

Abstract
We report the case of a 65-year-old man with a 6-year history of hypertension who presented with dilated cardiomyopathy, a transient cerebrovascular event, paroxysmal sweating, and intractable hypertension. Coronary angiography revealed no abnormality, but diagnostic testing was pursued because of the severe sweating and hypertension. Two-dimensional echocardiography showed 4-chamber dilatation with decreased left ventricular contractility. Further investigation, including a computed tomographic scan of the abdomen, led to a di-agnosis of pheochromocytoma. Surgical resection of a left adrenal pheochromocytoma quickly resolved the patient's hypertension and resulted in substantially improved cardiac function after 4 months.
Although pheochromocytoma has rarely been reported in the presence of both dilated cardiomyopathy and cerebrovascular events, it should be included in the differential diagnosis when patients present with dilated cardiomyopathy and a cerebrovascular event that have no obvious cause.
Key words: Adrenal gland neoplasms/complications/diagnosis/pathology; brain ischemia/etiology; cardiomyopathy, complications/dilated/etiology; catecholamines/physiology; cerebrovascular disorders/complications; diagnosis, differential; heart failure, congestive/diagnosis/etiology/surgery; hypertension/complications; pheochromocytoma/complications/diagnosis/physiopathology; remission, spontaneous; vasculitis; ventricular function, left
Catecholamine-induced cardiomyopathy caused by pheochromocytoma is well-recognized, yet rare. Cerebral ischemia and stroke symptoms can also occur (rarely) in patients who have pheochromocytoma. Dilated cardiomyopathy can predispose patients to mural thrombi and subsequent embolic events. However, excessive catecholamines can cause cerebrovascular events directly. Prompt recognition of pheochromocytoma is crucial in treating patients who present with otherwise-inexplicable dilated cardiomyopathy and a transient cerebrovascular event.
Case Report
In June 2003, a 65-year-old man presented with progressive exertional dyspnea and a 1-week history of orthopnea. The patient had a 6-year history of hypertension. His blood pressure was 213/115 mmHg; his pulse rate was 80 beats/min.
A chest radiograph revealed cardiomegaly and pulmonary congestion (Fig. 1). No ischemia or infarction was seen on a 12-lead electrocardiogram. Two-dimensional echocardiography revealed diffuse left ventricular hypokinesia, 4-chamber dilatation, an estimated left ventricular ejection fraction of 0.35 (modified Simpson's rule), a left ventricular end-diastolic diameter (LVEDD) of 62 mm, and a left ventricular end-systolic diameter (LVESD) of 51 mm. No intracavitary thrombosis was detected on cross-sectional 2-dimensional echocardiography. Results of a stress test with thallium 201 were negative for cardiac ischemia.

Fig. 1 A chest radiograph shows moderate cardiomegaly and pulmonary congestion.
The patient's initial symptoms placed him in New York Heart Association (NYHA) functional class III. Treatment with diuretic and other antihypertensive drugs controlled the symptoms of congestive heart failure. Therefore, he was discharged from the hospital; he was prescribed multiple antihypertensive drugs for the control of labile blood pressure.
Six days later, the patient—appearing anxious, and experiencing dizziness, paroxysmal sweating, hypertension, and left-leg weakness—arrived by ambulance at our emergency department. His heart rate was 100 beats/min, and his blood pressure was 120/70 mmHg. Neurologic examination showed normal right-side but impaired left-side sensation and motor function. A computed tomographic scan of the patient's head revealed very small low-density lesions on both sides of the basal ganglia. A repeat echocardiogram showed no mural thrombus.
The patient's acute-stage cerebrovascular events disappeared after 24 hours. Despite therapy with multiple antihypertensive drugs, the blood pressure varied from 120/70 to 200/110 mmHg over 10 days during his hospitalization. The presence of coronary artery disease was suspected, but cardiac catheterization showed normal coronary arteries. The results of thyroid studies were normal, as were the electrolyte levels, including sodium, potassium, calcium, and phosphate. However, urinary catecholamine studies revealed an elevated vanillylmandelic acid level (total, 83.7 mg/24 hr; normal range, 2–7 mg/24 hr). Computed tomography of the abdomen revealed a heterogeneous, dense mass (8 × 5 × 14 cm) above the left kidney (Fig. 2), consistent with a pheochromocytoma. The patient underwent a left adrenectomy; microscopic examination confirmed that the tumor was a pheochromocytoma.
