


The importance of providing care for children with low vision is recognised by many initiatives, such as VISION 2020, the 2004 Oslo Workshop on Low Vision,1 and the United Nation's global campaign, Education for All.
In 1992, the World Health Organization (WHO) published a working definition of low vision2: "A person with low vision is one who has impairment of visual functioning even after treatment and/or standard refractive correction, and has a visual acuity of less than 6/18 to light perception, or a visual field of less than 10 degrees from the point of fixation, but who uses, or is potentially able to use, vision for the planning and/or execution of a task for which vision is essential."
Functionally, low vision is characterised by irreversible visual loss and a reduced ability to perform many daily activities, such as recognising people in the street, reading blackboards, writing at the same speed as peers, and playing with friends.
Many children with low vision can perform better than their parents or carers expect and have the same quality of life as any other child, provided that their treatment follows these steps, and in this order:
Examination to establish the cause of visual loss
Surgical interventions where appropriate (such as cataract surgery)
Assessment of the child's various visual functions (distance vision, near vision, contrast sensitivity, and visual field)
Accurate refraction and provision of spectacles
Assessment for and prescription of low vision devices, such as magnifiers
Suggestions for non-optical low vision devices such as reading stands or reading slits
Educational support and training in the use of low vision devices (with follow-up).
Comprehensive care: an ideal
Care for children with low vision involves diverse groups, such as eye hospitals, schools, and community programmes. It should be provided in a structured and integrated way, known as comprehensive care.
A comprehensive system of care for people with low vision has clinical, educational, and social components. It ideally starts by locating people with visual problems and referring them to eye care or clinical low vision services. This is not always straightforward: differences exist between genders in access to care. A retrospective study of low vision programmes undertaken by the author in Asia3 showed that girls have poorer access to low vision care than boys. Girls may therefore need to be approached directly, and not only indirectly via community leaders or schools/school teachers.
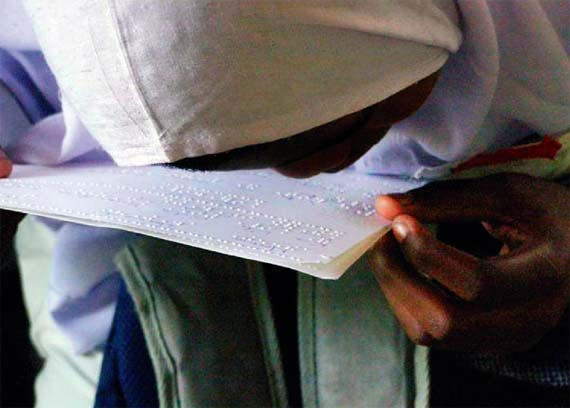
Some children with low vision are taught to read Braille unnecessarily. This child is clearly able to see the Braille dots on the page and, with refraction and/or the provision of low vision devices, should be able to read normal print. TANZANIA
Once children with low vision are identified, professionals in eye units can provide the clinical components of low vision care. They provide a diagnosis, treat acute problems, perform surgery, assess the most relevant visual functions (for instance distance vision, near vision, contrast sensitivity, and visual field), and prescribe distance glasses and/or low vision devices.
Regular follow-up visits to clinical services are very important, as the visual needs of children can change rapidly (e.g. the size of the text used in school books gets smaller as they progress through school).
Social and educational care
The social and educational components of care for children with low vision, such as training and counselling others in their environment, are often overlooked by clinical staff. This can include such diverse activities as informing peers of the visual abilities of their classmate, convincing the head of a pre-school to include a child with low vision, and teaching parents activities which can improve their baby's visual skills (such as fixation and tracking).
Educational care for children with low vision includes training children directly in the effective use of their best vision. This can involve their learning to write at closer distance, to use magnifying devices, or to use creative strategies to determine what is written on a blackboard (such as asking a child seated nearby to read aloud while the teacher writes). This training is important, as it enables children to attend local schools. Itinerant teacher programmes (see page 26) are one way of achieving many of these social and educational components of care for children with low vision.
Responsibility and co-ordination
A major obstacle to the provision of low vision services is a lack of co-ordination between eye care services and education or rehabilitation services. Each believes that the other will arrange for children to come for an eye examination and/or clinical low vision care or ensure that they obtain the surgery and/or spectacles needed.
Experience teaches that, in most cases, it is vital for staff in eye units to ensure that children with low vision are treated and managed appropriately. In situations where the eye care service provider is unable to do this, education programmes must take responsibility.
Caregivers, (special) schools, and community-based rehabilitation programmes often give cost as a reason for a child not receiving the clinical components of low vision care. However, transport costs, hospital fees, and the cost of a pair of glasses compare well to the long-term costs of interventions, such as enlarging print using photocopiers, the use of Braille, and education in a special school, for children who may not actually need them.
The importance of refraction
The importance of accurate refraction is illustrated in the study of low vision programmes undertaken by the author in Asia.3 Among the children aged 4–15 years enrolled in these programmes, more than two-thirds could achieve a distance visual acuity of 6/60 or better after receiving the correct spectacles. For many children, this level of vision is sufficient to allow them to read a blackboard from the front row in a classroom; these children generally only require minimal additional support. However, only 36% of the children in the study already had spectacles when they presented, and half of those needed a new pair.
A total of 75% of the children examined achieved a best corrected near vision of 1.25M (N10) or better, and an additional 18% could read a large print size of 2–2.5M (N16–N20) after refraction and/or magnification. These children thus had sufficient near vision to read the print used in school books (sometimes with some assistance). None of them needed to learn Braille (although some had already been taught it), and they gained the ability to attend local mainstream schools with their fully sighted peers.
This study illustrates that, even in the absence of a special clinical service dedicated to low vision, any eye unit can help many children with low vision, as long as it is capable of providing accurate refraction services.
It is important to recognise that any improvement in distance visual acuity for a child with low vision can make a big difference to his or her life; it can also improve near vision. This is particularly true for children with hyperopia, aphakia, or nystagmus. When providing low vision care for children, it is therefore vital to consider both distance and near vision.
The use of magnifying devices can be important for children whose near vision, after refraction, still remains insufficient to read print of the size used in their school books (children should be asked to bring their school books to the low vision clinic). Such devices are not necessarily expensive: in the 2005 study, 83% of the magnifying devices were locally produced and cost, on average, US $5 (rangingfrom US $0.5 to US $10).
Another lesson learnt from the study is that interventions should not be provided free of charge. When parents are charged according to their ability to pay they tend to be more motivated and to value the services. This requires co-operation between all service providers.
In conclusion, eye care providers, community workers, and teachers should firstly direct their efforts towards organising access to eye care, then towards providing surgical and optical interventions, and lastly towards determining what educational support is needed by a child with low vision.
‘It is vital to consider both distance and near vision’
References
- 1.Toward a reduction in the global impact of low vision. Report on an October 2004 meeting in Oslo. Published by The International Society for Low-vision Research and Rehabilitation. New York, March 2005.
- 2.Bangkok: 1992. WHO. Managementof low vision in children. [Google Scholar]
- 3.Van Dijk K. Unpublished retrospective study of low vision programmes in Asia, 2005, which analysed data extracted from standardised clinical records of 1,823 children, aged from 0 to 15 years, attending six low vision programmes in India, Indonesia, and Nepal in 2002 and 2003.