

Abstract
Researchers have demonstrated that certain types of pain coping are correlated with less pain severity and disability and that there are differences between Caucasians and African-American pain patients in their use of specific coping strategies. However, the extent to which racial group differences exist in the associations between pain coping strategies and pain severity, interference, and disability is unclear. Furthermore, the role of education in these associations is uncertain. We recruited a diverse community sample of individuals with chronic pain and their spouses to examine this issue (N = 105). Participants completed the Coping Strategies Questionnaire, Multidimensional Pain Inventory, and Sickness Impact Profile. Results showed that African-American participants reported significantly more pain severity, interference, and disability and reported using diverting attention and prayer and hoping pain-coping strategies significantly more often than Caucasian participants; however, only the racial group difference in prayer and hoping remained when controlling for education. We also examined whether race and education interacted with coping strategies in relating to pain and disability. Significant three-way interactions were found for physical and psychosocial disability, suggesting that educational level should be included in analyses exploring racial group differences. The results suggest the need for pain treatments that take into account the educational and cultural context of pain.
Perspective
This article demonstrates that demographic variables such as race and education should be considered together when evaluating the effectiveness of coping with pain. The findings have the potential to enhance research and clinical practice with diverse groups.
Keywords: Chronic pain, coping strategies, education, race, physical disability, psychosocial disability
Researchers have called attention to racial disparities in pain care and compensation.4-6,12,30,32In addition, there are race differences in clinical and experimental pain with African-Americans reporting more clinical pain, lower pain thresholds for ischemic and cold pressor pain, higher pain-related disability, and higher pain unpleasantness than Caucasians.4,5,8,12,13,33,34,40,41 Other research groups have not found race differences in pain severity.9,21 Although such research may enhance treatment and prevention with diverse groups, it is essential to also examine variables that might moderate racial group differences in the pain experience. For instance, race differences in coping and educational background might explain group differences in pain and disability. The purpose of the current study is to examine race and education as variables that play a significant role in the relationship between coping and pain.
According to Lazarus and Folkman,29 coping is a consequence of individuals’ appraisals of events. The use of particular coping strategies is based on judgments of pain as a threat as well as perceived ability to cope with pain, suggesting that certain types of coping are related to pain ratings. Indeed, greater pain control beliefs and ignoring pain are inversely related with poorer pain outcomes, including pain, distress, and disability, whereas prayer and hoping and diverting attention are positively correlated with these poorer outcomes.9,21,28,43 Pain coping can affect long-term functional disability and pain,1,10 and changes in coping are related to improvements in psychological and physical functioning.20,22-24
Researchers have demonstrated race differences in some pain coping strategies. African-Americans report using prayer and hoping more than Caucasians to cope with pain.7,9,21 African-American pain patients also report lower perceived control over pain, more external pain-coping strategies, and a stronger belief that others should be solicitous when they experience pain.41 In a study of rheumatoid arthritis (RA), African-Americans were more likely to divert attention away from pain whereas Caucasians were more likely to ignore the pain and use coping self-statements.21 However, few published studies have focused on racial group differences in the relationship between pain coping and pain variables. Jordan et al21 found that prayer and hoping was positively correlated with inactivity in African-American but not Caucasian participants. In contrast, reinterpreting pain sensations was positively correlated with pain severity in African-American participants whereas this coping strategy was negatively correlated with pain severity in Caucasian participants.
While identifying race differences in coping, pain, and the correlation between coping and pain has added to our knowledge of disparities in pain, it is also important to consider other demographic characteristics that might account for or interact with racial group differences. In doing so, researchers may avoid the danger of overinter-preting racial group differences.16,31 Educational attainment is one such demographic factor, especially because many pain-coping strategies (eg, distraction, reinterpretation) rely on cognitive skills that might be enhanced by education. In the pain field, low levels of education are associated with maladaptive pain beliefs and coping strategies.38 Further examination of racial group and educational differences may provide valuable information to inform treatment and research on racial disparities and pain coping.
In the current study, we examined race differences in the pain experience. First, we expected that African-American participants would report significantly more pain severity, interference, and disability than Caucasian participants. In addition, racial group differences in some coping strategies (eg, prayer and hoping, distraction, reinterpretation) were expected. Second, we expected that education would mediate these racial group differences. Third, it was hypothesized that education and race would moderate the relationship between pain coping and the pain variables.
Methods
Participants
Participants were recruited through newspaper advertisements in the Detroit metropolitan area for a larger study of couples and chronic pain (N = 139). The sample was ethnically and racially diverse (55% Caucasian, 37% African-American, 8% other racial/ethnic groups such as Native American, Asian, and Hispanic/Latino). Participants who self-identified as Caucasian (n = 69) or African-American (n = 58) were retained for further analysis. Participants were predominantly female (n = 75, 59%) and were 53.64 (SD = 13.10) years old on average. They reported an average income of $53,409.23 (SD = $33,001.51). Participants completed an average of 14.02 (SD = 2.54) years of formal education in school, by their own reports. Of the African American participants, approximately 10% (n = 6) reported fewer than 12 years of education, 29% (n = 17) reported 12 years (high school degree or high school equivalent), 55% (n = 32) reported some college or completion of bachelor’s degree, and 5% (n = 3) reported graduate work. Of the Caucasian participants, 6% (n = 4) reported fewer than 12 years of education, 26% (n = 18) reported 12 years, 46% (n = 32) reported some college or completion of bachelor’s degree, and 21% (n = 15) reported graduate work. Thus, the distribution in education appears to be similar for each group with the exception of graduate-level education. The average pain duration was 118.41 (SD = 125.54) months. Positive skew explains the large variance in pain duration. The most common pain location was the lower back. Eighty-six percent (n = 109) had received a diagnosis for the pain, and of those who had received a diagnosis, the most common pain problems were osteoarthritis (n = 50, 46%), spine or disk problems (n = 27, 25%), fibromyalgia (n = 7, 6%), and other musculoskeletal pain problems including pain resulting from fracture (n = 9, 8%). There were no racial group differences on each diagnosis type, P > .05, with the exception of spine or disk problems, χ2 (N = 109) = 3.90, P < .05, a diagnosis reported more frequently by Caucasian (n = 20) than African-American (n = 7) participants.
