

Abstract
Context: Motion in the lumbar spine during certain physical activities may exceed tissue homeostasis, leading to low back pain. Previous authors have assessed sagittal motion of the lumbar spine during walking; however, limited attention has been focused on changes in spine position with walking or running on different surface gradients.
Objective: To investigate lumbar spine sagittal position during standing, walking, and running on level, uphill, and downhill surfaces.
Design: Three by three and 2 × 3 (activity by gradient) within-subjects design with repeated measures on both factors.
Setting: Motion analysis laboratory.
Patients or Other Participants: Twenty healthy women (age = 23.4 ± 2.2 years, height = 141.5 ± 7.5 cm, mass = 60.5 ± 5.9 kg) with no history of low back pain or surgery or lower extremity impairments or surgery.
Intervention(s): Subjects stood motionless, walked at 1.3 m/s, and ran at 2.9 m/s on a treadmill under 3 conditions: level, uphill at 5°, and downhill at 5°.
Main Outcome Measure(s): We measured lumbar spine position and total lumbar range of motion in the sagittal plane using an infrared motion analysis system, with markers affixed to the skin over the sacrum and thoracolumbar junction.
Results: The average lumbar spine position, for both walking and running, was smallest uphill and greatest downhill. On all 3 gradients, the sagittal range of motion (flexion-extension) was greater when running than when walking.
Conclusions: For each of the surface gradients, the average lumbar spine position was greatest during standing, at an intermediate value during running, and smallest during walking. Changes in lumbar spine position corresponding to different activities and different surface gradients are important considerations when rehabilitating patients with lumbar spine conditions.
Keywords: lumbosacral region, lordosis, kinematics
Key Points
Total lumbar spine range of motion was greater during running than walking.
Total lumbar spine range of motion was greater during running and walking downhill than during walking uphill or on a level surface.
Changes in lumbar spine motion as a function of gradient and activity must be considered in those with low back pain.
The need to understand the demands placed on the low back during physical activity has prompted authors to perform numerous biomechanical studies.1–6 The gross movement of the hips and trunk tell us little about the arthokinematics of the pelvis and lumbar vertebrae. Common activities such as walking and running, particularly on different surface gradients, may produce motion that exceeds tissue homeostasis, thereby placing these structures at risk for injury or reinjury. Lumbar spine position during normal walking and running on a level surface has been previously examined in several studies.1–6 Crosbie et al1 studied patterns of spinal motion during walking and described the pelvic motion that occurs as the lower limb is advanced. They suggested that movement of the pelvis enhances the ability of the body weight to be transferred from one lower extremity to the other during normal walking. They also found that movements of the spinal segments tended to complement movements of the pelvis (ie, maximum flexion of the lumbar spine occurs at initial foot contact, with the pelvis in a posterior tilt). During the loading response, lumbar extension occurs, accompanied by an anterior pelvic tilt, indicating that the spinal segments move in response to the motion of the lower limbs.1 In contrast, Rowe and White6 noted that minimum rather than maximum flexion of the lumbar spine occurred at initial contact and that flexion increased early in the single-support phase of the gait cycle. Such discrepancies are to be expected because Whittle and Levine4 found considerable variability in the lumbar spine position among subjects during the gait cycle.
The effects of altered walking speed on spinal motion have been reported in general terms by Crosbie et al,7 who found that increases in the range of lumbar flexion-extension and other spinal motions occurred with increases in walking speed. Crosbie et al1 stated that the lumbar and lower thoracic spinal regions need to produce compensatory motions to keep the trunk in neutral alignment with respect to the ground in order to avoid an abnormal gait. Because increased walking speed is usually accompanied by increased step length,7 we could assume that as an individual runs, greater compensatory motion of the spinal segments would be necessary as step length and speed increase. However, Novacheck8 reported very little increased motion of the pelvis in the sagittal plane with faster velocities.
Whittle and Levine4 examined the 3-dimensional movements of the lumbar spine, pelvis, and hip in walking, and Schache et al9 studied similar factors during running. These authors documented the normal kinematic patterns between the pelvis and lumbar spine during walking and running. Schache et al10 also compared over-ground and treadmill running and found that treadmill running adequately represented the typical running pattern with respect to pelvic and spinal motion.
