

Abstract
Context: Instrumented helmets have been used to estimate impact acceleration imparted to the head during helmet impacts. These instrumented helmets may not accurately measure the actual amount of acceleration experienced by the head due to factors such as helmet-to-head fit.
Objective: To determine if an accelerometer attached to a mouthpiece (MP) provides a more accurate representation of headform center of gravity (HFCOG) acceleration during impact than does an accelerometer attached to a helmet fitted on the headform.
Design: Single-factor research design in which the independent variable was accelerometer position (HFCOG, helmet, MP) and the dependent variables were g and Severity Index (SI).
Setting: Independent impact research laboratory.
Intervention(s): The helmeted headform was dropped (n = 168) using a National Operating Committee on Standards for Athletic Equipment (NOCSAE) drop system from the standard heights and impact sites according to NOCSAE test standards. Peak g and SI were measured for each accelerometer position during impact.
Main Outcome Measures: Upon impact, the peak g and SI were recorded for each accelerometer location.
Results: Strong relationships were noted for HFCOG and MP measures, and significant differences were seen between HFCOG and helmet g measures and HFCOG and helmet SI measures. No statistically significant differences were noted between HFCOG and MP g and SI measures. Regression analyses showed a significant relationship between HFCOG and MP measures but not between HFCOG and helmet measures.
Conclusions: Upon impact, MP acceleration (g) and SI measurements were closely related to and more accurate in measuring HFCOG g and SI than helmet measurements. The MP accelerometer is a valid method for measuring head acceleration.
Keywords: helmet, head injury, measurement techniques
Key Points
An accelerometer attached to the mouthpiece provided a valid method for measuring the head acceleration and Severity Index.
An accelerometer attached to the helmet overestimated the head acceleration and Severity Index.
Placing an accelerometer in the mouthpiece permits direct assessment of the actual acceleration experienced by the head and not simply the acceleration of the helmet.
Approximately 300 000 athletes incur concussions in the United States each year.1–3 This may be a conservative estimate because many minor head injuries go unreported. Although most concussions occur in high-impact sports, athletes in low-impact sports are not immune to mild traumatic brain injury.4 Head injuries are caused by positive and negative acceleration forces experienced by the brain and may result from linear or rotational accelerations (or both).5–7 Both linear and rotational accelerations are likely to be encountered by the head at impact, damaging neural and vascular elements of the brain.5,6
Identifying the magnitude of acceleration that causes brain injury may assist in prevention, diagnosis, and return-to-play decisions. Most field measurements assess the acceleration experienced by the player with accelerometers attached to the helmet.8–12 Helmets are designed to help mediate the amount of acceleration experienced by the head; therefore, accelerometers placed on the helmet may not reflect acceleration of the head.12–14 Testing impact acceleration to the head with an intraoral device may allow for both accurate measurements of accelerations in sports in which helmets are not worn and more precise examination of the acceleration limits of the brain in these sports. It could also assist in assessing the protective capabilities of a helmet for all helmeted sports.
An accepted method of impact testing involves the use of biofidelic headforms.15 These headforms are used by the National Operating Committee on Standards for Athletic Equipment (NOCSAE) in the impact testing of football, hockey, baseball, and lacrosse helmets. Each headform is instrumented with an accelerometer, located at the center of gravity, to measure the acceleration experienced by the helmeted headform upon impact in all of NOCSAE testing standards.
Our purpose was to determine if peak acceleration (g) and Gadd Severity Index (SI) values measured intraorally are more representative of headform center of gravity (HFCOG) acceleration and SI than are helmet g and SI values. We hypothesized that an accelerometer placed intraorally would measure impact acceleration of a headform more accurately than would an accelerometer attached to a helmet.
METHODS
Instrumentation
Modified Headform
A NOCSAE medium-sized headform (model JBMA-03; Overland Park, KS) was modified (Figure 1) with 3 triaxial accelerometers (model 355-17; PCB Piezotronics, Inc, Depew, NY) for testing. The NOCSAE headform is a biofidelic headform with a glycerin-filled brain cavity (Rapid Mold Prototype, Marne, MI).15 This headform is designed to take on anthropometric characteristics of the human head. The medium headform and neck assembly weighs 4.8 kg and is 575 mm in circumference.15 The triaxial accelerometers measure the peak acceleration in 3 orthogonal axes: anterior-posterior (x), inferior-superior (y), and side-side (z).
