

Abstract
Individuals with left-hemisphere damage often have concomitant impairment of spoken and written language. Whereas some treatment studies have shown that reading paired with spoken naming can benefit both language modalities, little systematic research has been directed toward the treatment of spelling combined with spoken naming. The purpose of this study was to examine the therapeutic effect of pairing a lexical spelling treatment referred to as Copy and Recall Treatment (CART) with verbal repetition of target words. This approach (CART + Repetition) was compared with treatment using verbal repetition without the inclusion of orthographic training (Repetition Only). Two individuals with moderate aphasia and severe impairment of spelling participated in the study using a multiple baseline design across stimulus sets and treatment conditions. Both participants improved spelling of targeted words as well as spoken naming of those items, but improvement in spoken naming was marked for one individual in the CART + Repetition condition, while the other participant made smaller gains in spoken than written naming irrespective of treatment condition. Consideration of the participant profiles suggested that CART + Repetition provides greater benefit when there is some residual phonological ability and the treatment serves to stimulate links between orthography and phonology.
Keywords: Aphasia, Agraphia, Anomia, Language, Stroke, Rehabilitation
INTRODUCTION
Lexical retrieval difficulties are pervasive in individuals with aphasia, typically affecting written as well as spoken language. The underlying cause of naming impairment may be damage to semantics, phonology, or orthography—or the links among these central components of language processing that are depicted in Figure 1. Treatments for lexical retrieval may be variously directed toward semantic knowledge and lexical–semantic relations (e.g., Boyle, 2004; Kiran & Thompson, 2003), phonological processing and speech production (e.g., Franklin et al., 2002; Hillis & Caramazza, 1994; Miceli et al., 1996), or orthographic representations and writing (e.g., Aliminosa et al., 1993; Beeson et al., 2003a; Robson et al., 2001). Behavioral treatments also may stimulate interactive use of residual knowledge across semantic, phonologic, and orthographic domains. For example, treatments involving written word-to-picture matching have been shown to result in improved spoken naming (Best & Nickels, 2000; Marshall et al., 1990; Nickels & Best, 1996). In some cases, written naming abilities are better preserved than spoken naming so that orthographic knowledge may serve to cue retrieval of phonological word forms (Bastiaanse et al., 1996; Nickels, 1992). Orthography also can serve to cue phonology via sublexical grapheme–phoneme correspondences. In other words, the sounding out of graphemes can assist in the retrieval of phonological word forms when such skills are preserved or retrained. Several treatment studies have shown that the ability to write or type a word (or first letter of the word) may prompt self-cueing for phonological production (Bruce & Howard, 1987; Holland, 1998).
Fig. 1.
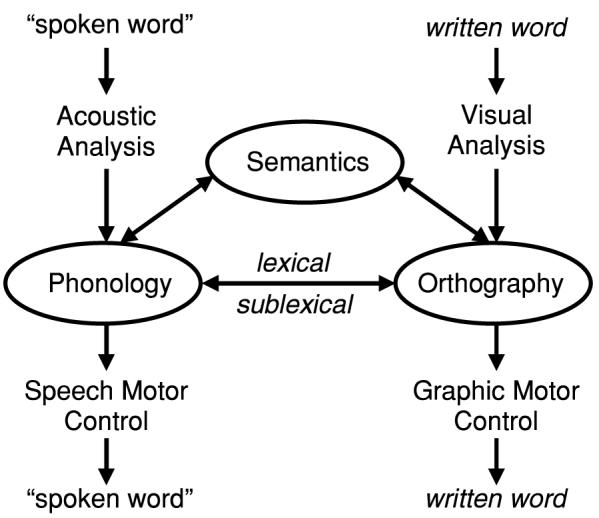
A cognitive model of language depicting interactive processing of semantic, phonologic, and orthographic information for single words.
In a series of writing treatment studies directed toward strengthening specific orthographic representations in individuals with aphasia of varying severity levels, we observed that some participants orally repeated the target words to themselves during the writing-to-dictation tasks (Beeson et al., 2002; Beeson et al., 2003a; Clausen & Beeson, 2003). Although the focus of this Copy and Recall Treatment (CART) was on written naming, anecdotal reports indicated that several participants improved oral naming over the course of treatment. Based on these observations, we suspected that pairing writing treatment with repeated spoken naming practice might provide a potent and efficient treatment affecting both output modalities.
