

Abstract
Objective—To assess changes in size of the central pulmonary arteries following a total cavopulmonary connection (TCPC). Design—A retrospective analysis of the angiographic diameters of the central pulmonary arteries, expressed as z scores, in infancy before the TCPC and 3.5 (0.9) years (mean (SD)) later. Analysis of the relation between the pulmonary arteriolar resistance and the z scores at follow up. Setting—Tertiary referral centre. Patients—32 patients who had TCPC from February 1990 to July 1993. Results—The patients were divided into two groups (n = 16) depending on their preoperative flow ratio: group I, Qp/Qs ⩽ 1; group II, Qp/Qs > 1. At the initial study in infancy the mean z scores in group I were −6.0 for the right pulmonary artery (RPA) and −9.6 for the left pulmonary artery (LPA); in group II the respective values were −2.7 and −3.0. Before the TCPC the values increased to 0.5 (RPA) and −0.5 (LPA) in group I, and to 8.8 (RPA) and 8.2 (LPA) in group II. At follow up the z scores decreased to −2.4 (RPA) and −4.9 (LPA) in group I, and to 2.2 (RPA) and −0.7 (LPA) in group II. The changes in pulmonary artery diameters were significant for both groups (p < 0.02). Following the TCPC, no significant difference in pulmonary arteriolar resistance index was found between patients with relatively small pulmonary arteries (z score RPA+LPA ⩽ 0) and those with relatively large pulmonary arteries (z score RPA+LPA > 0). Conclusions—Creation of a TCPC results in a significant reduction in size of the central pulmonary arteries. At a mean interval of 3.5 years following the TCPC, however, there was no significant difference in pulmonary arteriolar resistance index between patients with smaller and larger central pulmonary arteries. Keywords: total cavopulmonary connection; congenital heart disease; pulmonary artery size; pulmonary arteriolar resistance
Full Text
The Full Text of this article is available as a PDF (149.2 KB).
Figure 1 .
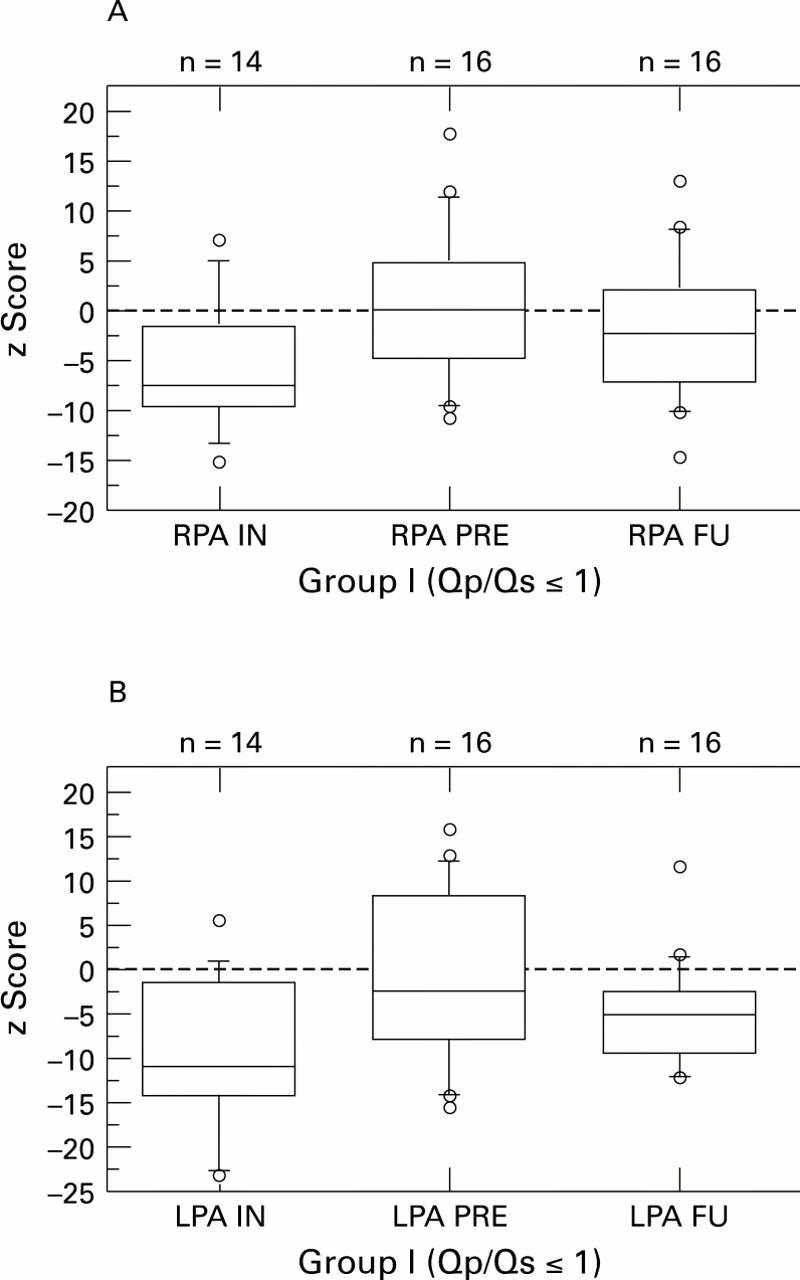
Diameters (given as z scores) of the central right (RPA) and central left pulmonary artery (LPA) at the initial cardiac catheterisation (IN), before total cavopulmonary connection (TCPC) (PRE), and at the follow up study 3.5 years after TCPC (FU) in patients of group I. For both pulmonary arteries the changes in the diameters between the three points were significant (p < 0.02), and the difference between IN and FU was also significant (p < 0.05).