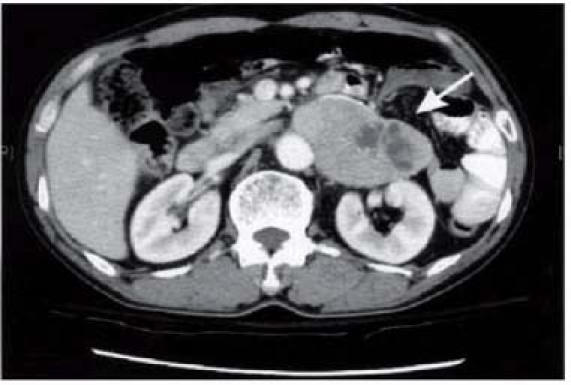
Fig. 2 An enhanced abdominal computed tomographic scan shows a large (8 × 5 × 14-cm) left adrenal mass (arrow) with areas of necrosis and hemorrhagic fluid.
After the excision of the tumor, the patient's systolic blood pressure decreased by 50 to 60 mmHg. Follow-up 2-dimensional echocardiography, performed approximately 4 months later, revealed normal left ventricular dimensions (LVEDD, 48 mm; and LVESD, 30 mm). By that time, his left ventricular ejection fraction had increased to 0.64 (modified Simpson's rule), and his symptoms had improved to the level of NYHA functional class I.
Discussion
Pheochromocytoma, a rare neuroendocrine tumor de-rived from enterochromaffin cells, usually causes paroxysmal or sustained hypertension. Less common car-diovascular manifestations include acute heart failure, myocardial infarction, angina pectoris, arrhythmias, and dilated cardiomyopathy.1
Our patient was an elderly man whose pheochromocytoma induced dilated cardiomyopathy, which presented as a stroke. A review of the English-language medical literature revealed only 1 case—that of an adolescent male—with a similar presentation.5 The most unusual aspect of our reported case was the coexistence of a transient cerebrovascular event with dilated cardiomyopathy.
Dilated cardiomyopathy secondary to pheochromocytoma is rare. The condition is partially or completely reversible in some patients. In the reported cases, resolution occurred between 6 weeks and 16 months.2–4
The chronic secretion of catecholamines can facilitate various forms of myocardial damage. Catecholamine-induced cardiomyopathy probably arises from multiple factors. At the cellular level, increased levels of catecholamines cause a receptor-mediated elevation of intracellular calcium, which results in the supercontraction of sarcomeres and consequent myofibrolysis.6 A release of lysosomal proteases activates lipoperoxidases that can be directly toxic or can cause damage via the release of oxygen free radicals, either of which increases sarcolemma-membrane permeability.7 Hypertrophy and the contraction-band necrosis of myofibers occur, along with a moderate inflammatory reaction. The fibrous replacement of myocardium, which can also occur, may explain the incomplete reversibility of catecholamine-induced cardiomyopathy in certain patients.8
Reversible cerebral ischemia with focal neurologic deficits is a rare manifestation of pheochromocytoma. There are several reasons for the onset of acute ischemic cerebral infarction in patients who have pheochromocytoma.
First, hypertension alone can cause cerebral infarction in patients who have pheochromocytoma.9 During hypertensive crises, the combination of cerebrovascular autoregulation failure and very high blood pressure can cause hypertensive encephalopathy.10 Paroxysmal hypertension, as we observed in our patient, can be followed by extended hypotension because of the systemic exhaustion of catecholamines.
Second, retrospective studies have suggested that patients with dilated cardiomyopathy are at risk of stroke, probably attributable to the embolization of a left ventricular thrombus.11 At autopsy, patients with dilated cardiomyopathy often display pathologic evidence of ventricular thrombi. In a study by Falk and coworkers,11 a left ventricular thrombus was present on initial echocardiography in 44% of cases of dilated cardiomyopathy. The investigators concluded that the highest risk of thrombus formation and systemic embolization occurred in patients who had the lowest fractional shortening of the left ventricle. Compared with the thrombi that develop in cases of acute myocardial infarction, the thrombi in patients with dilated cardiomyopathy tend to be smaller and are not always located in a dyskinetic region of the myocardium. Therefore, such thrombi are often difficult to see on echocardiography.
Third, spasms of the cerebral arteries—induced by sympathomimetic agents—may cause brain lesions. Vascular spasms, which have been reported in the peripheral, coronary, and cerebral arteries of patients who have pheochromocytoma,12 typically cause either transient impairment of circulation or infarction. Razavi and colleagues13 described a patient with both pheochromocytoma and variations in the caliber of central-nervous-system vessels; on serial cerebral angiography, the caliber variations resembled vasculitis. Angiographic changes are likely produced by excessive catecholamine and, accordingly, suggest vasospasm rather than true vasculitis.
