

Abstract
Study Design.
In vivo biomechanical design using stadiometry and MRI to measure the height change due to (hyper)extension.
Summary of Background Data.
Spine height is decreased under loads such as lifting, whole body vibration and sitting. Extension including increased lumbar lordosis reduces the load on the spine.
Methods.
The aim was to assess the effects of a supine hyperextended posture as a means of restoring the intervertebral disc height after loading and allowing rehydration of the discs. Ten healthy male subjects were tested. A hyperextension intervention was achieved by the means of an inflatable cushion placed under the lumbar spine. The spine height was measured using a stadiometer and MRI was used to assess disc height changes.
Results.
The spine height gain after 10 minutes of a supine hyperextended posture differed significantly between individuals but everybody gained height. MRI images of the lumbar spine were used to measure the disc height. All but one subjects gained height during the hyperextension. Images of the spine during hyperextended posture showed increased lumbar curve and an increased anterior height of each disc compared with the dimensions of the disc with the spine in neutral posture.
Conclusions.
All subjects lost height during sitting. Both methods demonstrated a recovery of height due to hyperextension. Hyperextension could be considered as a prophylaxis against the height loss in occupational loading.
INTRODUCTION
There is a normal diurnal change in spine height. This change is increased under occupational exposures such as lifting, whole body vibration and sitting. In sitting, the normal lumbar lordosis flattens and the intradiscal pressure increases. The beneficial effects of extension (increase of lumbar lordosis) were demonstrated by Williams et al.10, which showed that a lordotic posture results in less back pain than a kyphotic one. It has been shown that a sitting posture causes the spine to lose height3. The height changes are due to both compression and creep of the intervertebral disc and the postural change.
A popular method for seated height measurements is a stadiometer described by Magnusson et al.3. The stadiometer is a device for assessing overall spinal height change while controlling the posture (Figure 1). Height changes are measured using a linear variable transformer (LVDT) with a plunger directly over the top of the head. The technique has been used in a number of studies to evaluate the effects of seat back inclination on spine height changes5, whole body vibration4, back supports9, and passive and active extension interventions6–8. It is believed that the amount of height loss/gain is proportional to increasing or decreasing compressive loads on the spine. Magnusson and Pope6 showed that passive hyperextension for 20 minutes resulted in a significantly increased height recovery compared to a prone flat posture. It is believed that, during hyperextension the facet joints act like a fulcrum, in such a way that they allow more fluid to return into the intervertebral disc, resulting in a height increase4. They tested the hypothesis that stretching hyperextension effort shifts the load pathways in the lumbar spine; however the recovery in height is temporary8. During hyperextension, the facet joints support a certain amount of load that is normally applied to the intervertebral disc. Moreover, the hydration of the disc increases (temporarily) and this results in an improvement of disc nutrition. Another study showed that the optimal time and angle combination was 20° for 20 minutes, as it resulted in the largest recovery and also remained for a relatively long period of time7. This method can be useful in therapy and in primary and secondary prevention of low back pain.
Figure 1. Modified Stadiometer for sitting measurements (from Magnusson et al. 1990).

MATERIALS AND METHODS
For measuring the effects of 10 minutes hyperextension after 5 minutes loading in a seated position, two different methods were used, stadiometry and MRI.
STADIOMETRY
A stadiometer modified for seated postures was used (Figure 1). The subject was positioned in the stadiometer, the supports for head and pelvis were adjusted and four rods to control posture were adjusted to the subject's spinal curve. The subjects were asked to focus their eyes on a spot straight ahead, in order to keep the head still. A linear variable differential transformer (LVDT) with a plunger was lowered on to the top of the subject's head. The sample frequency was 1 Hz. The adjustable rods were placed at four different regions of the spine: a) the mid lumbar region (~L3), b) the mid to lower thoracic region (~T8), c) the upper thoracic region (~T4) and d) the mid cervical region (C4). The seat pan was fixed, while the footrest was adjustable up-down and forwards-backwards, in order to achieve 90°, 75° and 75° angles, for the hip, knee and ankle joints respectively. The LVDT was connected to an analogue oscilloscope and was calibrated by 5mm thick flat metal plates.