Figure 1. Modified National Operating Committee on Standards for Athletic Equipment (NOCSAE) headform with mouthpiece and headform center-of-gravity (HFCOG) accelerometers. The chin portion has been removed to show placement of accelerometer.
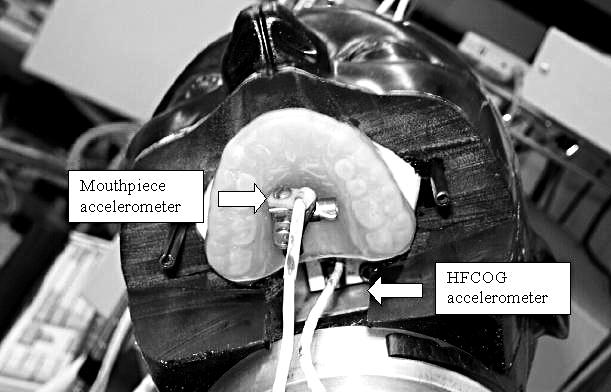
The following modifications were made to the headform: (1) The chin portion of the headform was cut off and a molded dentition fabricated by a licensed dentist was inserted into the headform to replicate the teeth and palate structure. (2) The dentition was held into place by 2 guide pins inserted into the headform. (3) A custom mouthpiece (MP) was made from the dentition mold and was placed onto the dentition covering the teeth and palate. The mouthpiece was not affixed to the dentition, so it would be similar to an athlete wearing a mouthpiece. (4) A 0.25-cm-diameter hole was placed in the center of the MP where the accelerometer wire passed through and connected to a data analyzer (model 200; KME Co, Troy, MI). (5) The chin portion was placed back on the headform with 2 guide pins.
Headform Calibration
The headform was mounted to a NOCSAE drop test system. The accelerometer was connected to a dedicated KME data analyzer. The nonhelmeted headform was calibrated according to NOCSAE test standards15–19 before testing using the calibration Modular Elastomer Programmer (Cadex Inc, St Jean-Sur-Richelieu, Quebec, Canada), which is a pad impact surface that is 3 in (7.6 cm) thick by 6 in (15.2 cm) in diameter. The front alignment was checked to ensure that the headform was as close to the center of the pad as possible without contacting the nose. The nonhelmeted headform was dropped onto the standard calibration locations: front, side, and top.15–19 Upon impact, the SI was calculated and peak g was recorded. The resultant SI was 1200 ± 2% at all 3 impact locations. The HFCOG, helmet, and MP accelerometers were calibrated at the HFCOG position according to NOCSAE test standards.15–19 After calibration at the center-of-gravity location, we placed the accelerometers at their testing positions; HFCOG, helmet, and MP. The voltages were recorded for X, Y, and Z channels of the 3 accelerometers.
Instrumentation Calibration
Three KME 200 data analyzers were calibrated according to NOCSAE test standards.15–19 The KME data analyzers are data acquisition systems that measure acceleration of the HFCOG, helmet, and MP accelerometers in peak g and calculate the SI. The KME data analyzers used a sampling frequency of 14 000 Hz with a 4-pole, 1-kHz, active low-pass filter on the vector resultant.15–19
Procedures
Helmet, Headform, and Mouthpiece Testing
The headform was properly fitted with a football helmet (model VSR-4; Riddell Inc, Memphis, TN), so the helmet did not move or slide on the headform.16–19 The position of the helmet was checked before each impact. Acceleration (peak g) and SI levels were measured and compared in a modified NOCSAE headform at the standard location (HFCOG) and experimental locations of the MP and helmet. Each accelerometer was connected to a dedicated KME 200 data analyzer that calculated peak g and SI levels. Testing procedures followed NOCSAE standards for football helmet testing onto the test modular elastomer programmer.15–19 The helmeted headform was dropped in a free fall from 46 cm, 92 cm, 122 cm, and 152 cm, landing on the test programmer in the standard locations: front, front boss, side, rear boss, rear, top, and one random location lower rear boss. Three drops were performed at each location. This procedure was repeated twice (n = 168). Each alignment was checked to make sure the helmeted headform impacted the programmer as close to the center of the pad as possible. Upon impact, peak g and SI were recorded for the HFCOG, helmet, and MP accelerometers. Precalibration and postcalibration impacts were performed to ensure reliable and valid measurements according to NOCSAE protocol.15,16 The NOCSAE-approved drop testing system (Figure 2) was calibrated according to standard guidelines before each test to ensure the accuracy of acceleration measurements.15–19 One triaxial accelerometer was placed in the center of gravity of the humanoid headform. A second triaxial accelerometer was attached firmly to the palate portion of the MP, which was custom-made to fit over the dentition. A third triaxial accelerometer was placed on the crown of the helmet (Figure 3).