Conclusion
Hypertension, congestive heart failure, and cerebrovascular events have been reported as complications of pheochromocytoma. Cerebral ischemia and stroke symptoms also occur occasionally in patients who have pheochromocytoma, sometimes subsequent to the development of a mural thrombus. After the pheochromocytoma has been excised, both the hypertension and the cardiac dysfunction can resolve. The speed with which the cardiomyopathy resolves generally depends on the duration of the condition.
An evaluation for pheochromocytoma is appropriate when patients present with dilated cardiomyopathy and focal cerebral symptoms that have no clear cause, especially in the presence of intermittent hypertension or other paroxysmal symptoms. Although pheochromocytoma is a rare cause of these symptoms, awareness of atypical presentations of this tumor is crucial. Pheochromocytoma should be considered in the differential diagnosis in refractory cases.
Footnotes
Address for reprints: Shih Tai Chang, MD, Division of Cardiology, Chia-yi Chang Gung Memorial Hospital, 6, Sec. West Chai-Pu Road, Pu-TZ City, Chai Yi Hsien 613, Taiwan, ROC. E-mail: cst1234567@yahoo.com.tw
References
- 1.Sardesai SH, Mourant AJ, Sivathandon Y, Farrow R, Gibbons DO. Phaeochromocytoma and catecholamine induced cardiomyopathy presenting as heart failure. Br Heart J 1990; 63:234–7. [DOI] [PMC free article] [PubMed]
- 2.Wood R, Commerford PJ, Rose AG, Tooke A. Reversible catecholamine-induced cardiomyopathy. Am Heart J 1991;121(2 Pt 1):610–3. [DOI] [PubMed]
- 3.Lam JB, Shub C, Sheps SG. Reversible dilatation of hypertrophied left ventricle in pheochromocytoma: serial two-dimensional echocardiographic observations. Am Heart J 1985;109(3 Pt 1):613–5. [DOI] [PubMed]
- 4.Quigg RJ, Om A. Reversal of severe cardiac systolic dysfunction caused by pheochromocytoma in a heart transplant candidate. J Heart Lung Transplant 1994;13:525–32. [PubMed]
- 5.Dagartzikas MI, Sprague K, Carter G, Tobias JD. Cerebrovascular event, dilated cardiomyopathy, and pheochromocytoma. Pediatr Emerg Care 2002;18:33–5. [DOI] [PubMed]
- 6.Pearce RM. Experimental myocarditis; a study of the histological changes following intravenous injections of adrenalin. J Exp Med 1906;8:400–9. [DOI] [PMC free article] [PubMed]
- 7.Boutet M, Huttner I, Rona G. Permeability alteration of sarcolemmal membrane in catecholamine-induced cardiac muscle cell injury. In vivo studies with fine structural diffusion tracer horse radish peroxidase. Lab Invest 1976;34:482–8. [PubMed]
- 8.Bloom S. Catecholamine cardiomyopathy. N Engl J Med 1987;317:900–1. [DOI] [PubMed]
- 9.Lehmann FS, Weiss P, Ritz R, Harder F, Staub JJ. Reversible cerebral ischemia in patients with pheochromocytoma. J Endocrinol Invest 1999;22:212–4. [DOI] [PubMed]
- 10.Goswami R, Tandon N, Singh B, Kochupillai N. Adrenal tumour, congestive heart failure and hemiparesis in an 18-year-old male. A clinical-pathological conference. Int J Cardiol 1995;49:233–8. [DOI] [PubMed]
- 11.Falk RH, Foster E, Coats MH. Ventricular thrombi and thromboembolism in dilated cardiomyopathy: a prospective follow-up study. Am Heart J 1992;123:136–42. [DOI] [PubMed]
- 12.Isner JM, Estes NA 3rd, Thompson PD, Costanzo-Nordin MR, Subramanian R, Miller G, et al. Acute cardiac events temporally related to cocaine abuse. N Engl J Med 1986;315: 1438–43. [DOI] [PubMed]
- 13.Razavi M, Bendixen B, Maley JE, Shoaib M, Zargarian M, Razavi B, Adams HP. CNS pseudovasculitis in a patient with pheochromocytoma. Neurology 1999;52:1088–90. [DOI] [PubMed]