All the subjects were males between 23 and 30 years old (mean: 26.3, Sd: 2.26), with no history of any musculoskeletal disorder. Their height ranged from 1.67 - 1.97 m (mean: 1.8 m, Sd : 0.077 m), their weight from 65 - 101 Kg (mean: 80.5 Kg, Sd: 12.349 Kg). Prior to the measurements, each subject underwent a training session of repositioning in the stadiometer, in order to achieve a variation less than 1 mm due to posture differences.
All measurements were made between 9:00 to 13:00. The subject lay for 10 minutes in a supine position with the spine in a neutral angle, to normalise hydration from any pre-loading. Thereafter, the subject was positioned in the stadiometer and was loaded with 4.5 Kg on each shoulder for 5 minutes. After removing the loads, a curve of the length changes of the LVDT over time was obtained for 5 minutes, which was followed by a 10 minutes intervention, where the subject adopted a supine hyperextended posture, achieved by means of an inflatable lumbar support. Finally, the subject was placed again in the stadiometer and another curve of the length changes of the LVDT over time was obtained for 5 minutes. For each set of measurements (prior and post hyperextension) the oscilloscope readings were recorded every 20 seconds.
The lumbar support (Figure 2) used to achieve hyperextension was a plastic, inflatable, ellipsoidal cushion with dimensions of 34 cm x 11 cm when deflated. The air pressure of the cushion was 180 mm of H2O ± 10%, depending on parameters such as the height, weight and flexibility of each subject, but also on the tolerance of the subjects to this slightly uncomfortable posture. The natural curvature of the lumbar spine provided the means for positioning the cushion always at the same point for each subject i.e. right under the peak curve. Thus, a fairly good repeatability of the procedure was achieved as well as the attainment of a symmetrical hyperextended posture.
Figure 2. Inflatable cushion used to increase the lumbar curve.

MAGNETIC RESONANCE IMAGING
The procedure for the MRI scans was kept as close as possible to the procedure that was followed for the stadiometry measurements. The subjects who were scanned were the same ones that underwent the stadiometry procedure and all the scans were taken between 9:00 and 13:00. First, the subject lay supine for 10 minutes with the spine in a neutral angle and then sat on a chair for 5 minutes with loads of 4.5 kg on each shoulder. Thereafter, the subject lay in a supine neutral position inside the magnet and a scan was performed, which lasted for 4 minutes. The inflatable cushion was thereafter placed under the lumbar spine, so a hyperextended posture was adopted. This lasted for 10 minutes, after which another image was obtained, starting from the 6th minute of hyperextension and finishing at the 10th minute. For each subject, the air pressure inside the cushion was exactly the same as the one used in the stadiometry. Finally, the cushion was removed and another 4 minutes scan was taken with the spine in a neutral position.
The magnet, which was used was a 0.2 Tesla "C-shaped" open magnet (Siemens Magnetom Open Viva). As we were interested in measuring the difference in height of the intervertebral discs, took sagittal images of the lumbar spine were taken using a standard pulse sequence for this purpose, called Turbo Spin Echo. The parameters that were used were the following:
| Echos | TR (repetition time) | TE (echo time) | Scan time | Field of view | Slices | Acquisitions |
|---|---|---|---|---|---|---|
| 15 | 3900msec | 134msec | 3min16sec | 175mmx350 mm | 9(6 mm) | 3 |
RESULTS
Stadiometry
Typical results of one subject using the stadiometer are presented in Figure 3. The average over all subjects is presented in Table 1.
Figure 3. Subject No3.