Measures
The Coping Strategies Questionnaire-Revised (CSQ-R) was used to assess 5 different pain-coping strategies: diverting attention, ignoring pain sensations, reinterpreting pain sensations, coping self-statements, and prayer and hoping. Catastrophizing was not examined because of the debate about whether it is an appraisal, coping strategy, or both.15,20,39 Researchers have suggested using the CSQ-Revised rather than the original Coping Strategies Questionnaire37 because of improved factor structure and reliability of subscales, especially with Af-rican-American samples.14,35,36 The behavioral activation subscale in the CSQ is not found in the CSQ-R because of poor reliability. The inter-item reliabilities of the 5 CSQ-R subscales were acceptable to excellent, and ranged from .73 to .83 for African-American participants and .80 to .87 for Caucasian participants.
Pain severity and interference were assessed with the Multidimensional Pain Inventory (Kerns et al, 1995). The MPI subscales have good psychometric properties.25-27 The 3-item pain severity subscale was used to assess participants’ perceptions of current pain severity and intensity. Pain severity was rated using 7-point Likert-type scales (eg, 0 = not at all severe, 6 = extremely severe). Two of the items referred specifically to the past week or the time of study participation. The 9-item interference subscale was used to assess the degree to which participants perceived the pain to interfere with or change their satisfaction with and ability to engage in everyday, work, social, and interpersonal activities. The MPI does not direct participants to a specific time frame on which to report interference, but they most likely reported about current interference as these items were imbed-ded in section 1 of the MPI, which contained other items referring to the past week. The wording limits the gen-eralizability of the interference results because it cannot be assumed that participants are referring to current interference. Interference was rated using 7-point Likert-type scales (eg, 0 = no change, 6 = extreme change). In the current study, interitem reliabilities for both pain severity and interference were acceptable to excellent for African-Americans (pain severity: α = .76; interference: α = .92) and Caucasians (pain severity: α = .80; interference: α = .76).
The Sickness Impact Profile3 was used to measure physical and psychosocial disability. The SIP has good convergent and discriminant validity and excellent inter-item and test-retest reliabilities.3,27 Participants reported on the presence of behaviors on the day of assessment. Following Bergner et al,3,27 each item was weighted to indicate the degree to which the behavior affects daily life and then items within each subscale were summed. The following SIP subscales were used in the current study: physical disability (45 items; ie, disability in ambulation, body care and movement, mobility) and psychosocial disability (48 items; ie, social interaction, communication, alertness, emotion). The interitem reliabilities of the physical disability were excellent for African-Americans (α = .86) and Caucasians (α = .82). Similarly, the reliabilities of psychosocial disability were excellent for African-Americans (α = .91) and Caucasians (α = .87).
Procedure
This study was approved by the Wayne State University Institutional Review Board. Eligible participants for the larger study were individuals with chronic pain and their spouses. Note that, for this report, only individuals with chronic pain were examined. Exclusionary criteria included pain duration of less than 6 months, presence of psychotic symptoms, presence of cognitive impairment as assessed with a phone version of the Mini-Mental Status Examination,11 and presence of a terminal illness. Participants attended a 3-hour lab session with their spouses where they completed consent forms, surveys, interviews, and videotaped interactions as part of the larger study. Couples were paid $100 upon completion of the study.
Data Analysis Plan
Participants who did not complete items pertaining to education or coping were excluded from further analysis (N = 22 ). As noted in the Participants section, only participants who self-identified as Caucasian or African-American were retained for further analysis. Therefore, unless otherwise indicated, analyses presented below included 43 African-American and 62 Caucasian participants (N = 105 ). The noncompleters did not differ from completers on the dependent variables (ie, pain severity, interference, disability), P values > .50.
T-tests were conducted to test whether there were racial group differences in education, pain variables (ie, pain severity, interference, disability), and coping strategies. It was expected that African-Americans would report higher pain scores than Caucasians. In addition, Af-rican-Americans were expected to report greater use of prayer and hoping and diverting attention than Cauca-sians but lower use of coping self-statements and ignoring pain sensations. Analyses of covariance (ANCOVA) were performed to determine whether education mediated the relationship between race and pain variables. The significance level for these analyses was set at P < .05.
Correlations were then conducted to examine the relationships between education, pain variables, and coping. We expected that the coping variables would be negatively related to pain variables with the exception of prayer and hoping and diverting attention, which were expected to be positively related to pain. We also expected that education level would be positively correlated with pain and coping variables. Next, partial correlations were conducted to determine whether education mediated the relationship between coping and pain.
Finally, hierarchical regressions were conducted to determine whether race, education, or both explained the most variance in pain variables and to test whether race and education interacted with coping strategies in correlating with pain variables. We examined the relationships of gender and age with the pain variables to determine whether the former should be included as covariates. Gender was not significantly associated with any of the pain variables, P values > .13, whereas age was significantly associated with pain severity and interference (r values = −.27 and −.34, respectively, P values < .01). Therefore, age was included as a covariate in the regressions with pain severity and interference. Other potential covariates were explored including current major depressive disorder or dysthymia, pain duration, psychological treatment, and medication usage. Inclusion of these variables as covariates did not affect the regression results. Approximately 8% (n = 5) Caucasian and 19% (n = 8) African-American participants declined to provide family income data. We did not include income in the analyses because doing so would have adversely impacted power and resulted in a biased sample. After entering in covariates, the next step in the hierarchical regression consisted of education, race, and coping, followed by a step consisting of the 2-way interactions, and a last step including the 3-way interaction between race, education, and coping.