Low back pain (LBP) in runners has not received much attention, possibly because of its relatively low incidence. In a number of surveys,11–13 LBP accounted for 5% to 19% of running injuries. Koplan et al11 reported an incidence of back pain of 8% and 9% in male and female runners, respectively, in a large cohort (n = 535). Spinal symptoms related to running occur most commonly in runners between 30 and 50 years of age and often are the result of an underlying degenerative process, the lumbar region being the most commonly affected.14 Low back pain has also been attributed to excessive lumbar spine position, muscular imbalances, leg-length differences, and excessive pronation,15 although the relationship between LBP and these variables remains controversial.
Guten16 reported an association between running and exaggerated lumbar mobility, as well as postural changes such as the development of lumbar spine lordosis with hip extension. This increased mobility may be advantageous in running, because with every step, the spine must move from a flat position to the lordotic position.14,16 In addition, flexibility of the lumbar spine enhances its shock-absorbing ability,17 which is important because as the speed of gait increases, the magnitude of the vertical force increases up to about 275% of body weight.18 Cappozzo19 reported that the total axial load on the lumbar spine during running is more than 3 times the weight of the upper body above the fifth lumbar segment.
Alexander15 suggested that the lumbar spine is responsible for supporting the entire body weight above the pelvis and that the force is greatest at the lumbosacral junction. Here, the natural lordotic curve causes much of the vertical compressive force of the body weight to become shear force, which increases the load on the intervertebral discs. In line with Alexander's description of shear force occurring at the lumbosacral junction, Guten16 portrayed the leg as a lever arm and the lumbar spine as the fulcrum in running; thus, force is transmitted horizontally. Running may also lead to LBP problems because of an exaggerated lumbar spine position due to hip extension and long stride length.15,16 Shorter runners may be at greater risk for injury because they tend to have relatively longer strides.15,16 Guten16 attributed the backward thrust of the leg during running to strong lumbar muscles tilting the pelvis. As the pelvis tilts forward maximally, lumbar spine extension also increases to a maximum.20,21
Although several authors have reported sagittal motion of the lumbar spine during walking, change in lumbar spine position during standing, walking, and running on different grades has received little attention. Therefore, our purpose was to measure lumbar spine position in the sagittal plane during standing, walking, and running on level, uphill, and downhill surfaces. Understanding the amount of motion through which the spine moves will help us to develop return-to-activity protocols and prevent injury based on how much motion is desirable and which lumbar position(s) the athlete should avoid. Our hypothesis was that lumbar spine position would decrease during uphill walking and running, as compared with level-surface lumbar spine position, and that the opposite would occur when the runner is walking and running downhill. We also hypothesized that a greater range of lumbar spine motion would occur during running, as compared with walking, on the same gradient.
METHODS
Subjects
Because of the well-known sex differences in pelvic structure, we decided to conduct the present study on a single sex. We selected 20 women (age = 23.4 ± 2.2 years, height = 141.5 ± 7.5 cm, mass = 60.5 ± 5.9 kg) to participate in this study. The subjects were all volunteers from the general student population at the university who signed informed consent forms. All subjects were recreational runners (averaging 15.1 mile/wk [24.3 km/wk]) and met the following inclusion criteria: they (1) were in good health, (2) had no history of LBP or surgery, and (3) had no history of lower extremity impairments or surgery. Our study was approved by the university's institutional review board.