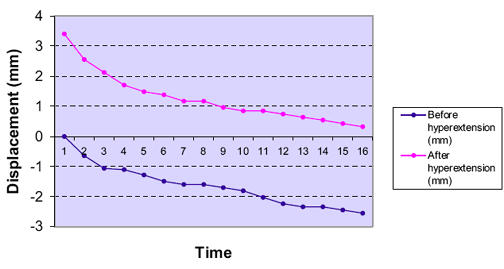
Stadiometer results for one subject
TABLE 1. Average height changes pre- and posthyperextension.
| Sec | Prehyperextension | Posthyperextension |
|---|---|---|
| 0 | 0 | +5.234 (1798)mm |
| 20 | -1.226 (0.831) mm | -1.873 (1.194) mm |
| 40 | -1.883 (1.172) mm | -2.617 (1.729) mm |
| 60 | -2.272 (1.260) mm | -3.277 (2.208) mm |
| 80 | -2.549 (1.298) mm | -3.774 (2.715) mm |
| 100 | -2.905 (1.407) mm | -4.130 (2.890) mm |
| 120 | -3.206 (1.515) mm | -4.466 (3.050) mm |
| 140 | -3.370 (1.516) mm | -4.781 (3.220) mm |
| 160 | -3.681 (1.792) mm | -5.066 (3.258) mm |
| 180 | -3.868 (1.894) mm | -5.253 (3.359) mm |
| 200 | -4.141 (1.917) mm | -5.479 (3.455) mm |
| 220 | -4.275 (1.982) mm | -5.636 (3.493) mm |
| 240 | -4.440 (1.986) mm | -5.866 (3.551) mm |
| 260 | -4.562 (2.010) mm | -6.023 (3.613) mm |
| 280 | -4.838 (2.165) mm | -6.198 (3.665) mm |
| 300 | -5.030 (2.266)mm | -6.374 ( 3.766) mm |
Readings of the oscilloscope were taken every 20 seconds. The table shows the readings whilst seated, pre- and post hyperextension. The figures represent the height lost by the subjects for each point of time, with the Sd given within parentheses. The average amount of height gain after 10 minutes in the supine hyperextended posture (5.234 mm ± 1.798 mm) was almost the same as the height lost (5.030 mm ± 2.266 mm) during the seated posture before hyperextension. The starting point is different from the first measurements as it is the point that is defined as the difference between the mean height gained during hyperextension (5.234 mm) and the mean height lost during sitting before hyperextension (5.030 mm), that is 0.204 mm higher than the original point. It is worth mentioning that the mean amount of height lost after hyperextension was about 1 mm greater than the height gained during hyperextension; however the standard deviation was as large as ~ 2 mm. As for individual subjects, eight of them lost more than gained height during hyperextension. Although there are differences between subjects, all graphs follow a similar pattern. Of most interest was the amount of height gain after 10 minutes of a supine hyperextended posture. Whilst it differed significantly between individuals, everybody gained height, as shown in Figure 4. The values varied from 2.766 mm to 7.660 mm with a mean of 5.234mm (Sd 1.798 mm).
Figure 4. Height Gain.
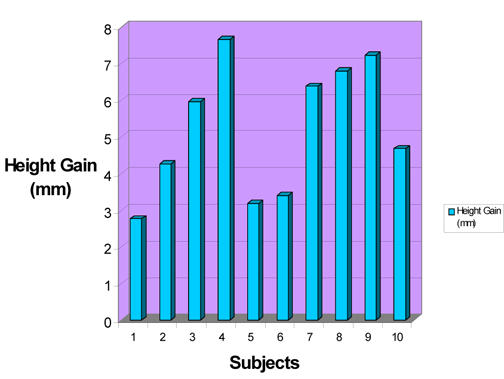
Height gain for each subject after 10 minutes in a supine hyperextended posture
The amount of height lost pre and post hyperextension was also compared. Before hyperextension, the subjects lost height from 2.340 mm up to 8.936 mm with a mean value of 5.030 mm and a standard deviation of 2.266 mm. After hyperextension, the amount of height loss varied from 2.872 mm up to 15.319 mm, with a mean value of 6.374 mm and a standard deviation of 3.766 mm. With the exception of one subject, all subjects lost more height after the hyperextension intervention than before it.