Of particular interest were the 2-way and 3-way interactions. The significance level for the regression analyses was set at P< .01 due to the number of regressions. Results for regressions with nonsignificant interactions are not displayed here because the results are similar to those presented in the correlations and ANCOVAs (ie, the extent to which education mediates the relationship between race, coping, and pain variables). Regression results not presented in this paper are available upon request from the first author. Significant interactions were plotted using the unstandardized regression coef-ficients (Bs) from the last step of the regression. Expected values were plotted for African-American and Caucasian participants with low (−1 SD) and high (+1 SD) values on education and coping.
Results
Racial Group Differences in Education, Pain Variables, and Coping
Mean level of education was significantly higher in the Caucasian group compared to the African-American group (see t column of Table 1). When accounting for the slight positive skew in education for Caucasian participants, this difference remained significant, t (101.39) = −2.45, P < .02). t tests also demonstrated that African-American participants reported significantly higher mean pain, interference, and disability compared to Cau-casian participants (see t column of Table 1). In addition, African-American participants reported using diverting attention coping and prayer and hoping significantly more often than Caucasian participants. No other racial group differences in coping strategies were found.
Table 1.
t Tests Comparing Racial Groups on Pain and Coping Variables and ANCOVAs Accounting for the Effect of Education
| RACIAL GROUP | ||||
|---|---|---|---|---|
| AFRICAN-AMERICAN | CAUCASIAN | |||
| VARIABLE | M (SD) | M (SD) | ta | Fb |
| Education (in years) | 13.42 (2.25) | 14.65 (2.87) | –2.35* | n/a |
| Pain severity | 12.07 (3.78) | 10.18 (3.58) | 2.61* | 3.44 |
| Interference | 35.14 (12.03) | 30.02 (13.52) | 2.00* | 1.91 |
| Physical disability | 12.21 (11.70) | 7.98 (8.04) | 2.20* | 2.14 |
| Psychosocial disability | 16.18 (16.57) | 9.15 (10.26) | 2.69** | 3.79 |
| Diverting attention | 12.28 (6.19) | 9.76 (5.70) | 2.15* | 3.54 |
| Reinterpreting pain sensations | 5.30 (6.19) | 4.37 (5.09) | .84 | .50 |
| Coping self-statements | 18.16 (4.21) | 17.03 (5.20) | 1.18 | 2.55 |
| Ignoring pain sensations | 12.65 (6.63) | 14.84 (7.41) | –1.55 | .83 |
| Prayer and hoping | 14.72 (3.58) | 8.20 (5.42) | 6.90** | 38.52** |
NOTE. N = 105 with the exception of N = 104 for correlations involving Ignoring Pain Sensations and Prayer and Hoping as 1 participant did not complete items in those subscales.
t test comparing African-American and Caucasian participant groups.
ANCOVA results when including education as a covariate.
P < .05.
P < .01.
An analysis of covariance (ANCOVA) was performed to examine the possibility that education, also a significant correlate of the pain and coping variables as seen in Table 2, mediated the relationship between racial group and these other variables. Race remained a significant correlate of prayer and hoping (see F column of Table 1) with education as a significant covariate, F (1, 101) = 16.47, P < .0001. However, race was no longer a signifi-cant correlate of the other pain and coping variables (see F column of Table 1), supporting the mediating role of education.
Table 2.
Correlations Among Education, Pain Variables, and Coping
| 1. | 2. | 3. | 4. | 5. | 6. | 7. | 8. | 9. | |
|---|---|---|---|---|---|---|---|---|---|
| 1. Education | |||||||||
| 2. Pain severity | –.38** | ||||||||
| 3. Interference | –.30** | .61** | |||||||
| 4. Physical disability | –.36** | .43** | .45** | ||||||
| 5. Psychosocial disability | –.38** | .48** | .46** | .63** | |||||
| 6. Diverting attention | –.14 | .11 | .09 | .14 | .09 | ||||
| 7. Reinterpreting pain sensations | –.07 | .18 | .16 | .13 | .27** | .26** | |||
| 8. Coping selfstatements | .15 | –.10 | –.15 | –.25** | –.17 | .30** | .22* | ||
| 9. Ignoring pain sensations | .28** | –.13 | –.21* | –.19 | –.13 | .10 | .44** | .46** | |
| 10. Prayer and hoping | –.44** | .28** | .27** | .34** | .32** | .44** | .16 | .23* | –.11 |
NOTE. N = 105 with the exception of N = 104 for correlations involving Ignoring Pain Sensations and Prayer and Hoping as 1 participant did not complete items in those subscales.
P < .05.
P < .01.
Correlations Among Education, Coping, and Pain Variables
As shown in Table 2, diverting attention was not sig-nificantly related to pain variables, whereas prayer and hoping was consistently and positively correlated with each pain variable. Ignoring pain sensations was negatively correlated with interference ratings and coping self-statements were related to lower reported physical disability. On the other hand, reinterpreting pain sensations was associated with greater psychosocial disability.
Education was negatively and significantly correlated with the pain variables, indicating that higher levels of education were associated with less pain and disability. Education was positively associated with the use of ignoring pain sensations but negatively associated with the use of prayer and hoping.