Figure 2. National Operating Committee on Standards for Athletic Equipment impact test system. The helmeted headform was dropped from various heights onto the modular elastomer programmer (black pad).
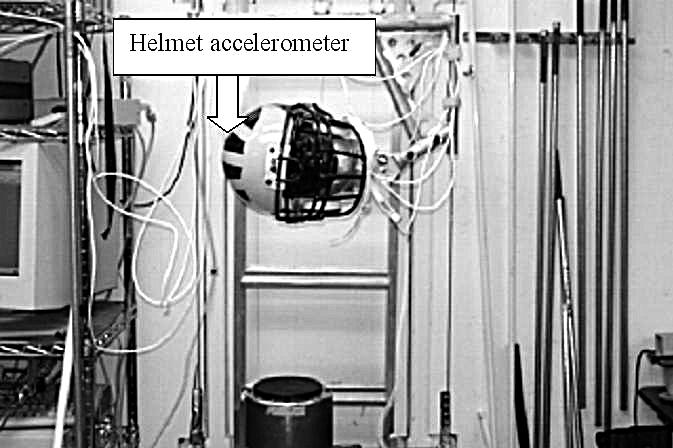
Figure 3. National Operating Committee on Standards for Athletic Equipment (NOCSAE) impact testing sites and reference planes according to DOC 001-98. F indicates front; R, rear; FB, front boss; RB, rear boss, Ref. plane, reference plane. Reprinted with permission from NOCSAE, Overland Park, KS.

Impact Sites and Reference Planes
The standard impact sites were front, front boss, side, rear boss, rear, and top (Figure 3). The front impact site is located in the median plane 1 in (2.54 cm) above the anterior intersection of the median and reference planes. The front boss is an impact point in the 45° plane from the median plane measured clockwise and located 1 in (2.54 cm) above the reference plane. The side impact is located at the intersection of the reference and coronal planes on the right side of the headform. The rear boss impact is a point on the reference plane located 135° clockwise from the anterior intersection of the median and reference planes. The rear impact is located at the posterior intersection of the median and reference planes. The top impact site is located at the intersection of the median and coronal planes, and the random impact is any point located in the area of protective coverage, on or above the basic plane but no closer than 1 in (2.54 cm) from the edge of the helmet. The random location in this study was the lower rear boss, which was chosen by simple random sample.15–19
Orientation planes were defined as follows. The reference plane is a plane marked on the headform at a specified distance above and parallel to the basic plane. The basic plane (Frankfort plane) is an anatomical plane that includes the superior rims of the auditory meatuses and the notches of the inferior orbital ridges. The coronal plane is an anatomical plane perpendicular to both the basic plane and the midsagittal plane and containing the midpoint of a line connecting the superior rims of the right and left auditory meatuses. The midsagittal (median) plane is an anatomical plane perpendicular to the basic plane and containing the midpoint of the line connecting the notches of the right and left inferior orbital ridges and the midpoint of the line connecting the superior rims of the right and left auditory meatus.15–19 The impact data from these sites were used to calculate the SI.