One other parameter derived from the measurements was the percentage of height loss per minute. The largest amount of height loss occurred during the first minute both in pre- and posthyperextension (Table 2 and Figures 5A and B).
TABLE 2. Percentage of height loss per minute.
| Minutes | 1 | 2 | 3 | 4 | 5 |
|---|---|---|---|---|---|
| Pre-Hyperextension | 45.169 % | 18.569 % | 13.161 % | 11.371 % | 11.730 % |
| Post-Hyperextension | 51.412 % | 18.654 % | 12.347 % | 9.617 % | 7.970 % |
MAGNETIC RESONANCE IMAGING
Three images of the lumbar area of the spine were taken. The first and the third image were taken with the spine in a neutral angle (Figure 6A), before and after the 10 minutes intervention of hyperextended posture (Figure 6B).
The most interesting parameter was the difference in height after hyperextension. However, it was not possible to image the whole spine, because of the limited field of view. In addition, it was not practical to measure the possible height gain in separate intervertebral discs, because the height difference was expected to be a fraction of a mm, thus it would be impossible to have adequate accuracy in our measurements. Thus, we elected to measure the length of the part of the spine that was clear in the images for all the volunteers. This included seven intervertebral discs: S1/ Lf5 to T12/11. However, these are the thickest discs in the spine. The measurements were made using the available software of the magnet. The measurements were repeated three times for each subject and the estimated error was less than 0.5 mm. The collected data are displayed in Table 3.
TABLE 3. Spine (part of it) length pre- and posthyperextension.
| Subjects | Spine length pre- hyperextension (mm) | Spine length post- hyperextension (mm) | Difference(mm) |
|---|---|---|---|
| 1 | 212 | 214 | + 2 |
| 2 | 208 | 206 | - 2 |
| 3 | 228 | 231 | + 3 |
| 4 | 216 | 220 | + 4 |
| 5 | 217 | 220 | + 3 |
| 6 | 233 | 236 | + 3 |
| 7 | 206 | 208 | + 2 |
| 8 | 200 | 202 | + 2 |
| 9 | 234 | 236 | + 2 |
| 10 | 245 | 247 | + 2 |
Nine of the ten subjects gained height during the 10 minutes of hyperextension. Half of them gained 2 mm, three others gained 3 mm, one gained 4 mm while one lost 2 mm. The mean gain in height was 2.1 mm, while the standard deviation (mostly due to the subject who lost height) was 1.57 mm. The results are schematically displayed in Figure 7
Figure 7. Length differences of a part of the spine before and after hyperextension (mm).
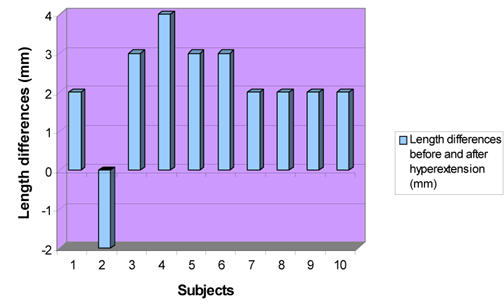
Height (length) gain and loss of the lumbar spine before and after hyperextension.
Images of the spine when the volunteers adopted a hyperextended posture for 10 minutes were taken. It was obvious that the lumbar curvature had increased. Moreover, the anterior height of each disc increased while the posterior height had decreased, when compared with the dimensions of the disc with the spine in neutral angle before the hyperextension intervention. The mean anterior height increased from 1.13 to 1.27cm (p<0.005) and the posterior height decreased from 0.777 to 0.725 (p<0.005). The dimensions for the intervertebral disc space between each lumbar vertebra are presented in Table 4.