Because education was significantly related to both ignoring pain sensations and prayer and hoping, partial correlations between these coping variables and the pain variables were performed. Prayer and hoping remained a significant correlate of physical disability (r =.22, P < .05. However, prayer and hoping was no longer a significant correlate of pain severity (r = .14, P > .05), interference (r = .16, P > .05), and psychosocial disability (r = .19, P > .05). Ignoring pain sensations was no longer a significant correlate of psychosocial disability (r =−.03, P > .05) or interference (r = −.13, P < .05). In other words, education partially mediated the relationship between some coping and pain variables but not others.
Hierarchical Regressions
To examine the potential moderating role of education in the relationship between race and pain variables, hierarchical regressions were performed. None of these interactions were significant for pain severity and interference, suggesting that the effect of education was limited to mediation as demonstrated earlier by the t-tests and ANCOVAs.
However, there were significant interactions in examining physical disability. As demonstrated in Table 3, a significant 3-way interaction between race, education, and reinterpreting pain sensations emerged. All regressions were also conducted without participants with education levels >16 years to account for the slight positive skew in education found in the Caucasian group. We present the analyses conducted on the full sample because the results were similar with and without the highly educated participants.
Table 3.
Hierarchical Regression Examining Race, Education, Reinterpreting Pain Sensations, and Their Interactions As Correlates of Physical Disability
| B | SE | Beta | ΔR2 | R2 | |
|---|---|---|---|---|---|
| Step 1 | .16** | .16** | |||
| Race | –2.60 | 1.88 | –.13 | ||
| Education | – .20 | .34 | –.33** | ||
| Reinterpreting pain sensations | .17 | .16 | .10 | ||
| Step 2 | .04 | .20** | |||
| Education X Race | –1.20 | .75 | –.85 | ||
| Education X Reinterpreting pain sensations | .02 | .07 | .14 | ||
| Race X Reinterpreting pain sensations | .47 | .34 | .44 | ||
| Step 3 | .07** | .27** | |||
| Race X Education X Reinterpreting pain sensations | –.52 | .17 | –6.62** |
B, unstandardized regression coefficient. SE, standard error of B. Beta, standardized regression coefficient.
NOTE. N = 105.
P < .05.
P < .01.
Figure 1 depicts the expected values for Caucasian and African-American participants with lower and higher education levels, which were calculated using the unstandardized regression coefficients from the final step of the regression. Caucasian and African-American participants with higher levels of education appear to report the highest level of physical disability when using less reinterpretation but report low physical disability at higher levels of reinterpretation. In contrast, for both racial groups with lower levels of education, greater use of reinterpretation was associated with greater physical disability. In addition, the Caucasian group’s mean disability scores appear to be greater than those of the African-American group.
Figure 1.
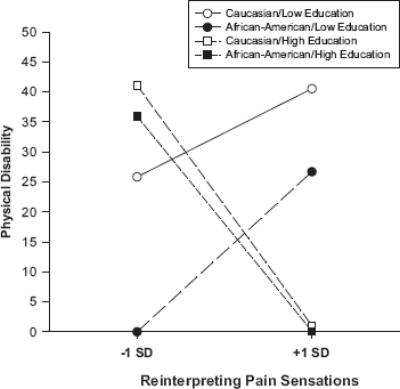
Expected physical disability scores based on race, education, and the use of reinterpreting pain sensations. Low and high education levels are represented by −1 SD and +1 SD from mean education, respectively. Expected disability scores were calculated on the basis of the regression results presented in Table 3.
Table 4 and Figure 2 show a different 3-way interaction between race, education, and coping self-statements in relating to physical disability. Unlike the results for reinterpretation, greater use of coping self-statements was associated with less disability in Caucasian participants with lower levels of education. In addition, Caucasian participants with lower education and who reported using lower levels of reinterpretation reported the highest physical disability. The pattern of results was similar for African-American participants with either low or high education, albeit this negative relationship was weaker than for the Caucasian participants with lower education. In contrast, there was a slight positive association between the use of coping self-statements and physical disability for Caucasian participants reporting higher educational levels.
Table 4.
Hierarchical Regression Examining Race, Education, Coping Self-Statements, and Their Interactions As Correlates of Physical Disability
| B | SE | BETA | 3R2 | R2 | |
|---|---|---|---|---|---|
| Step 1 | .20** | .20** | |||
| Race | –3.46 | 1.85 | –.17 | ||
| Education | –1.06 | .34 | –.29** | ||
| Coping self-statements | –.47 | .19 | –.23** | ||
| Step 2 | .03 | .23** | |||
| Education X Race | –1.12 | .78 | –.80 | ||
| Education X Coping self-statements | .01 | .08 | .10 | ||
| Race X Coping self-statements | –.30 | .42 | –.35 | ||
| Step 3 | .06** | .28**a | |||
| Race X Education X | .54 | .20 | 9.42** | ||
| Coping self-statements |
B, unstandardized regression coefficient. SE, standard error of B. Beta, standardized regression coefficient.
NOTE. N = 105.
R2s do not sum to final R2 because of rounding.
P < .05.
P < .01.
Figure 2.
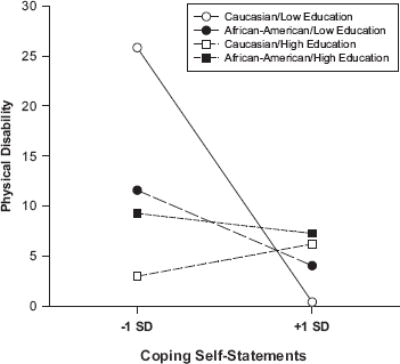
Expected physical disability scores based on race, education, and the use of coping self-statements. Low and high education levels are represented by −1 SD and +1 SD from mean education, respectively. Expected disability scores were calculated on the basis of the regression results presented in Table 4.