Data Reduction
Gadd Severity Index
The SI was developed to evaluate the extent of injury of an acceleration-time history experienced by simulated human heads due to impact.20 It correlates the severity of the head injury with the time and deceleration upon impact. A weight-impulse value is calculated by integrating the area under the acceleration-time curve after instantaneous accelerations have been raised to the 2.5 power:
 |
where a = instantaneous resultant acceleration expressed as a multiple of g, and dt = time increments in seconds. Integration was carried out over the essential duration (t) of the acceleration pulse. A weighting factor of 2.5 was based on impact data available to Gadd on animal and cadaver impacts that led to skull fracture.21,22 An SI of 1200 has been accepted by NOCSAE as the level of pass-fail for football helmets and is the maximum value that a sports helmet can sustain to be deemed acceptable for play. If a helmet has an SI above 1200 at any site during impact testing, it fails the test and is deemed unacceptable for play. A 1200 SI maximum value represents a threshold for a severe head injury such as skull fracture or subdural hematoma.22,23
Statistical Analysis
We calculated 2 separate 1-way analyses of variance tested for the main effect of accelerometer position (HFCOG, helmet, MP) using g and SI as dependent measures. Post hoc Scheffé tests were calculated to determine if significant differences existed among accelerometer measurements in the HFCOG, helmet, and MP (P < .05). Pearson correlation coefficients were used to determine relationships among the HFCOG and helmet and the HFCOG and MP g and SI measures. Linear regression analysis was used to determine relationships among HFCOG, helmet, and MP measures.
All statistics were calculated with SPSS (version 10.1; SPSS Inc, Chicago, IL) and Statistica for Windows (version 2000; StatSoft, Tulsa, OK).
RESULTS
Impact means and SDs for each triaxial accelerometer location at the 122-cm drop height are shown in Table 1. The HFCOG impact measures were significantly lower than the helmet impact measures for both SI (F2,501 = 345.0, P < .05) and g (F2,501 = 505.8, P < .05). No statistically significant differences were noted between HFCOG and MP SI and g measures (F2,501 = 0.347, P < .05 and F2,501 = 0.322, P < .05, respectively). A statistically significant correlation was seen between SI and g measures for HFCOG and MP. No significant correlation was found between HFCOG and helmet SI or g measures (P < .05) (Table 2).
Table 1. Impacts at Each Accelerometer Location (n = 168).

Table 2. Pearson Correlation Coefficient Values.

A linear regression analysis for HFCOG g and MP g revealed an r2 of .664, and for HFCOG and MP SI, an r2 of .927. Both were significant at the P < .01 levels. Linear regression analysis for HFCOG and helmet g revealed a weak r2 value (r2 = .245, P <.01). The HFCOG and helmet SI also showed a weak r2 value (r2 = .437, P < .01) (Figure 4).
Figure 4. Linear regressions of headform center of gravity (HFCOG) and helmet g measures, HFCOG and helmet Severity Index (SI) measures, HFCOG and mouthpiece g measures, and HFCOG and mouthpiece SI values (P < .01).

DISCUSSION
Our study demonstrated that an accelerometer attached to an MP in a NOCSAE helmeted headform is a valid measurement of acceleration and SI experienced by the HFCOG. No significant differences were noted between HFCOG and MP g and SI measurements, and a high correlation was seen between HFCOG and MP g and SI measurements. Conversely, an accelerometer placed on the helmet significantly overestimated accelerations and SI in a nonuniform manner that could not be related to the acceleration and SI measured at HFCOG. This is in agreement with the findings of Lewis et al,12 who stated that when hit with a pendulum device, accelerometers in helmet padding measured peak acceleration as 300% greater than accelerometers placed intraorally in cadaver heads. They also noted that intraoral measurements were highly correlated with simultaneous intracranial measurements and concluded that intraoral measurements of acceleration correlated better with intracranial measurements than did measurements taken in the helmet padding.12,13 Accelerometer placement in helmet padding appears to significantly overestimate the actual acceleration forces experienced by the head.13
Helmets are designed to reduce acceleration at the head, and if this did not occur, the helmet would not be performing its function in protecting the head from large impacts.13,24,25 Acceleration is reduced through deformation of the outer shell and liner that spreads the force throughout the helmet. An increase in acceleration to the head occurs when the foam liner “bottoms out.” When a material bottoms out, it loses the ability to absorb or to dissipate energy.24 By attaching the accelerometer to the MP and not to the helmet, the effects of the shell and liner properties are eliminated, allowing for the direct assessment of acceleration experienced by the head. The difference between HFCOG and helmet acceleration (g) and SI may have been due to the helmet liner, mass, or shell altering the acceleration experienced by the head.