A review of the treatment literature yielded limited evidence specific to combining spelling treatment with spoken repetition, but several studies provided relevant findings. Hillis (1989) implemented a cueing hierarchy for written naming that included the opportunity for spoken naming of target items. The treatment resulted in improved written naming in the two participants, with concomitant improvement in spoken naming in the participant who appeared to have a central semantic impairment. Drew and Thompson (1999) contrasted treatments in which auditory comprehension tasks were performed with and without repetition of target words. In the four participants studied, they found greater improvement in spoken naming when the lexical–semantic and phonological tasks were combined. In a single-case treatment study, DeDe et al. (2003) implemented a cueing hierarchy that included written naming (or copying of a written model) and spoken naming (or spoken repetition) along with tactile cueing for articulatory placement of initial phonemes. Although phonological self-cueing was the intended focus of the treatment, they concluded that the stimulation from written naming appeared to be “more critical to the observed gains in verbal naming than the tactile cueing” (p. 477). A more direct examination of treatment combining spoken and written word stimulation was implemented by Sugishita and colleagues with 22 native speakers of Japanese who had aphasia subsequent to cerebrovascular pathology (Sugishita et al., 1993). Treatment involved repeated copying of kana phonograms (hiragana) paired with oral repetition of the words. They reported significantly improved spelling in approximately half the participants and improved spoken naming in a subset of those participants. Taken together, these studies support the notion that treatment combining written spelling with spoken repetition has potential therapeutic value.
From a cognitive perspective, interactive models of lexical processing suggest that orthography receives converging input from semantics and phonology (see Figure 1), so that spelling is typically accessed via both types of linguistic codes (Ellis, 1993; Margolin, 1984; Rapcsak & Beeson, 2002). The neural substrates of these component cognitive processes await confirmation, but lesion-deficit studies and functional neuroimaging research suggest that spelling depends upon the dynamic interaction of distributed neural systems in the language-dominant hemisphere (for review, see Rapcsak & Beeson, 2002). In brief, semantic processing is thought to engage anterior and inferolateral temporal regions (BA 38, 20, 21) as well as inferior prefrontal cortex (BA 47), and the angular gyrus (BA 39; Binder & Price, 2001; Mummery et al., 2000; Vandenberghe et al., 1996). The phonological codes involved in spelling rely on a network of perisylvian cortical regions, including Broca's area, Wernicke's area, the supramarginal gyrus, and insula (Alexander et al., 1992; Fiez, 1997; Omura et al., 2004; Roeltgen et al., 1983). Orthographic knowledge of lexical representations for reading and spelling is thought to engage a critical region within temporo-occipital cortex (BA 37), sometimes referred to as the visual word form area (Beeson et al., 2003b; Cohen & Dehaene, 2004; Nakamura et al., 2002; Rapcsak & Beeson, 2004). Thus under normal circumstances, spelling engages both perisylvian and extrasylvian cortical regions.
Cortical damage can variously disrupt the cognitive processes that support spoken and written language. Whereas some individuals have greater preservation of spoken than written language, in other cases, orthographic lexical forms may be retrieved without access to corresponding phonological representations (Beeson, 1999; Rapp et al., 1997; Tainturier & Rapp, 2001). For this treatment study, our objective was to engage both phonological and orthographic processing of lexical items, with the expectation that concurrent stimulation of spoken and written word forms would have a greater effect than treatment directed toward the spoken word alone. To do so, a single-subject multiple baseline design was implemented with two individuals with aphasia of moderate severity, and their responses to two treatment approaches were examined. The first treatment paired repeated copying of written words using Copy and Recall Treatment with repetition of a spoken model; it was referred to as CART + Repetition. The goal was to improve both written and oral naming of the targeted words. The comparison treatment used repetition of a spoken model to improve oral naming of target words (Repetition Only). This exploration of the therapeutic effect of the CART + Repetition protocol was considered a Phase 1 study relative to the rubric for aphasia treatment research described by Robey and Schultz (1998). It was expected to provide insight regarding the value of promoting interaction between orthographic and phonological representations in the remediation of lexical retrieval impairments.
METHODS
Participants
Two individuals with acquired aphasia resulting from vascular damage were participants in this study (see Table 1). They both had chronic aphasia of moderate severity and expressed a desire to improve written and spoken language abilities. Informed consent was obtained for participation in this study, and the data reported here were acquired in compliance with the University of Arizona Human Subjects Protection Program.
Table 1.