As for physical disability, greater use of coping self-statements were associated with less psychosocial disability for Caucasian participants reporting lower levels of education (see Table 5, Fig 3). This association is also found for African-American participants reporting lower levels of education, although to a greater degree than when examining physical disability. In contrast, there was a slight positive association between the use of coping self-statements and physical disability for Caucasian and African-American participants reporting higher educational levels. This effect appears to be more pronounced for Caucasian participants.
Table 5.
Hierarchical Regression Examining Race, Education, Coping Self-Statements, and Their Interactions As Correlates of Psychosocial Disability
| B | SE | BETA | &R2 | R2 | |
|---|---|---|---|---|---|
| Step 1 | .19** | .19** | |||
| Race | –5.58 | 2.55 | –.20* | ||
| Education | –1.56 | .47 | –.31** | ||
| Coping self-statements | –.41 | .26 | –.15 | ||
| Step 2 | .01 | .20** | |||
| Education X Race | –.60 | 1.08 | –.31 | ||
| Education X Coping self-statements | .09 | .11 | .59 | ||
| Race X Coping self-statements | –.28 | .58 | –.24 | ||
| Step 3 | .06** | .26** | |||
| Race X Education X | .76 | .28 | 9.64** | ||
| Coping self-statements |
B, unstandardized regression coefficient. SE, standard error of B. Beta, standardized regression coefficient.
NOTE. N = 105.
P < .05.
P < .01.
Figure 3.
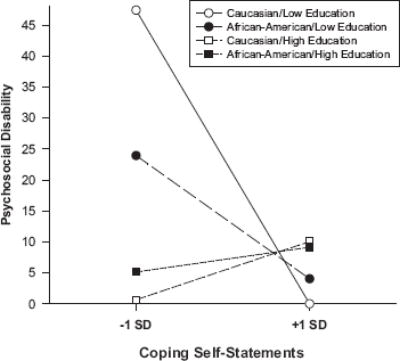
Expected psychosocial disability scores based on race, education, and the use of coping self-statements. Low and high education levels are represented by −1 SD and +1 SD from mean education, respectively. Expected disability scores were calculated on the basis of the regression results presented in Table 5.
Note that the 2-way interactions between race and coping, race and education, and coping and education were not significant in all other regressions in which the significant 3-way interaction was absent. The lack of 2-way interactions suggests that there are no other significant race differences in the relationship between coping styles (ie, diverting attention, reinterpreting pain sensations, coping-self-statements, ignoring pain sensations, prayer and hoping) and the pain variables. In addition, there were no other significant race differences in the associations between education and pain variables and no differences in the relationships between coping and pain variable at different levels of education.
Discussion
The purpose of this paper was to examine racial group differences in coping and pain variables and to determine whether both race and education mediated and moderated the relationship between coping and pain. As in previous studies,4,5,8,13,34,40,41 we found that African-American participants, on average, reported more pain, interference, and disability than their Caucasian counterparts. In addition, we found that African-American participants reported using diverting attention and prayer and hoping more than Caucasian participants. These findings also support prior work.21 However, unlike Jordan et al,21 we did not find that Caucasian participants were more likely to ignore the pain or to use coping self-statements, perhaps because the current sample reported muscu-loskeletal rather than RA pain. These findings, with the exception of prayer and hoping, disappeared when accounting for educational attainment. That is, any racial group differences on these variables are likely due mediated by racial group differences in education. These results demonstrate the importance of looking into mediators of racial group differences that are modifiable and potentially targets of prevention and intervention.
We also examined the relationships between coping strategies and each of the pain variables. Prayer and hoping was positively related to pain severity, interference, and physical and psychosocial disability, which is consistent with prior work.9,21,28,42 After controlling for education, only the significant correlation for physical disability remained. Education also mediated the associations between ignoring pain sensations, psychosocial disability, and interference. The variable of education may be related to reading ability, ability and knowledge about how to search for information about health and treatment, and communication skills. Persons without the educational resources to use or investigate more complex pain-coping strategies may use prayer and hoping or ignoring pain sensations in isolation from other strategies and may therefore also have problems with psychosocial disability, pain, and interference. Reinterpretation was negatively associated with psychosocial disability, suggesting that reinterpretation reduces psychosocial disability, persons with less disability find it easier to engage in cognitive reinterpretation, or both.
Hierarchical regressions revealed that education and race moderated some of the coping and pain relationships. Specifically, race, education, and reinterpreting pain sensations interacted with each other in correlating with physical disability. The use of reinterpreting pain sensations was negatively correlated with physical disability for participants of either race who reported higher levels of education. In contrast, reinterpreting pain sensations was associated with higher physical disability for participants with lower education. Reinterpreting pain sensations is a coping strategy that relies heavily on imagination and thought processes. Persons with higher levels of education may have more practice or more success in using strategies that involve complex cognitions about pain sensations. In contrast, reinterpreting pain sensations may be too demanding or may lead to increased attention to pain and disability for persons who may have not had as much practice or training in this coping strategy. It is also possible for these results to be interpreted in light of John Henryism, which consists of persistent, effort-ful coping in the face of chronic stress. James and colleagues17-19 found that this type of coping relates to negative health outcomes in African-American and Caucasian adults with low socioeconomic status. In this sample, persistent use of reinterpretation in persons with lower educational levels may detract from one’s quality of life. However, longitudinal and experimental research is necessary before temporal or causal conclusions can be made.