Instrumented helmets have been used to estimate head acceleration upon impact.8–12,26 However, these results may not be an accurate estimation of the actual amount of acceleration the head experiences due to various factors, including helmet-to-head fit and helmet liner properties. The hard shell of the helmet spreads the impact force over a large surface area, and the helmet liner absorbs the acceleration forces, thereby reducing the amount of acceleration imparted to the head to nonconcussive levels.23,25,27–31 Therefore, if the helmet shell or liner is instrumented, it is very difficult to estimate the amount of acceleration passed to the head. Most sport helmets are effective in attenuating impacts with hard or stiff objects, such as other helmets, sticks, pucks, and trees. Impact is attenuated through deformation of a compliant, energy-absorbing layer inside the helmet. A person wearing a helmet will be better protected if (1) the energy is dissipated by the material inside the helmet, (2) the mass of the helmet reduces the velocity imparted upon the person's head, thereby decreasing the acceleration to the head, and (3) the compliant soft layer inside the helmet increases the time involved in the momentum transfer, reducing head acceleration.31 Our results show that helmet g and SI values were much higher than the HFCOG g and SI and MP g and SI values, suggesting that the helmet and liner absorb and dissipate the acceleration transferred to the head. Further, the results of this study showed that the acceleration values varied greatly between the helmet and the HFCOG. Thus, actual acceleration measures of the helmet should not be used to represent the acceleration experienced by the head.
Naunheim et al8 examined the level of head acceleration experienced by high school athletes. The authors investigated whether cumulative subconcussive impacts may cause neurologic deficits. The average peak acceleration measured was 29.1 ± 1 g for football impacts. Lewis et al12 measured peak g intraorally, intracranially, and in helmet padding. During impact with a soccer ball traveling at 39.3 mph (63.25 kph), 49.3 g was recorded at the helmet and 7.7 g intraorally. Mean peak acceleration intraorally was 19.2 g without a helmet under the same testing conditions. Naunheim et al31 collided a headform with soccer balls traveling at 3 speeds (9, 12, and 15 m/s). The acceleration measured at the HFCOG headform was 15, 21.3, and 30.4 g, respectively. Duma et al9 measured head acceleration with football helmets instrumented with accelerometers and found mean head acceleration to be 32 g with a range of 1 to 200 g. Mihalik et al26 measured impact magnitude in collegiate football players by attaching accelerometers to football helmets. They reported a mean impact magnitude of 19.46 ± 2.29 g for all positions measured. Guskiewicz et al9 noted impacts ranging from 64 to 102 g, as measured by an instrumented helmet, on a defensive end during practice. Our results revealed that peak g averages from the 152-cm height were 122 g (front), 127 g (rear boss), and 136 g for all impact locations, with average SI values of 674 (front), 672 (rear boss), and 728 (all impacts).
The data supported our hypothesis that an accelerometer placed intraorally would measure acceleration to the head more accurately than would an accelerometer placed on the helmet. The MP fit to the headform was the same as the MP fit to athletes because it was molded to the dentition (a custom-made MP for athletes is molded and is only held in place by the fit of the MP to the dentition). The intraoral MP and headform most likely acted as a unit on impact, so their measurements were similar. Our results validate an MP molded to the dentition as a valid method of measuring head acceleration. Future research will focus on testing the MP in live subjects in a laboratory setting to measure impact acceleration to the head in different sport activities. Also, acceleration levels to the head can be assessed and compared in many different sports to examine the potential for head injury and to determine the sports in which the greatest amount of acceleration exists. It is important to be able to measure the magnitude of head impacts in helmeted and nonhelmeted sports. The measurement of head acceleration in helmeted sports is being investigated with instrumented helmets,8–10,26 but little success has been demonstrated in developing techniques to accurately measure head acceleration in nonhelmeted sports. This study demonstrates the potential of having a valid measuring device to accomplish this task.
CLINICAL RELEVANCE
With the awareness of the incidence of mild traumatic brain injury increasing, the ability to measure actual head acceleration during competition will provide medical personnel, helmet manufacturers, and researchers with invaluable information to help protect athletes more effectively. Measuring head acceleration of athletes during actual competition may greatly enhance the ability of sports medicine professionals and helmet manufacturers to protect athletes. This information would help to determine the range of acceleration levels that may cause a concussion. Our findings suggest that placement of the accelerometer on the helmet is not a valid measurement of head acceleration. The MP measurement used in this study is a more valid measure of head acceleration, because its data were comparable, highly correlated, and not significantly different from the actual acceleration the headform experienced directly. The placement of an accelerometer in an MP has the potential to allow for the direct assessment of the actual acceleration experienced by the head and not the acceleration of the helmet.