TABLE 4. Comparison between the anterior and posterior height (in cm) of the lumbar intervertebral discs pre- and posthyperextension.
| Subjects | L1/L2
|
L2/L3
|
L3/L4
|
L4/L5
|
||||
|---|---|---|---|---|---|---|---|---|
| Ant | Post | Ant | Post | Ant | Post | Ant | Post | |
| 1 - Pre | 1.0 | 0.7 | 1.1 | 0.9 | 1.4 | 1.0 | 1.6 | .07 |
| 1 - Post | 1.1 | 0.7 | 1.2 | 0.9 | 1.6 | 0.9 | 1.7 | 0.6 |
| 2 - Pre | 0.8 | 0.7 | 0.9 | 0.6 | 1.2 | 0.9 | 1.2 | 0.8 |
| 2 - Post | 0.9 | 0.6 | 1.1 | 0.6 | 1.2 | 0.8 | 1.3 | 0.8 |
| 3 - Pre | 1.2 | 0.8 | 1.2 | 0.9 | 1.3 | 0.9 | 1.5 | 1.0 |
| 3 - Post | 1.3 | 0.7 | 1.3 | 0.8 | 1.5 | 0.9 | 1.7 | 0.9 |
| 4 - Pre | 0.8 | 0.6 | 1.0 | 0.7 | 1.1 | 0.8 | 1.5 | 0.8 |
| 4 - Post | 0.9 | 0.6 | 1.1 | 0.7 | 1.3 | 0.7 | 1.6 | 0.8 |
| 5 - Pre | 1.1 | 0.7 | 1.1 | 0.7 | 1.3 | 0.9 | 1.5 | 0.9 |
| 5 - Post | 1.2 | 0.6 | 1.3 | 0.7 | 1.4 | 0.8 | 1.6 | 0.8 |
| 6 - Pre | 0.9 | 0.6 | 1.0 | 0.8 | 1.2 | 0.9 | 1.5 | 0.8 |
| 6 - Post | 1.2 | 0.5 | 1.3 | 0.7 | 1.4 | 0.7 | 1.6 | 0.8 |
| 7 - Pre | 0.8 | 0.6 | 1.0 | 0.8 | 1.2 | 0.8 | 1.3 | 0.7 |
| 7 - Post | 0.9 | 0.5 | 1.1 | 0.7 | 1.2 | 0.8 | 1.5 | 0.6 |
| 8 - Pre | 0.6 | 0.6 | 0.8 | 0.7 | 1.1 | 0.7 | 1.2 | 1.0 |
| 8 - Post | 0.7 | 0.7 | 1.0 | 0.7 | 1.1 | 0.7 | 1.2 | 0.9 |
| 9 - Pre | 0.7 | 0.5 | 1.0 | 0.7 | 1.2 | 0.8 | 1.5 | 0.9 |
| 9 - Post | 1.0 | 0.4 | 1.1 | 0.7 | 1.3 | 0.7 | 1.6 | 0.9 |
| 10 - Pre | 1.0 | 0.7 | 1.1 | 0.8 | 1.3 | 0.8 | 1.1 | 0.9 |
| 10 - Post | 1.3 | 0.7 | 1.3 | 0.7 | 1.5 | 0.8 | 1.3 | 0.9 |
DISCUSSION
The curve obtained using the stadiometer, which describes the average height loss pre and post hyperextension is an overall indication of the behaviour of the spine, under the conditions described in this study. It is worth mentioning that the standard deviation is very high; in some cases it is almost 70% of the mean value. However, this is something that was expected, since the only common characteristics of our volunteers were their age (23-30 years old) and their gender (male). There were remarkable differences in height (up to 30 cm), in weight (up to 37 Kg), in stamina and even differences in their character, which made some of the subjects less focused to the procedure or less tolerant to the requirements (i.e. sitting completely still for 5 minutes). Moreover, although none of the subjects had a history of back problems, the MRI scans revealed some pathological conditions (e.g. Subject No 9 is scoliotic, Subject No 10 has two degenerated "black" intervertebral discs) that may have affected the results.
