Joint Surg. (Am) 1995;77:1477–1489. doi: 10.2106/00004623-199510000-00002. [DOI] [PubMed] [Google Scholar]
- 9.Crawford AH, Gupta AK. Clubfoot controversies: complications and causes for failure. Instr Course Lect. 1991;45:339–346. [PubMed] [Google Scholar]
- 10.Crawford AH, Marxen JL, Osterfeld DI. The Cincinnati incision: A comprehensive approach for surgical procedures of the foot and ankle in childhood. J Bone Joint Surg. (Am) 1982;64:1355–1358. [PubMed] [Google Scholar]
- 11.Dewaele J, Zachee B, De Vleeschauwer P, Fabry G. Treatment of idiopathic clubfoot: critical evaluation of different types of treatment programs. J Pediatr Ortho. 1994;3:89–95. [Google Scholar]
- 12.Dimeglio A, Bonnet F, Mazeau PH, De Rosa V. Orthopaedic treatment and passive motion machine: consequences for the surgical treatment of clubfoot. J Pediatr Ortho. 1996;5B:173–180. doi: 10.1097/01202412-199605030-00007. [DOI] [PubMed] [Google Scholar]
- 13.Eysenbach G, Jadad AR. Evidence-based patient choice and consumer health informatics in the Internet age. J Med Internet Res. 2001;3:E19. doi: 10.2196/jmir.3.2.e19. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Grayev AM, Boal DK, Wallach DM, Segal LS. Metaphyseal fractures mimicking abuse during treatment for clubfoot. Pediatr Radiol. 2001;31:559–563. doi: 10.1007/s002470100497. [DOI] [PubMed] [Google Scholar]
- 15.Green ADL, Lloyd-Roberts GC. The results of early posterior release in resistant clubfeet. A long-term review. J Bone Joint Surg. (Br) 1985;67:588. doi: 10.1302/0301-620X.67B4.4030856. [DOI] [PubMed] [Google Scholar]
- 16.Greenes RA. eCare and eHealth: The Internet meets health care. J Med Pract manage. 2001;17:106–108. [PubMed] [Google Scholar]
- 17.Han HR, Belcher AE. Computer-mediated support group among parents of children with cancer: an exploratory study. Comput Nurs. 2001;19:27–33. [PubMed] [Google Scholar]
- 18.Horrigan JB, Rainie L. Counting on the Internet. Pew Internet and American Life Project http://www.pewinternet.org. 2002. Dec 29,
- 19.Kite JH. Nonoperative treatment of congenital clubfoot. Clin Orthop. 1972;84:29–38. doi: 10.1097/00003086-197205000-00007. [DOI] [PubMed] [Google Scholar]
- 20.Krauspe R, Vispo Seara JL, Lohr JF. Long-term results after surgery for congenital clubfoot. Foot and Ankle Surgery. 1996;2:77–82. [Google Scholar]
- 21.Ponseti IV, Smoley EN. Congenital Clubfoot: the results of treatment. J Bone Joint Surg. (Am) 1963;45:261–275. [Google Scholar]
- 22.Ponseti IV. Congenital Clubfoot: Fundamentals of Treatment. Oxford, England: Oxford University Press; 1996. [Google Scholar]
- 23.Simons GW. Complete subtalar release in clubfeet. I: A preliminary report. J Bone Joint Surg. (Am) 1985;67:1044–1055. [PubMed] [Google Scholar]
- 24.Sobel E, Giorgini RJ, Michel R, Cohen SL. The natural history and longitudinal study of the surgically corrected clubfoot. J Foot Ankle Surg. 2000;5:305–320. doi: 10.1016/s1067-2516(00)80047-2. [DOI] [PubMed] [Google Scholar]
- 25.Tarraf YN, Carroll NC. Analysis of the components of residual deformity in clubfeet presenting for reoperation. J Pediatr Orthop. 1992;20:233–239. doi: 10.1097/01241398-199203000-00011. [DOI] [PubMed] [Google Scholar]
- 26.Turco VJ. Resistant congenital clubfoot: One-stage posteromedial release with internal fixation: A followup report of a fifteen-year experience. J Bone Joint Surg. (Am) 1979;61:805–814. [PubMed] [Google Scholar]
- 27.Uglow MG, Clarke NM. Relapse in staged surgery for congenital talipes equinovarus. J Bone Joint Surg. (Br) 2000;82:739–743. doi: 10.1302/0301-620x.82b5.9413. [DOI] [PubMed] [Google Scholar]
- 28.Vizkelety T, Szepesi K. Reoperation in Treatment of clubfoot. J Pediatr Orthop. 1989;9:144–147. [PubMed] [Google Scholar]