Limitations
We only measured linear acceleration and not rotational acceleration with impact. Rotational acceleration has been reported to be a cause of neuronal injury because of the shearing forces experienced by neuronal tissue. We used a single triaxial accelerometer at each location; the limitation of this method is that it measures the acceleration only at the location of the accelerometer, which may limit understanding of the acceleration of the whole head.32 The transfer of this method to the measurement of head acceleration in the field is being investigated in human subjects. Factors being addressed are wires exiting the mouth and MP fit. Further investigation into head acceleration measurement in nonhelmeted sports is needed.
Acknowledgments
We thank the staff of the Southern Impact Research Center for their hospitality and support. We would like to especially thank David McNeely for his untiring effort in working with us during this project and John Govern, PhD, for his statistical advice.
REFERENCES
- Powell JW, Barber-Foss KD. Traumatic brain injury in high school sports. JAMA. 1999;282:958–963. doi: 10.1001/jama.282.10.958. [DOI] [PubMed] [Google Scholar]
- Sosin DM, Sniezek JE, Thurman DJ. Incidence of mild and moderate brain injury in the United States, 1991. Brain Inj. 1996;10:47–54. doi: 10.1080/026990596124719. [DOI] [PubMed] [Google Scholar]
- Thurman DJ, Branche CM, Sniezek JE. The epidemiology of sports-related traumatic brain injuries in the United States: recent developments. J Head Trauma Rehabil. 1998;13:1–8. doi: 10.1097/00001199-199804000-00003. [DOI] [PubMed] [Google Scholar]
- National Collegiate Athletic Association (NCAA). NCAA Injury Surveillance System. Overland Park, KS: NCAA; 2000.
- Barth JT, Freeman JR, Broshek DK, Varney RN. Acceleration-deceleration sport-related concussion: the gravity of it all. J Athl Train. 2001;36:253–256. [PMC free article] [PubMed] [Google Scholar]
- McCrory P, Johnston KM, Mohtadi NG, Meeuwisse W. Evidence-based review of sport-related concussion: basic science. Clin J Sport Med. 2001;11:160–165. doi: 10.1097/00042752-200107000-00006. [DOI] [PubMed] [Google Scholar]
- Therrien RG, Bourassa PA. Mechanics application to sports equipment: protective helmets, hockey sticks, and jogging shoes. In: Ghista DN, ed. Human Body Dynamics: Impact, Occupational, and Athletic Aspects. Oxford, UK: Clarendon Press; 1982:498–511.
- Naunheim RS, Standeven J, Richter C, Lewis LM. Comparison of impact data in hockey, football and soccer. J Trauma. 2000;48:938–941. doi: 10.1097/00005373-200005000-00020. [DOI] [PubMed] [Google Scholar]
- Duma SM, Manoogian SJ, Bussone WR. Analysis of real-time head accelerations in collegiate football players. Clin J Sport Med. 2005;15:3–8. doi: 10.1097/00042752-200501000-00002. et al. [DOI] [PubMed] [Google Scholar]
- Guskiewicz KM, Mihalik JP, Notebaert AJ. Recurrent concussion in a collegiate football player equipped with a Head Impact Telemetry System. J Athl Train. 2005;40((suppl):):S-81. et al. [Google Scholar]
- Shewchenko N, Withnall C, Keown M, Gittens R, Dvorak J. Heading in football, part 1: development of biomechanical methods to investigate head response. Br J Sports Med. 2005;39((suppl 1)):i10–i25. doi: 10.1136/bjsm.2005.019034. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lewis LM, Naunheim R, Standeven J, Lauryssen C, Richter C, Jeffords B. Do football helmets reduce acceleration of impact in blunt head injuries? Acad Emerg Med. 2001;8:604–609. doi: 10.1111/j.1553-2712.2001.tb00171.x. [DOI] [PubMed] [Google Scholar]
- Lewis LM, Naunheim RS, Richter CJ, Standeven JW. Are helmets protective in high impact collisions? Acad Emerg Med. 2000;7:437. [Google Scholar]
- Gurdjian ES, Lissner HR, Evans FG, Patrick LM, Hardy WG. Intracranial pressure and acceleration accompanying head impacts in human cadavers. Surg Gynecol Obstet. 1961;113:185–190. [PubMed] [Google Scholar]
- National Operating Committee on Standards for Athletic Equipment (NOCSAE). Standard Drop Test Method and Equipment Used in Evaluating the Performance Characteristics of Protective Headgear. Overland Park, KS: NOCSAE; 1998. ND01-06m06.