Nevertheless, the graphs for individual subjects followed a similar pattern. All subjects lost height during sitting, as it was expected, since when a person is sitting the lumbar lordosis tends to flatten, so the intradiscal pressure rises, resulting to fluid transport out of the intervertebral disc.4, 10. The measurements also showed that most of the height is lost during the first minute. This verifies previous research3 and it is believed that this occurs due to the osmotic swelling pressure within the disc, which tends to resist the hydrostatic pressure derived from compressive loads and prevents the disc of becoming completely dehydrated1,2.
After the 10 minute hyperextension intervention, all the subjects gained height. However, it cannot be argued that the height recovery for any person going through the same procedure will be of this magnitude. An unknown, and practically impossible to measure, amount of height loss took place during the interval in which the subject got up from the bed and positioned himself in the stadiometer. In addition, although each volunteer underwent a training session of positioning in exactly the same posture in the stadiometer (with no more than 1 mm variability), it cannot be certain that the desired accuracy was obtained when the subjects were tired and un-concentrated at the end of the 30 minutes procedure.
It is clear that hyperextension causes height gain, as has been shown in previous research6–8. In addition, we were able to verify this by using MRI. It was clear that during hyperextension the Functional Spine Units were more "open" anteriorly than in a neutral posture (Figure 7, Table 4). Even in the neutral position, the anterior part of the FSUs were more "open" than the posterior parts; this is probably one reason for recovering height when resting on a bed. The anterior height of four intervertebral discs, during hyperextension, was even 40% greater than normal in some cases, while the posterior height decreased up to 20%. Consequently, more fluid is allowed to be imbibed into the disc and at a faster rate when compared to "flat" supine posture.7
In the MRI scans, due to the limited field of view, only a part of the spine was possible to image. However, this included the whole lumbar part, which was most important since the purpose of the cushion was to increase the lumbar lordosis of the spine. The comparison of the length of this part of the spine pre and post hyperextension (Table 3) showed that the individuals gained and also maintained height, since lying on a bed is not a loading condition for the intervertebral discs. The reduction in height after hyperextension in one subject could possibly be caused by small muscle contractions or that the subject rolled slightly over his glutei, by compressing his spine (the subject was rather obese).
Another indication of the rehydration of the disc due to hyperextension is the fact that nine out of ten volunteers lost more height when sitting in the stadiometer after being hyperextended than before. Also, the percentage of height that was lost during the first minute was greater after hyperextension (51.412% of the total amount) than before (45.169%), as we can derive from Table 2 and Figures 5 and 6. One of the properties of a well hydrated intervertebral disc is its relatively low osmotic swelling pressure, which retains fluid in the disc., Therefore, under a compressing condition (e.g. sitting), more fluid is "available" to flow out of the disc and it can be argued that it will occur faster than in a less hydrated disc. In this study, there was one subject who had opposite results than the others, i.e. he lost more height before hyperextension. However, this subject (as it was shown in the MRI scans) had scoliosis, which possibly could have affected the distribution of the loads on his spine. Another reason could be that he tried to remain still in the stadiometer by pressuring his hands on his lap rather than having them relaxed.
Figure 5. Percentage of average height loss per minute before (A) and after (B) hyperextension.
Figure 5A. Percentage of average height loss per minute (before hyperextension).
Figure 5B. Percentage of average height loss per minute (after hyperextension).
Figure 6. Image of the lumbar spine in a neutral angle (A), and in the hyperextended posture (B).
Figure 6A.

Figure 6B.

Comparing the two methods (stadiometry and Magnetic Resonance Imaging), although following similar procedures, it cannot be argued that there is a direct correlation between results. One important reason for this is that the measurements with the stadiometer were taken while the subjects were sitting, while in MRI the subjects were lying. Therefore, the already compressed spine from the weight bearing (4.5 Kg on each shoulder for 5 minutes), became even more compressed before the hyperextension intervention in stadiometry. On the contrary, in order to obtain the MRI images, after the weight bearing period, the subjects had to lie, which started to unload the spine, so the effects of hyperextension could not be the same, since the measurements started from different conditions of the intervertebral discs.