Participant characteristics
| Participant |
||
|---|---|---|
| Characteristic | NEM | EMF |
| Sex | M | F |
| Age | 60 | 72 |
| Education (years) | 7 | 14 |
| Handedness (pre/post stroke) | L/L | R/R |
| Time post onset (months) | 67 | 61 |
| WAB Aphasia Quotient | 62.9 | 64.2 |
| Aphasia type | Conduction | Broca's → Anomic |
Note. WAB = Western Aphasia Battery.
Pre- and Posttreatment Assessment
Before the initiation of treatment, several tests were used to examine the nature of the language impairment. The Western Aphasia Battery (WAB; Kertesz, 1982) was administered to provide an overall profile of receptive and expressive language abilities. Semantic processing was assessed using the picture version of the Pyramids and Palm Trees Test (Howard & Patterson, 1992). This test requires the participant to decide which of two line drawings is more closely related to a target picture. The Raven's Coloured Progressive Matrices (Raven, 1976) was administered to determine the status of nonverbal visual problem solving.
Selected subtests from the Psycholinguistic Assessment of Language Processing in Aphasia (PALPA; Kay et al., 1992) were administered to explore spoken and written processing of single words. Auditory comprehension was assessed using a spoken word-to-picture matching task (PALPA 47), while reading was examined with an analogous test using the same 40 stimuli for a written word-to-picture matching task (PALPA 48). A written lexical decision task (PALPA 25) with 60 real words and 60 nonwords was used to assess visual word recognition. Assessment of repetition, oral naming, writing to dictation, and written naming was undertaken both before and after treatment on a common set of 40 items from the PALPA Subtest 53. Finally, peripheral writing abilities were assessed before the initiation of treatment to confirm adequate graphomotor control for written production using a case conversion task (PALPA 22; e.g., A → a) and a direct copy task (e.g., dog → dog).
Treatment Materials
Approximately 50 common and proper nouns were identified for each participant as potential items to target for treatment. These items included names of family members, friends, and famous people, as well as street names and common objects that were relevant for the particular individual. Performance was probed on both oral and written naming for these items, and 40 were chosen that were named correctly on no more than one of three trials given on separate days. The target items were separated into two groups balanced for word length and semantic category, with 20 words assigned to CART + Repetition and 20 words treated in the Repetition Only condition.
To establish a consistent homework program, each participant was given an augmentative/alternative communication (AAC) device manufactured by Advanced Multimedia Devices Incorporated (AMDI) and loaned to the investigators by the Mayer-Johnson Company. The device included an array of 4 × 4 cm buttons (4 rows of 8) with an audio-recording feature. As items were entered into treatment, representative pictures for each target (either photographs or iconic representations) were affixed to a button, with the appropriate spoken label recorded. The left half of the device was used to display pictures for the Repetition Only condition, and the right side was used for CART + Repetition. Each side was labeled with icons to indicate the output modality (see Figure 2).
Fig. 2.
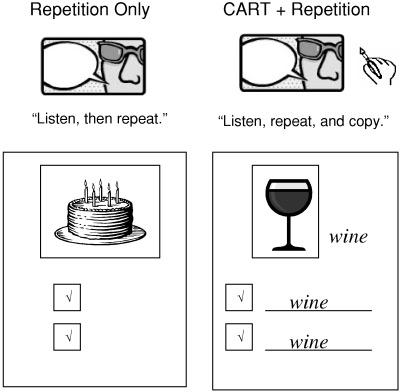
(Upper) Icons used on augmentative/alternative communication (AAC) device to indicate homework tasks: spoken repetition of words (Repetition Only) or Copy and Recall Treatment plus spoken repetition (CART + Repetition). (Lower) Portion of homework page for Repetition Only (for “cake”) and CART + Repetition (for “wine”).
Procedure
Each participant met with the clinician twice weekly for 10 weeks, either in the participant's home or at the university clinic. Daily homework that required between 30 and 60 minutes to complete was assigned. The frequency and duration of treatment implemented for this study was patterned after other studies using CART (Beeson et al., 2002, 2003a), and it was intended to be typical of service delivery for outpatient rehabilitation. Each session followed a similar format: All 40 words were probed at the beginning of the session, homework was reviewed, and then 10 words were targeted for treatment (5 for CART + Repetition, and 5 for the Repetition Only treatment). The order of treatments alternated from session to session. Using a multiple baseline design, three sets of words for each condition were treated in succession and one set was probed but not treated, thus providing a comparison for the treated sets.