Coping self-statements interacted with race and education in relating to physical and psychosocial disability. This time, greater use of coping self-statements was associated with less physical and psychosocial disability for Caucasian participants with lower education. A similar relationship was demonstrated for Af-rican-American participants with lower education, but this relationship appears to be weaker when examining physical versus psychosocial disability. It is difficult to apply the John Henryism concept to these findings because one would expect persons with lower education who focus on their own efforts to overcome pain to report more disability. Perhaps coping self-statements is an effective strategy for these groups because it is perceived as a commonsense, straightforward coping strategy that is effective in pain coping. The nearly flat slopes for African-American participants with greater education suggests that coping self-statements were weakly related to physical or psychosocial disability. Research is needed to determine the extent to which coping self-statements are perceived as effective in this group. Interestingly, the use of coping self-statements among Caucasian participants with greater education levels was associated with greater disability, especially with respect to psychosocial disability. For Caucasians with high educational levels, it is possible that experience with other cognitive strategies makes it more difficult to implement coping self-statements. Alternatively, this group may appraise self-statements as an ineffective or naïve way to deal with pain. Additional research may determine that greater use of coping self-statements are effective for individuals of any educational level regardless of appraisals of effectiveness or that persons with lower psychosocial disability are better able to engage in this type of coping. Cultural or societal background factors may also account for the different relationships between coping and physical disability for Caucasians and African Ameri-cans at higher educational levels. For instance, researchers have found that ethnic identity is related to coping styles and locus-of-control.2 Further research may reveal that a combination of intrapersonal and interpersonal experiences shape individuals’ perceptions and appraisals of the effectiveness of different types of pain coping.
Race and education did not interact with coping selfstatements and reinterpreting pain sensations in relating to pain severity or interference. These results combined with the correlation results showing an absence of correlations among these variables suggest that the effects of coping self-statement and reinterpretation are limited to perceived limitations (ie, disability) or that disability impacts individuals’ coping choices or frequency. Diverting attention, ignoring pain sensations, and prayer and hoping did not interact with race or education in correlating with any of the pain variables. In other words, any significant correlations between these coping strategies and pain variables were consistent across racial and educational groups. These results contrast with those of Jordan et al,21 who found racial group differences in the correlations between prayer and hoping and reinterpreting pain sensations with pain variables. Perhaps, sample differences (eg, diagnosis, disease severity, study setting) account for the different findings.
One of the strengths of the study was the assessment of 4 related but distinct aspects of the pain experience, including pain severity, interference, and 2 types of disability. However, it is important for researchers to also use more objective measures of pain and disability (eg, observation) to determine whether the race and education findings can be generalized to different measures of pain and to assess a variety of pain-related health behaviors including sleep and appetite. Research with more than 2 racial groups (eg, Asian-Amer-icans, Native Americans) and with persons of different ethnic backgrounds (eg, Hispanics/Latinos) as well as research with non-married and non-self-selected samples experiencing a variety of pain problems is also needed to examine how well the current findings generalize to other samples. Race as a variable of interest must also be understood as an imprecise variable, one that may function as a proxy variable for historical social and political policy, genetic variability, or other variables.16,31 Likewise, educational attainment may be highly correlated with types of employment that may put individuals at greater risk for injury, pain, and disability. Educational attainment might also be related to income and socioeconomic status, variables that were not examined in this study. In the current study, there was some positive skew in education for Caucasians but not in African Americans. While we attempted to account for this finding in our analyses, it may have contributed to the pattern of results found here. Therefore, racial group and educational differences should be interpreted in a cautious manner and additional variables that may underlie these differences should be explored.
Nevertheless, the current study has several notable findings. First, racial group differences in pain severity, interference, disability, and pain coping are mediated by education attainment. Second, a more complex relationship exists between race, education, and coping in relating to physical and psychosocial disability. Researchers should continue to search for variables that might explain racial group differences in an effort to inform theory and clinical work. The fact that educational attainment accounts for some of the racial group differences and also interacts with race in other analyses, suggests that clinicians and intervention researchers should include education as an important variable of interest. Perhaps, coping measures or coping instructional material could be adapted for individuals with different educational backgrounds. Alternatively, some individuals with pain might need to be encouraged to practice and engage in certain types of coping strategies before positive effects can be seen. Continued research aimed at other variables that might mediate or interact with race and education is strongly encouraged.1-43
Acknowledgments
The authors thank the members of the Relationships and Health Lab for their help in conducting this study.
Footnotes
The first author was supported by Grant K01 MH66975 while working on this paper.