Instrumentation
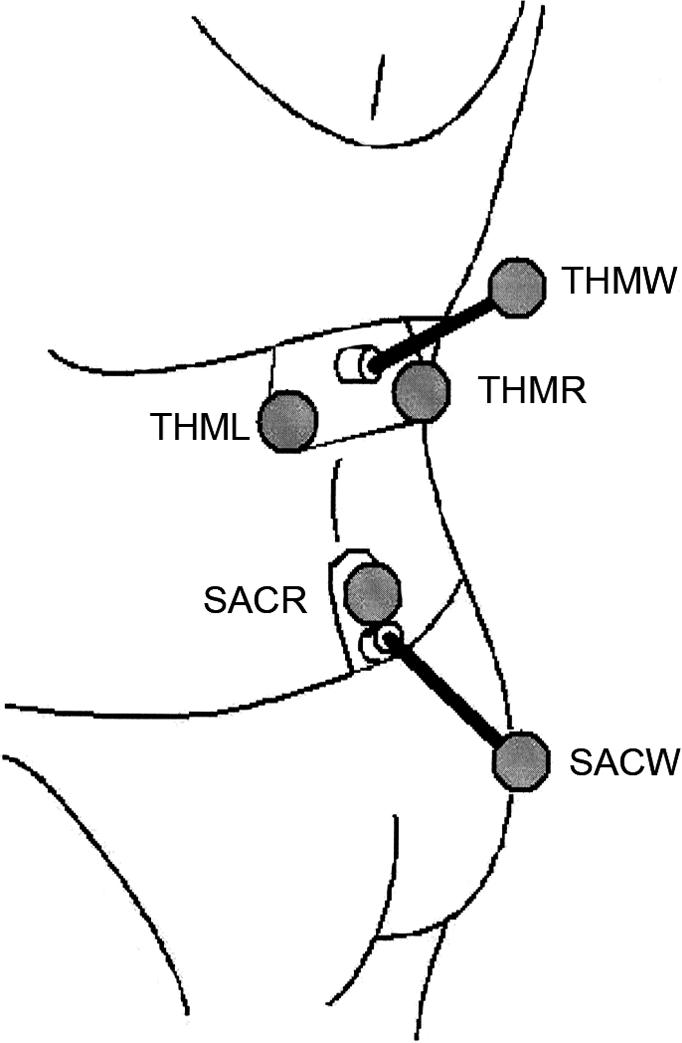
We quantified lumbar position using a 3-dimensional kinematic system (Vicon; Oxford Metrics Ltd, Oxford, UK).4 Reliability of the kinematic system has been established for measurement of both pelvic tilt and lumbar spine position.21,22 Six infrared-sensitive, 50-Hz cameras with infrared strobes were located around the measurement area. Four 25-mm–diameter spherical retroreflective markers were affixed to the subjects' skin with double-sided adhesive tape22 over both anterior superior iliac spines and both lateral malleoli. We also affixed 2 measurement rigs to the skin, one over the sacrum and one over the upper lumbar spine. Each consisted of a flat plastic base plate covering 2 spinal levels (Figure 1).21 The sacral rig consisted of one marker midway between the posterior superior iliac spines at S2 and one marker on the end of a 100-mm aluminum wand extending inferiorly and posteriorly from the plate's center.21,22 The thoracic rig consisted of 2 markers, one on each side of the spinous process of T12 and a third marker on the end of a 100-mm wand pointing posteriorly and superiorly.21,22 The wands were attached to the rigs at a fixed angle.
Figure 1. Rigs used to make measurements. The sacral rig has one marker over S2 (SACR) and one on a wand (SACW). The thoracic rig has markers to the left (THML) and right (THMR) of the T12 spinous process and one marker on a wand (THMW).
For each rig, we conducted a static trial in which the angle was measured between the base plate surface and the line joining the markers on the rig (the thoracic and sacral wand angles).21 This measurement was achieved by performing data capture with the rigs on a horizontal surface, skin surface down, in the same relative positions they would occupy when placed on the subjects. The thoracic and sacral wand angles were used to compute the orientation of the skin surfaces beneath the thoracic and sacral rigs during the walking and running trials.21 We defined the lumbar spine position as the difference in the sagittal plane between the angles of the skin surfaces in the thoracic and sacral areas, as described by Levine and Whittle (Figure 2).21 The markers on the lateral malleoli were used for identifying events in the gait cycle but were not required to collect data on pelvic or lumbar movement. We used a computer software program (RData2; Motion Lab Systems, Baton Rouge, LA) to extract 3-dimensional coordinates from the kinematic system data files for transfer to a spreadsheet (Excel version 2003; Microsoft Corp, Redmond, WA). Calculation of the lumbar spine position in the sagittal plane was performed using the method of Whittle and Levine,4 as later modified by Whittle.23
Figure 2. Lumbar spine position is defined as the angle in the sagittal plane between the skin surface over the T12 spinous process and the sacrum at S2.