Figure 2 .
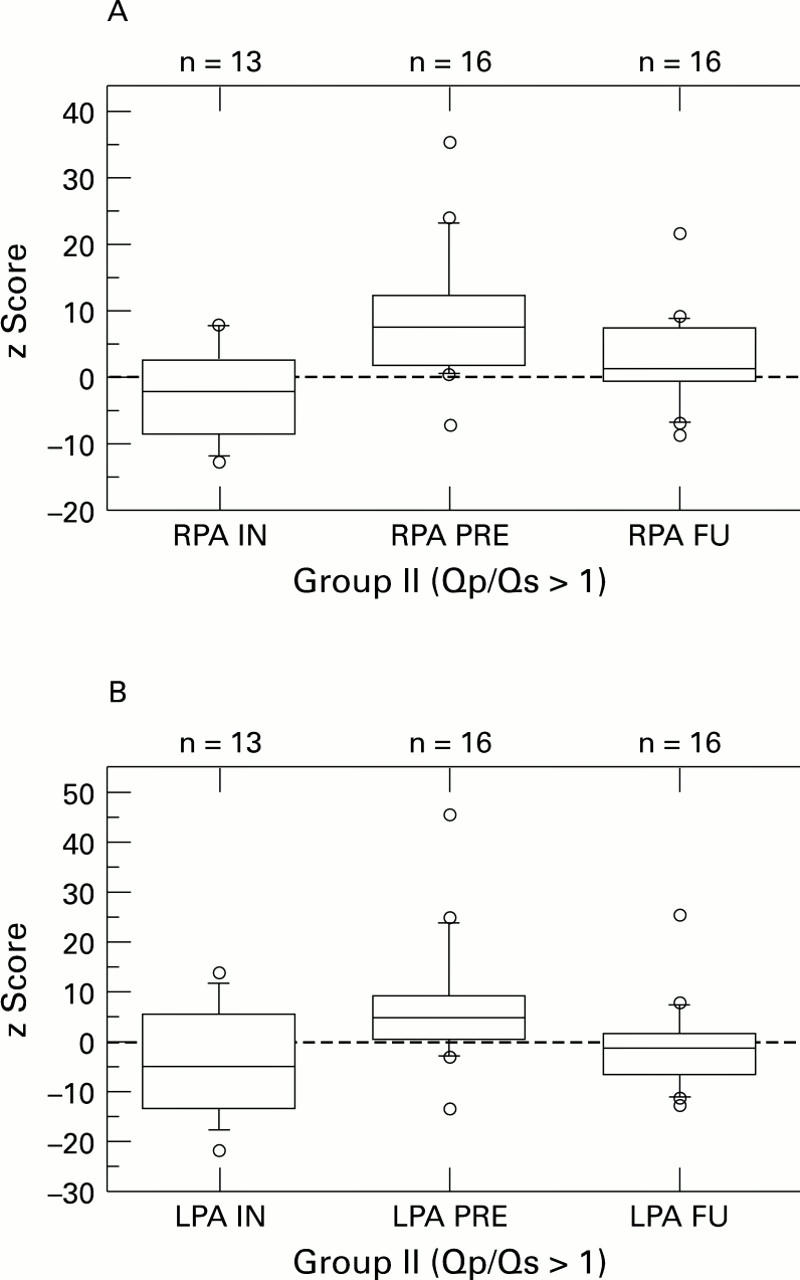
Diameters (given as z scores) of the central right (RPA) and central left pulmonary artery (LPA) at the initial cardiac catheterisation (IN), before total cavopulmonary connection (TCPC) (PRE), and at the follow up study 3.5 years after TCPC (FU) in patients of group II. For both pulmonary arteries the changes in the diameters between the three points were significant (p < 0.02); the difference between IN and FU was significant only for the right pulmonary artery (p < 0.03).