References
- 1.Affleck G, Urrows S, Tennen H, Higgins P. Daily coping with pain from rheumatoid arthritis: Patterns and correlates. Pain. 1992;51:221–229. doi: 10.1016/0304-3959(92)90263-B. [DOI] [PubMed] [Google Scholar]
- 2.Bates M, Edwards W. Ethnic variations in the chronic pain experience. Ethn Dis. 1992;2:63–83. [PubMed] [Google Scholar]
- 3.Bergner M, Bobbitt RA, Carter WB, Gilson BS. The Sickness Impact Profile: Development and final revision of a health status measure. Med Care. 1981;19:787–805. doi: 10.1097/00005650-198108000-00001. [DOI] [PubMed] [Google Scholar]
- 4.Chibnall JT, Tait RC. Disparities in occupational low back injuries: predicting pain-related disability from satisfaction with case management in African Americans and Cauca-sians. Pain Medicine. 2005;6:39–48. doi: 10.1111/j.1526-4637.2005.05003.x. [DOI] [PubMed] [Google Scholar]
- 5.Chibnall JT, Tait RC, Andresen EM, Hadler NM. Race and socioeconomic differences in post-settlement outcomes for African American and Caucasian Workers’ Compensation claimants with low back injuries. Pain. 2005;114:462–472. doi: 10.1016/j.pain.2005.01.011. [DOI] [PubMed] [Google Scholar]
- 6.Dominick K, Baker T. Racial and ethnic differences in osteoarthritis: Prevalence, outcomes, and medical care. Ethn Dis. 2004;14:558–566. [PubMed] [Google Scholar]
- 7.Dunn KS, Horgas AL. Religious and nonreligious coping in older adults experiencing chronic pain. Pain Manag Nurs. 2004;5:19–28. doi: 10.1016/s1524-9042(03)00070-5. [DOI] [PubMed] [Google Scholar]
- 8.Edwards RR, Doleys DM, Fillingim RB, Lowery D. Ethnic differences in pain tolerance: Clinical implications in a chronic pain population. Psychosom Med. 2001;63:316–323. doi: 10.1097/00006842-200103000-00018. [DOI] [PubMed] [Google Scholar]
- 9.Edwards RR, Moric M, Husfeldt B, Buvanendran A, Ivank-ovich O. Ethnic similarities and differences in the chronic pain experience: A comparison of African American, His-panic, and White patients. Pain Medicine. 2005;6:88–98. doi: 10.1111/j.1526-4637.2005.05007.x. [DOI] [PubMed] [Google Scholar]
- 10.Evers AWM, Kraaimaat FW, Geene R, Jacobs JWG, Bijl-sma JWJ. Pain coping and social support as predictors of long-term functional disability and pain in early rheumatoid arthritis. Behaviour Research & Therapy. 2003;41:1295–1310. doi: 10.1016/s0005-7967(03)00036-6. [DOI] [PubMed] [Google Scholar]
- 11.Folstein M, Folstein S, McHugh P. Mini-mental state: A practical method for grading the state of patients for the clinician. Journal of Psychiatric Research. 1975;31:251–259. doi: 10.1016/0022-3956(75)90026-6. [DOI] [PubMed] [Google Scholar]
- 12.Green C, Anderson K, Baker T, Campbell L, Decker S, Fillingim R, Kalauokalani D, Lasch K, Myers C, Tait R, Todd K, Vallerand A. The unequal burden of pain: Confronting racial and ethnic disparities in pain. Pain Medicine. 2003;4:277–294. doi: 10.1046/j.1526-4637.2003.03034.x. [DOI] [PubMed] [Google Scholar]
- 13.Green CR, Ndao-Brumblay SK, Nagrant AM, Baker TA, Rothman E. Race, age, and gender influences among clusters of African American and White patients with chronic pain. J Pain. 2004;5:171–182. doi: 10.1016/j.jpain.2004.02.227. [DOI] [PubMed] [Google Scholar]
- 14.Hastie BA, Riley JL, Fillingim RB. Ethnic differences in pain coping: Factor structure of the Coping Strategies Questionnaire and Coping Strategies Questionnaire-Revised. J Pain. 2004;5:304–316. doi: 10.1016/j.jpain.2004.05.004. [DOI] [PubMed] [Google Scholar]
- 15.Haythornthwaite JA, Menefee LA, Heinberg LJ, Clark MR. Pain coping strategies predict perceived control over pain. Pain. 1998;77:33–39. doi: 10.1016/S0304-3959(98)00078-5. [DOI] [PubMed] [Google Scholar]
- 16.Helms J, Jernigan M, Mascher J. The meaning of race in psychology and how to change it. Am Psychol. 2005;60:27–36. doi: 10.1037/0003-066X.60.1.27. [DOI] [PubMed] [Google Scholar]
- 17.James S, Hartnett S, Kalsbeek W. John Henryism and blood pressure differences among Black men. J Behav Med. 1984;6:259–278. doi: 10.1007/BF01315113. [DOI] [PubMed] [Google Scholar]
- 18.James S, LaCroix A, Kleinbaum D, Strogatz D. John Hen-ryism and blood pressure differences among Black Men: II. The role of occupational stressors. J Behav Med. 1984;7:259–275. doi: 10.1007/BF00845359. [DOI] [PubMed] [Google Scholar]
- 19.James S. John Henryism and the health of African-Amer-icans. Cult Med Psychiatry. 1994;18:163–182. doi: 10.1007/BF01379448. [DOI] [PubMed] [Google Scholar]
- 20.Jensen MP, Turner JA, Romano JM. Changes in beliefs, catastrophizing, and coping are associated with improvement in multidisciplinary pain treatment. J Consult Clin Psy-chol. 2001;69:655–662. doi: 10.1037//0022-006x.69.4.655. [DOI] [PubMed] [Google Scholar]
- 21.Jordan MS, Lumley MA, Leisen JCC. The relationships of cognitive coping and pain control beliefs to pain and adjustment among African-American and Caucasian women with rheumatoid arthritis. Arthritis Care & Research. 1998;11:80–88. doi: 10.1002/art.1790110203. [DOI] [PubMed] [Google Scholar]