Procedures
The subjects wore either a 2-piece bathing suit or shorts and a sports bra, thereby exposing the necessary bony landmarks, and they wore shoes suitable for running. We conducted standing, walking, and running trials on a treadmill at 3 gradients: level, 5° uphill, and 5° downhill, as measured using an inclinometer. Data collection was initiated 60 seconds or more after the start of activity; the subjects were unaware that data collection had begun. We collected 1 trial at each speed with multiple gait cycles. Data on 4 complete gait cycles in each combination of speed and gradient were collected for each trial. Treadmill speed was set at 1.3 m/s (2.9 mph) in the walking trials and at 2.9 m/s (6.5 mph) in the running trials. Subjects walked or ran between 90 and 120 seconds per trial. Between trials, subjects were permitted to relax and walk around the room for 1 minute.
Statistical Analysis
We averaged 4 gait cycles under each condition for analysis on each subject. Mean lumbar spine position and total lumbar range of motion (ROM) (motion between maximum flexion and maximum extension) were measured during 3 activities on 3 gradients. Our data were analyzed by computing separate, repeated-measures analysis of variance (ANOVA) procedures. Specifically, 3 × 3 (activity × gradient) and 2 × 3 (activity × gradient) repeated-measures ANOVAs were calculated for the mean lumbar spine position and the mean lumbar ROM, respectively. The standing condition was not utilized for the ROM analysis, thereby warranting a 2 × 3 ANOVA (2 activities, 3 grades) for lumbar ROM. A significant activity × gradient interaction effect was interpreted as evidence of a significant difference in the amount of lumbar position change caused by a given combination of activity type and surface gradient. We used the Bonferroni correction24 for multiple comparisons to adjust the chosen alpha level of .05 for the 2 activity × gradient analyses, which established .025 as the adjusted alpha level for determination of statistical significance. The Mauchley test24 was performed to ensure that the ANOVA assumption of homogeneity of variance was not violated for the evaluation of the activity × gradient interaction effect. We also used pairwise comparisons for follow-up analyses to identify specific significant differences among the conditions. All statistical analyses were performed with SPSS software (version 11.5; SPSS Inc, Chicago, IL).
RESULTS
Mean lumbar spine position and total lumbar ROM when standing, walking, and running on all 3 gradients (level, uphill, and downhill) are illustrated in Figure 3. Table 1 includes the means and SDs for lumbar spine position (standing, walking, and running) and for the total lumbar ROM (walking and running). Because the assumption of compound symmetry was not met, we report univariate results with a Geisser-Greenhouse epsilon correction.24 Mean lumbar position showed a significant activity × gradient interaction (F2.30,34.30 = 14.873, P < .001). The power to reject the null hypothesis of no interaction effect for mean lumbar position was exceptionally strong (1 − β = 1.00), and the proportion of total variance attributable to the activity × gradient interaction effect was large (η2 = .498). Tables 2 and 3 report the pairwise activity and gradient comparisons for mean lumbar position and total ROM, respectively. The gradients are pooled for pairwise comparisons for activity, and the activities are pooled for pairwise comparisons for gradient. For each of the 3 gradients, our findings indicate that lumbar spine position was greater while standing than during either walking or running and was greater while running than while walking (Tables 1 and 2; Figure 3). Standing lumbar spine position (Table 1; Figure 3) was not significantly affected by the gradient. However, for both walking and running, we found statistically significant differences between each pair of gradients, lumbar spine position being greatest downhill and smallest uphill.
Figure 3. Range-of-motion and mean values across gait cycle for lumbar spine position during standing, walking, and running on downhill, level, and uphill surfaces. A larger angle represents extension of the lumbar spine. The upper and lower margins of each box represent the maximum and minimum values, and the line across the box indicates the mean.

Table 1. Lumbar Spine Position and Total Lumbar Range of Motion When Standing, Walking, and Running on Each Gradient (°).

Table 2. Pairwise Comparisons for Mean Lumbar Spine Position.

Table 3. Pairwise Comparisons for Total Lumbar Range of Motion.