CART + Repetition
The 20 targets in CART + Repetition were presented each session for the participant to orally name and then write the name. Next, the participant was cued to press the corresponding button on the AAC device, repeat the spoken model, and attempt to write the target again. For the target items that were being treated, unsuccessful oral responses to the probe were followed by corrective feedback and repeated opportunities to achieve correct spoken production. If the target was incorrectly written, the clinician called attention to errors and guided the participant to copy the written stimulus correctly. The naming and writing tasks were completed three times for each target and were followed by a recall trial in which the participant attempted to say the name of the item in response to the picture. Whether or not the target was named correctly, the participant pressed the button on the AAC device, and repeated the name of the item. Next, the participant attempted to write the target without a written model. If the participant incorrectly wrote the target during the recall trial, the written model was provided for copy. This recall sequence was also completed three times for each item during the treatment session.
The homework for this condition used the same format: spoken repetition using the AAC device, and repeated copying of each target item. A worksheet prompted 20 repetitions and copying of target words each day, as well as recall trials for each item. In effect, the treatment sessions served to train the participants to implement the homework procedures. The participants were instructed to put a check mark in a small box for each trial to indicate whether they judged the spoken production to be correct (see Figure 2). Although there was no means to confirm accuracy of production, the procedures were intended to promote self-evaluation and self-correction as needed.
Repetition Only
The Repetition Only treatment was designed to parallel CART + Repetition, but without the written production of target items. For each of the 20 targets, the clinician directed attention to a picture and asked the participant to name it. For the five targets being treated, the naming trial was followed by the participant pressing the corresponding button on the AAC device and repeating the model. After the spoken repetition, the clinician engaged the participant in conversation for 30 seconds to parallel the time taken to write in CART + Repetition, and then recall of the target name was prompted, followed by another repetition of the model. This sequence was completed six times for each item to parallel the three practice and three recall trials in CART + Repetition. For homework, the participant was instructed to attempt to orally name each target and to check the box if successful. After the naming attempt, the participant was instructed to push the button to hear and repeat the word. Twenty trials were prompted for each target word each day.
Criterion for moving to the next set
Treatment in therapy sessions continued for a set of 10 targets (5 for CART + Repetition, 5 for Repetition Only) until the participant achieved 80% (4 of 5) correct responses across two consecutive sessions for any of the three tasks: written or spoken naming in CART + Repetition, or spoken naming in the Repetition Only treatment. As subsequent sets were trained, homework continued for previous sets, but with fewer repetitions (5–10), so that the time demands were not unreasonable as more words were added.
Data Analyses
Effect sizes were calculated to provide a standardized index of change in performance in response to treatment. To do so, the d statistic was calculated according to procedures described by Busk and Serlin (1992; equation 2). Essentially, the d statistic reflects the change in performance following treatment divided by an estimate of performance variance. Specifically, we calculated the change from the baseline to maintenance phase for each of the treated sets of stimuli relative to the pooled variance observed in the baseline and maintenance phases. A summary d statistic that was weighted for the number of observations was obtained for each condition. The magnitude of the effect sizes was considered relative to other single-subject aphasia treatment studies with retrievable effect sizes (see review by Robey et al., 1999), such that 2.6, 3.9, and 5.8 were used as benchmarks for small, medium, and large sized effects, respectively.1
CASE REPORTS
Participant 1: NEM
NEM was a 60-year-old, left-handed male who suffered a left-hemisphere stroke at age 55. An magnetic resonance imaging scan taken approximately five years postonset revealed temporo-occipito-parietal damage, including the posterior superior temporal gyrus, posterior middle and inferior temporal gyri, and the angular gyrus, as depicted in Figure 3. NEM was a monolingual English speaker with seven years of education who had obtained his GED and worked as a musician for 30 years before his stroke. He had received speech and language therapy intermittently since the time of his stroke.
Fig. 3.
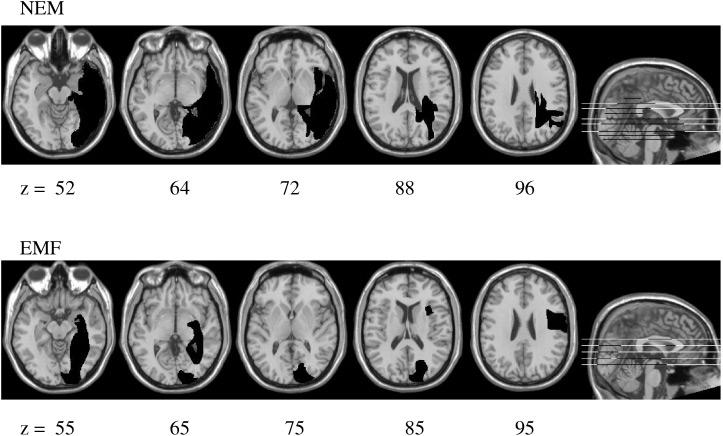
Left-hemisphere lesions for participants NEM and EMF mapped onto a standard brain template using MRIcro software (Rorden & Brett, 2000).