Another difference is that using the stadiometer, the height changes of the whole spine (including the head, the neck and the glutei) were measured. With the MRI only 7 intervertebral discs, although the whole lumbar spine, were imaged. The advantage of the stadiometer was that data were recorded every 20 seconds.
For the MRI measurements a "fast" sequence (Turbo Spin Echo) was used, which is the standard for imaging the spine. The advantage of this sequence, as it is for every "fast" sequence, is that it produces images of adequate quality in a relatively short time (in this case about 4 minutes including tuning of the machine and adjustment of the field of view). However, the image was not obtained in "real time", but it was the average of 3 acquisitions, which required 3 minutes and 16 seconds (net scan time). The huge advantage of this technique is that it provides images of the actual intervertebral discs, consequently allowing us to measure height differences caused only by fluid flow inwards and outwards of the discs, excluding any other parameter, which may induce height changes (in the case of the stadiometer, fatigue and inability to maintain a still posture).
References
- 1.Adams MA, McNally DS, Dolan P. Stress distribution inside intervertebral discs: The effects of age and degeneration. J Bone and Joint Surg (Br) 1996;78:965–972. doi: 10.1302/0301-620x78b6.1287. [DOI] [PubMed] [Google Scholar]
- 2.Botsford DJ, Esses SI, Ogilvie-Harris DJ. In vivo diurnal variation in intervertebral disc volume and morphology. Spine. 1994;19(8):935–940. doi: 10.1097/00007632-199404150-00012. [DOI] [PubMed] [Google Scholar]
- 3.Magnusson ML, Hult E, Lindström I, Lindell V, Pope MH, Hansson T. Measurement of time-dependent height-loss during sitting. Clin Biomechanics. 1990;5:137–142. doi: 10.1016/0268-0033(90)90016-Y. [DOI] [PubMed] [Google Scholar]
- 4.Magnusson ML, Almqvist M, Broman H, Pope M, Hansson T. Measurement of height loss during whole body vibrations. J Spinal Disorders. 1992;5(2):198–203. doi: 10.1097/00002517-199206000-00009. [DOI] [PubMed] [Google Scholar]
- 5.Magnusson M, Hansson T, Pope MH. The effect of seat back inclination on spine height changes. Applied Ergonomics. 1994;25(5):294–298. doi: 10.1016/0003-6870(94)90043-4. [DOI] [PubMed] [Google Scholar]
- 6.Magnusson ML, Pope MH, Hansson T. Does hyperextension have an unloading effect on the intervertebral disc? Scand J Rehab Med. 1995;27:5–9. [PubMed] [Google Scholar]
- 7.Magnusson ML, Aleksiev AR, Spratt KF, Lakes RS, Pope MH. Hyperextension and spine height changes. Spine. 1996;21(22):2670–2675. doi: 10.1097/00007632-199611150-00017. [DOI] [PubMed] [Google Scholar]
- 8.Magnusson ML, Pope ML. Body height changes with hyperextension. Clin Biomechanics. 1996;11(4):236–238. doi: 10.1016/0268-0033(95)00066-6. [DOI] [PubMed] [Google Scholar]
- 9.Magnusson M, Pope MH, Hansson T. Does a back support have a positive biomechanical effect? Applied Ergonomics. 1996;27(3):201–205. doi: 10.1016/0003-6870(95)00007-0. [DOI] [PubMed] [Google Scholar]
- 10.Williams MM, Hawley JA, McKenzie RA, Van Wijmen PM. A comparison of the effects of two sitting postures on back and referred pain. Spine. 1991;16(10):1185–1191. doi: 10.1097/00007632-199110000-00010. [DOI] [PubMed] [Google Scholar]