Total lumbar ROM demonstrated no significant activity × gradient interaction (F1.43,27.13 = 0.494, P = .553). We found a significant main effect for activity (F1,19 = 86.562, P < .001) and for gradient (F1.34,25.54 = 6.294, P = .012). A large proportion of total variance was attributable to the type of activity (η2 = .82), and a much smaller proportion of total variance was attributable to the surface gradient (η2 = .113). The total lumbar ROM during the gait cycle (Table 1; Figure 3) was significantly greater (P < .001) when the subject was running than when she was walking for all 3 gradients. The total lumbar ROM showed no significant difference between the level and uphill gradients but was significantly greater for both walking and running downhill than for level or uphill gradients (Table 1; Figure 3). Figure 4 shows the average pattern of lumbar spine position across the gait cycle for walking and running on a level surface. The curves for downhill and uphill walking and running were similar to those for level walking but displaced 3° to 4° in the direction of increased lumbar spine position (downhill) and decreased lumbar spine position (uphill). Furthermore, we found that the minimum and maximum values tended to occur at similar points in the gait cycles as in previous studies.4,7,9,22
Figure 4. Lumbar spine position while subjects were walking (solid line) and running (dashed line) on a level surface based on average values for all subjects. A larger angle represents extension of the lumbar spine.

DISCUSSION
Although past researchers stated that increased lumbar mobility associated with running is advantageous and that flexibility of the lumbar spine enhances its shock-absorbing ability,14,16,17 excessive increases and decreases in lumbar spine position have the potential to be detrimental to the spine. We demonstrated that uphill walking and running produced an overall decrease in lumbar spine position and that downhill walking and running produced an overall increase. The lumbar spine position and total lumbar ROM values found in this study are similar to the values previously reported on healthy nonrunners.21 The mean lumbar angles when subjects were walking and running downhill were significantly greater than when subjects were walking and running under level or uphill conditions (Table 1; Figure 3). This indicates that the angle of the pelvis adapts to the uphill or downhill gradient of the surface on which one is running. This would be expected if the pelvis follows the orientation of the lower extremities, which are adapted to a sloping surface. The greater lumbar angles may also be partially explained by positional changes superior to the lumbar spine (eg, head, extremity, thorax postures) and/ or in combination with changes in pelvic and lower extremity position.
Pairwise comparisons for lumbar spine position demonstrated statistically significant differences among all gradient pairs for both walking and running. This indicates a predictable change in lumbar spine position among level, uphill, and downhill conditions for walking and running. Walking and running, however, were not significantly different, with running producing marginally greater angles than walking (Tables 1 and 2), which is consistent with Novacheck's8 finding of little increased motion in the lumbar spine in the sagittal plane with faster velocities. This result may indicate that any potentially adverse effect from one activity may be attributable to other factors, such as flight, cadence, lower extremity position, or step length.15,16
For total lumbar ROM, we found that running produced a significantly greater excursion than walking (Table 1) and that downhill running used significantly more total lumbar motion than uphill or level conditions (P < .05) (Table 3). Our results support those of Crosbie et al,7 who found that increases in the range of lumbar flexion-extension and other spinal motions occurred with increases in walking speed. For all surface gradients, the range of lordotic excursion was significantly greater in running than in walking (Table 1). This increase in lordotic excursion in running was expected, because the combination of a backward thrust of the leg and anterior tilting of the pelvis increases lumbar spine position.16,20 The greatest range of lumbar spine position for walking trials occurred during downhill conditions; this range was significantly greater (P < .001) than for level or uphill conditions (Table 1). Similar results were found in the running trials. Recently, Gottschall and Kram25 investigated ground reaction forces during downhill and uphill running in 5 male and 5 female subjects. The subjects ran at 3 m/s on a treadmill at level condition and at gradients of 3°, 6°, and 9°. Downhill running significantly increased impact force peaks compared with level running. The increase in lumbar spine motion we found during downhill running may be advantageous in dissipating the added ground reaction forces associated with downhill running. The anterior convexity and mobility17 of the lumbar spine serve to cushion compressive forces along with the intervertebral discs.26 Because a relationship between lumbar lordosis and LBP has not been clearly established26 and because the incidence of LBP in runners in relatively low, perhaps the increase in lumbar spine motion found with downhill running in our subjects has a protective role.