- National Operating Committee on Standards for Athletic Equipment (NOCSAE). Equipment Calibration Procedures. Overland Park, KS: NOCSAE; 1996. ND101-00m03.
- National Operating Committee on Standards for Athletic Equipment (NOCSAE). Standard Performance Specification for Newly Manufactured Football Helmets. Overland Park, KS: NOCSAE; 1998. ND002-98m05.
- National Operating Committee on Standards for Athletic Equipment (NOCSAE). Laboratory Procedural Guide for Certifying Newly Manufactured Football Helmets. Overland Park, KS: NOCSAE; 1998. ND003-96m03.
- National Operating Committee on Standards for Athletic Equipment (NOCSAE). Standard Performance Specification for Recertified Football Helmets. Overland Park, KS: NOCSAE; 1998. ND004-96m06.
- Gadd CW. Use of a weighted-impulse criterion for estimating injury hazard. In: Proceedings of the 10th Stapp Car Crash Conference, 1966. New York, NY: Society of Automotive Engineers; 1966:164–174.
- Gurdjian ES, Hodgson VR, Hardy WG, Patrick LM, Lissner HR. Evaluation of the protective characteristics of helmets in sports. J Trauma. 1964;171:309–324. doi: 10.1097/00005373-196405000-00005. [DOI] [PubMed] [Google Scholar]
- Hutchinson J, Kaiser MJ, Hamid ML. The head injury criterion functional. Appl Math Comput. 1998;96:1–16. [Google Scholar]
- Hodgson VR. Biomechanical study of football head impacts using a human head model: a final report prepared for NOCSAE. Overland Park, KS: NOCSAE; 1973.
- Bishop PJ, Norman RW, Kozey JW. An evaluation of football helmets under impact conditions. Am J Sports Med. 1984;12:233–236. doi: 10.1177/036354658401200313. [DOI] [PubMed] [Google Scholar]
- Myers TJ, Yoganandan N, Sances A, Jr,, Pintar FA, Reinartz J, Battocletti JH. Energy absorption characteristics of football helmets under low and high rates of loading. Biomed Mater Eng. 1993;3:15–24. [PubMed] [Google Scholar]
- Mihalik JP, Guskiewicz KM, Notebaert AJ. Measurement of head impacts in Division I collegiate football players. J Athl Train. 2005;40((suppl)):S-82. et al. [Google Scholar]
- Bishop PJ, Norman RW, Pierrynowski M, Kozey J. The ice hockey helmet: how effective is it? Physician Sportsmed. 1979;7((2)):97–106. doi: 10.1080/00913847.1979.11948439. [DOI] [PubMed] [Google Scholar]
- Gurdjian ES, Roberts VL, Thomas LM. Tolerance curves of acceleration and intracranial pressure and protective index in experimental head injury. J Trauma. 1996;6:600–604. doi: 10.1097/00005373-196609000-00005. [DOI] [PubMed] [Google Scholar]
- Bishop PJ, Norman RW, Wells R, Ranney D, Sleryk B. Changes in the center of mass and moment of inertia of head form induced by a hockey helmet and face shield. Can J Appl Sport Sci. 1983;8:19–25. [PubMed] [Google Scholar]
- Bishop PJ. Dynamic response criteria for ice hockey helmet design. In: Komi P, ed. Biomechanics. Vol V-B. Baltimore, MD: University Park Press; 1976:299–305.
- Naunheim R, Ryden A, Standeven J. Does soccer headgear attenuate the impact when heading a soccer ball? Acad Emerg Med. 2003;10:85–90. doi: 10.1111/j.1553-2712.2003.tb01983.x. et al. [DOI] [PubMed] [Google Scholar]
- Crisco JJ, Chu J, Greenwald R. An algorithm for estimating acceleration magnitude and impact location using multiple nonorthogonal single-axis accelerometers. J Biomech Eng. 2004;15:849–854. doi: 10.1115/1.1824135. [DOI] [PubMed] [Google Scholar]