- 22.Keefe FJ, Caldwell DS, Baucom D, Salley A. Spouse-assisted coping skills training in the management of osteoar-thritic knee pain. Arthritis Care & Research. 1996;9:279–291. doi: 10.1002/1529-0131(199608)9:4<279::aid-anr1790090413>3.0.co;2-6. [DOI] [PubMed] [Google Scholar]
- 23.Keefe FJ, Caldwell DS, Baucom D, Salley A, Robinson E, Timmons K, Beaupre P, Weisberg J, Helms M. Spouse-assisted coping skills training in the management of knee pain in osteoarthritis: Long-term followup results. Arthritis Care & Research. 1999;12:101–111. doi: 10.1002/1529-0131(199904)12:2<101::aid-art5>3.0.co;2-9. [DOI] [PubMed] [Google Scholar]
- 24.Keefe FJ, Blumenthal J, Baucom D, Affleck G, Waugh R, Caldwell DS, Beaupre P, Kashikar-Zuck S, Wright K, Egert J, Lefebvre J. Effects of spouse-assisted coping skills training and exercise training in patients with osteoarthritic knee pain: a randomized controlled study. Pain. 2004;110:539–549. doi: 10.1016/j.pain.2004.03.022. [DOI] [PubMed] [Google Scholar]
- 25.Kerns RD, Turk DC, Rudy TE. The West Haven-Yale Multidimensional Pain Inventory (WHYMPI) . Pain. 1985;23:345–356. doi: 10.1016/0304-3959(85)90004-1. [DOI] [PubMed] [Google Scholar]
- 26.Kerns RD, Turk DC, Rudy TE. The West Haven-Yale Multidimensional Pain Inventory. Pain. 1985;23:345–356. doi: 10.1016/0304-3959(85)90004-1. [DOI] [PubMed] [Google Scholar]
- 27.Kerns RD, Jacob MC. Assessment of the psychosocial context of the experience of chronic pain. In: Turk DC, Melzack R, editors. Handbook of Pain Assessment. New York: Guilford Press; 1992. pp. 235–253. [Google Scholar]
- 28.Lamé IE, Peters ML, Vlaeyen JWS, Kleef Mv, Patijn J. Quality of life in chronic pain is more associated with beliefs about pain, than with pain intensity. Eur J Pain. 2005;9:15–24. doi: 10.1016/j.ejpain.2004.02.006. [DOI] [PubMed] [Google Scholar]
- 29.Lazarus RS, Folkman S. Springer. New York: 1984. Stress, Appraisal, and Coping. [Google Scholar]
- 30.Mayberry RM, Mili F, Ofili E. Racial and ethnic differences in access to medical care. Med Care Res Rev. 2000;57(Suppl 1):108–45. doi: 10.1177/1077558700057001S06. [DOI] [PubMed] [Google Scholar]
- 31.Ossorio P, Duster T. Race and genetics: Controversies in biomedical, behavioral, and forensic sciences. Am Psychol. 2005;60:115–118. doi: 10.1037/0003-066X.60.1.115. [DOI] [PubMed] [Google Scholar]
- 32.Paulson M, Dekker A. Healthcare disparities in pain management. J Am Osteopath Assoc. 2005;105:14–17. [PubMed] [Google Scholar]
- 33.Prevention CfDCa : Racial/ethnic differences in the prevalence and impact of doctor-diagnosed arthritis-United States, 2002. Morbidity and Mortality Weekly Report 54 119 123 2005
- 34.Riley I, Joseph L, Wade JB, Myers CD, Sheffield D, Papas RK, Price DD. Racial/ethnic differences in the experience of chronic pain. Pain. 2002;100:291–298. doi: 10.1016/S0304-3959(02)00306-8. [DOI] [PubMed] [Google Scholar]
- 35.Riley JL, Robinson ME. CSQ: Five factors or fiction? Clin J Pain. 1997;13:156–162. doi: 10.1097/00002508-199706000-00010. [DOI] [PubMed] [Google Scholar]
- 36.Riley JL, Robinson ME, Geisser ME. Empirical subgroups of the Coping Strategies Questionnaire-Revised: A multi-sample study. Clin J Pain. 1999;15:111–116. doi: 10.1097/00002508-199906000-00007. [DOI] [PubMed] [Google Scholar]
- 37.Rosenstiel AK, Keefe FJ. The use of coping strategies in chronic low back pain patients: Relationship to patient characteristics and current adjustment. Pain. 1983;17:33–44. doi: 10.1016/0304-3959(83)90125-2. [DOI] [PubMed] [Google Scholar]
- 38.Roth RS, Geisser ME. Educational achievement and chronic pain disability: Mediating role of pain-related cognitions. Clin J Pain. 2002;18:286–296. doi: 10.1097/00002508-200209000-00003. [DOI] [PubMed] [Google Scholar]
- 39.Severeijns R, Vlaeyen JWS, van den Hout MA. Do we need a communal coping model of pain catastrophizing? An alternative explanation. Pain. 2004;111:226–229. doi: 10.1016/j.pain.2004.07.024. [DOI] [PubMed] [Google Scholar]
- 40.Sheffield D, Biles PL, Orom H, Maixner W, Sheps DS. Race and sex differences in cutaneous pain perception. Psycho-som Med. 2000;62:517–523. doi: 10.1097/00006842-200007000-00010. [DOI] [PubMed] [Google Scholar]
- 41.Tan G, Jensen MP, Thornby J, Anderson KO. Ethnicity, control appraisal, coping, and adjustment to chronic pain among black and white Americans. Pain Medicine. 2005;6:18–28. doi: 10.1111/j.1526-4637.2005.05008.x. [DOI] [PubMed] [Google Scholar]
- 42.Turner JA, Jensen MP, Romano JM. Do beliefs, coping, and catastrophizing independently predict functioning in patients with chronic pain? Pain. 2000;85:115–125. doi: 10.1016/s0304-3959(99)00259-6. [DOI] [PubMed] [Google Scholar]
- 43.Turner JA, Jensen MP, Warms CA, Cardenas DD. Catastrophizing is associated with pain intensity, psychological distress, and pain-related disability among individuals with chronic pain after spinal cord injury. Pain. 2002;98:127–134. doi: 10.1016/s0304-3959(02)00045-3. [DOI] [PubMed] [Google Scholar]