Clinical Relevance
In this study, we have demonstrated that alterations in the lumbar spine occur depending on the gradient of the running surface and could be a source of LBP during running. Specifically, our findings demonstrated a link between gradient and lumbar position in our sample of healthy female participants. This linkage may be related to pain, although the evidence from this study does not directly support this relationship. Therefore, if excessive lordosis is a concern, we recommend against prolonged standing (versus walking or running) and prolonged downhill walking or running (level or uphill may be easier). Finally, if excessive lordosis or lumbar ROM is a concern, we recommend avoiding running (walking is easier). Runners who have been diagnosed with a condition made worse by increased lumbar lordosis (eg, spondylolysis, spondylolisthesis, spinal stenosis, or foraminal stenosis)27 may want to avoid excessive downhill running. Conversely, individuals with disc conditions, such as a herniated nucleus pulposus, may benefit from avoiding excessive uphill running or hill workouts, simply because of the changes in lumbar spine position that may theoretically exacerbate symptoms. Although this link needs to be investigated more extensively, clinicians should consider the implications of the biomechanics of uphill and downhill running when working with athletes. For example, a football lineman diagnosed with spondylolisthesis may note an increase in his symptoms with hill workouts. Flexibility and muscle tightness, as well as muscle imbalances, may also play roles in the exercise and training prescription. An athlete with tight hip flexors may run with a greater lumbar position, especially during downhill running. This may add excessive shear stresses to the lumbosacral region. Therefore, clinicians should pay close attention to muscle flexibility and muscle imbalances, particularly in the hip, pelvis, and lumbar region, when examining runners with LBP. Another interesting finding was that the maximum amount of lumbar position was in standing, and walking and running in all 3 conditions decreased the lumbar curve. This result may also have implications for exercise prescriptions.
Summary
Further study is warranted to improve our understanding of lumbar spinal motion during walking and running. We fully expected to see significant differences in lumbar spine position among conditions (level, uphill, and downhill) in walking and running trials, as well as between walking and running trials conducted under the same condition. Although the overall pattern was consistent with our expectations (Figure 3), we did not find significant differences among all conditions. This result appeared to be due to an unexpectedly high variability among subjects. This variability should be investigated in future studies to determine how much of the variance can be explained by individual strategies. The uphill and downhill conditions were conducted at +5° and −5° grades, respectively. Greater differences may be found if higher grades are used in future research, although we chose 5° as a reasonable grade for persons to run without overexertion. Future authors should investigate the kinematics of the thoracic spine, hip, and knee, as well as frontal-plane and transverse-plane kinematics, during various conditions of running in both sexes. In addition, an intervention study designed to change the lumbar spine posture and measure the resultant effect on lumbar spine position and total lumbar ROM would also be of interest.
REFERENCES
- Crosbie J, Vachalathiti R, Smith R. Patterns of spinal motion during walking. Gait Posture. 1997;5:6–12. [Google Scholar]
- Taylor NF, Goldie PA, Evans OM. Angular movements of the pelvis and lumbar spine during self-selected and slow walking speeds. Gait Posture. 1999;9:88–94. doi: 10.1016/s0966-6362(99)00004-1. [DOI] [PubMed] [Google Scholar]
- Thurston AJ, Harris JD. Normal kinematics of the lumbar spine and pelvis. Spine. 1983;8:199–205. doi: 10.1097/00007632-198303000-00012. [DOI] [PubMed] [Google Scholar]
- Whittle MW, Levine D. Three-dimensional relationships between the movements of the pelvis and lumbar spine during normal gait. Hum Mov Sci. 1999;18:681–692. [Google Scholar]