Figure 3 .

Diagram showing the pulmonary arteriolar resistance index (PARI) at the time of follow up in relation to pulmonary artery (PA) diameters (expressed as z score right PA + z score left PA). There was no significant difference between patients with larger pulmonary arteries (z score right PA + z score left PA > 0) and smaller pulmonary arteries (z score right PA + z score left PA < 0).
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Cecchin F., Johnsrude C. L., Perry J. C., Friedman R. A. Effect of age and surgical technique on symptomatic arrhythmias after the Fontan procedure. Am J Cardiol. 1995 Aug 15;76(5):386–391. doi: 10.1016/s0002-9149(99)80106-4. [DOI] [PubMed] [Google Scholar]
- Gewillig M., Wyse R. K., de Leval M. R., Deanfield J. E. Early and late arrhythmias after the Fontan operation: predisposing factors and clinical consequences. Br Heart J. 1992 Jan;67(1):72–79. doi: 10.1136/hrt.67.1.72. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hofbeck M., Singer H., Scharf J., Rupprecht T., Ries M., Buheitel G., Blum U., Mahmoud O., Emde J. V. Die totale kavopulmonale Anastomose: Risikofaktoren und Ergebnisse bei Patienten unter 4 Jahren. Z Kardiol. 1994 Sep;83(9):615–622. [PubMed] [Google Scholar]
- Lenfant C. NHLBI funding policies. Enhancing stability, predictability, and cost control. Circulation. 1994 Jul;90(1):1–1. doi: 10.1161/01.cir.90.1.1. [DOI] [PubMed] [Google Scholar]
- Lenfant C. NHLBI funding policies. Enhancing stability, predictability, and cost control. Circulation. 1994 Jul;90(1):1–1. doi: 10.1161/01.cir.90.1.1. [DOI] [PubMed] [Google Scholar]
- Mendelsohn A. M., Bove E. L., Lupinetti F. M., Crowley D. C., Lloyd T. R., Beekman R. H., 3rd Central pulmonary artery growth patterns after the bidirectional Glenn procedure. J Thorac Cardiovasc Surg. 1994 May;107(5):1284–1290. [PubMed] [Google Scholar]
- Rammos S., Kramer H. H., Trampisch H. J., Krogmann O. N., Kozlik R., Bourgeois M. Normalwerte des Wachstums der Pulmonalarterien im Kindesalter. Eine angiographische Studie. Herz. 1989 Dec;14(6):348–357. [PubMed] [Google Scholar]
- Redington A. N., Penny D., Shinebourne E. A. Pulmonary blood flow after total cavopulmonary shunt. Br Heart J. 1991 Apr;65(4):213–217. doi: 10.1136/hrt.65.4.213. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Slavik Z., Lamb R. K., Webber S. A., Devlin A. M., Keeton B. R., Monro J. L., Salmon A. P. Bidirectional superior cavopulmonary anastomosis: how young is too young? Heart. 1996 Jan;75(1):78–82. doi: 10.1136/hrt.75.1.78. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Uemura H., Yagihara T., Kawashima Y., Yamamoto F., Nishigaki K., Matsuki O., Okada K., Kamiya T., Anderson R. H. What factors affect ventricular performance after a Fontan-type operation? J Thorac Cardiovasc Surg. 1995 Aug;110(2):405–415. doi: 10.1016/S0022-5223(95)70237-7. [DOI] [PubMed] [Google Scholar]
- Weber H. S., Gleason M. M., Myers J. L., Waldhausen J. A., Cyran S. E., Baylen B. G. The Fontan operation in infants less than 2 years of age. J Am Coll Cardiol. 1992 Mar 15;19(4):828–833. doi: 10.1016/0735-1097(92)90526-s. [DOI] [PubMed] [Google Scholar]
- de Leval M. R., Kilner P., Gewillig M., Bull C. Total cavopulmonary connection: a logical alternative to atriopulmonary connection for complex Fontan operations. Experimental studies and early clinical experience. J Thorac Cardiovasc Surg. 1988 Nov;96(5):682–695. [PubMed] [Google Scholar]