- Schache AG, Bennell KL, Blanch PD, Wrigley TV. The coordinated movement of the lumbo-pelvic-hip complex during running: a literature review. Gait Posture. 1999;10:30–47. doi: 10.1016/s0966-6362(99)00025-9. [DOI] [PubMed] [Google Scholar]
- Rowe PJ, White M. Three dimensional, lumbar spinal kinematics during gait, following mild musculo-skeletal low back pain in nurses. Gait Posture. 1996;4:242–251. [Google Scholar]
- Crosbie J, Vachalathiti R, Smith R. Age, gender, and speed effects on spinal kinematics during walking. Gait Posture. 1997;5:13–20. [Google Scholar]
- Novacheck TF. The biomechanics of running. Gait Posture. 1998;7:77–95. doi: 10.1016/s0966-6362(97)00038-6. [DOI] [PubMed] [Google Scholar]
- Schache AG, Blanch P, Rath D, Wrigley T, Bennell K. Three-dimensional angular kinematics of the lumbar spine and pelvis during running. Hum Mov Sci. 2002;21:273–293. doi: 10.1016/s0167-9457(02)00080-5. [DOI] [PubMed] [Google Scholar]
- Schache AG, Blanch PD, Rath DA, Wrigley TV, Starr R, Bennell KL. A comparison of overground and treadmill running for measuring the three-dimensional kinematics of the lumbo-pelvic-hip complex. Clin Biomech (Bristol, Avon) 2001;16:667–680. doi: 10.1016/s0268-0033(01)00061-4. [DOI] [PubMed] [Google Scholar]
- Koplan JP, Rothenberg RB, Jones EL. The natural history of exercise: a 10-year follow-up of a cohort of runners. Med Sci Sport Exerc. 1995;27:1180–1184. [PubMed] [Google Scholar]
- Wen DY, Puffer JC, Schmalzried TP. Lower extremity alignment and risk of overuse injuries in runners. Med Sci Sport Exerc. 1997;29:1291–1298. doi: 10.1097/00005768-199710000-00003. [DOI] [PubMed] [Google Scholar]
- Rendall EO, Mohtadi GH. Survey of competitive distance runners in Alberta: satisfaction with health care services with respect to running injuries. Clin J Sport Med. 1997;7:104–112. doi: 10.1097/00042752-199704000-00006. [DOI] [PubMed] [Google Scholar]
- Jackson DW. Spine problems in the runner. In: D'Ambrosia RD, Drez D, eds. Prevention and Treatment of Running Injuries. 2nd ed. Thorofare, NJ: Slack Inc; 1989:83–96.
- Alexander MJL. Biomechanical aspects of lumbar spine injuries in athletes: a review. Can J Appl Sport Sci. 1985;10:1–20. [PubMed] [Google Scholar]
- Guten G. Herniated lumbar disk associated with running: a review of 10 cases. Am J Sports Med. 1981;9:155–159. doi: 10.1177/036354658100900305. [DOI] [PubMed] [Google Scholar]
- Deusinger RH. Biomechanical considerations for clinical application in athletes with low back pain. Clin Sports Med. 1989;8:703–715. [PubMed] [Google Scholar]
- Mann RA, Baxter DE, Lutter LD. Running symposium. Foot Ankle. 1981;1:190–224. doi: 10.1177/107110078100100402. [DOI] [PubMed] [Google Scholar]
- Cappozzo A. Force actions in the human trunk during running. J Sports Med Phys Fitness. 1983;23:14–22. [PubMed] [Google Scholar]
- Liemohn W. Exercise and arthritis: exercise and the back. Rheum Dis Clin North Am. 1990;16:945–970. [PubMed] [Google Scholar]
- Levine D, Whittle MW. The effects of pelvic movement on lumbar lordosis in the standing position. J Orthop Sports Phys Ther. 1996;24:130–135. doi: 10.2519/jospt.1996.24.3.130. [DOI] [PubMed] [Google Scholar]
- Whittle MW, Levine D. Measurement of lumbar lordosis as a component of clinical gait analysis. Gait Posture. 1997;5:101–107. [Google Scholar]
- Whittle MW. Reduction of crosstalk in the measurement of spinal motion. Gait Posture. 2003;18((suppl 2)):S10–S11. [Google Scholar]
- Huck SW, Cormier WH. Reading Statistics and Research. 2nd ed. New York, NY: Harper Collins College Publishing; 1996:430–456.
- Gottschall JS, Kram R. Ground reaction forces during downhill and uphill running. J Biomech. 2005;38:445–452. doi: 10.1016/j.jbiomech.2004.04.023. [DOI] [PubMed] [Google Scholar]
- Hansson T, Bigos S, Beecher P, Wortley M. The lumbar lordosis in acute and chronic low-back pain. Spine. 1985;10:154–155. doi: 10.1097/00007632-198503000-00008. [DOI] [PubMed] [Google Scholar]
- Cole AJ, Herring SA, Stratton SA. Spine injuries in runners: a functional approach. J Back Musculoskel Rehabil. 1995;5:317. doi: 10.3233/BMR-1995-5408. et al. [DOI] [PubMed] [Google Scholar]