At five years after onset of stroke, NEM had an Aphasia Quotient of 62.9 and exhibited conduction aphasia according to the criteria of the WAB. He was able to successfully repeat single words, but demonstrated difficulty repeating multiword utterances. He had fluent speech with frequent word-finding difficulties. NEM was able to communicate with fair success by self-correction and circumlocution; however, he was especially frustrated with his inability to recall friends' names and the names of streets. He said that his goal was to “keep on working and be as good as I can be.” Given his limited level of formal education, it is important to note that NEM confirmed that his reading and writing were markedly impaired relative to his premorbid ability.
Pretreatment assessment
As indicated in Table 2, NEM demonstrated excellent non-verbal visual problem-solving skills on the Raven's Coloured Progressive Matrices (33/36 correct; 95%ile). He scored 47/52 (90.3%) on the Pyramids and Palm Trees Test, which was below the range indicated for the control group in the test manual (49–52; 94–100%), and was 2 standard deviations below the performance of 32 healthy control participants (mean age = 66.6 years) tested at the University of Arizona (mean = 50.96/52, SD = 1.092; Bartholow, 2005), thus raising some question regarding the status of NEM's semantic processing. Auditory processing of single words was relatively intact (39/40; PALPA 47). NEM showed impairment on the visual lexical decision task (PALPA 25), incorrectly identifying 5 real words as nonwords and 12 nonwords as real words (43/60 overall). Reading accuracy was impaired, as he matched 30/40 written words to their target pictures (PALPA 48), producing mostly semantic errors. NEM correctly repeated 37/40 words, but orally named only 13/40 of those same words (PALPA 53). Errors included circumlocution (e.g., boat-thing for canoe) and semantic errors (e.g., knife for fork) as well as partial word form errors (e.g., /swa/ for swan). Marked impairment in spelling was noted on written picture naming (9/40; PALPA 53) and writing-to-dictation tasks (15/40). NEM did not attempt to write the name for many of the pictured items, but on the writing-to-dictation task, the majority of his errors were phonologically plausible (e.g., bird → berd; toaster → tostr). NEM often sounded out each phoneme in a word as he wrote it, although not without errors (e.g., canoe → kanay; screw → scrua). It was notable, however, that NEM wrote the correct first letter (or a plausible substitution) for all responses on the writing-to-dictation task. Direct assessment of his sublexical processing of orthography revealed difficulty reading nonwords (20% correct) and spelling nonwords (55% correct). With regard to single-letter writing, NEM demonstrated significant difficulty converting capital letters to their lowercase allographs (4/26), but could convert lower to uppercase letters with few errors. His direct copying skills were largely intact (8/10).
Table 2.
Participant performance on pretreatment measures
| Participant |
||
|---|---|---|
| Pre-treatment measure | NEM | EMF |
| Raven's Coloured Progressive Matrices | 33/36 | 12/36* |
| Visual lexical decision PALPA 25 |
43/60* | 46/60* |
| Written word-to-picture match PALPA 48 |
30/40* | 28/40* |
| Spoken word-to-picture match PALPA 47 |
39/40 | 29/40* |
| Semantic test | 47/52 | 36/52* |
| Pyramids and Palm Trees Test | ||
| Verbal repetition PALPA 53 |
37/40* | 40/40 |
| Oral naming PALPA 53 |
13/40* | 11/40* |
| Written naming PALPA 53 |
9/40* | 3/40* |
| Writing to dictation PALPA 53 |
15/40* | 3/40* |
| Upper to lowercase letters | 4/26* | 15/26* |
| Lower to uppercase letters | 21/26* | 13/26* |
| Direct copy | 8/10* | 10/10 |
Note. PALPA = Psycholinguistic Assessment of Language Processing in Aphasia.
Impaired performance
In summary, at five years after stroke, NEM demonstrated fairly good auditory comprehension at the single-word and sentence levels, with persistent marked anomia and residual difficulty with repetition of verbal information. His single-word reading and spelling were notably impaired. The reading difficulty appeared to reflect both visual/orthographic processing difficulties (viz., lexical decision errors) and impaired access to semantics (viz., semantic errors on written word-to-picture matching). The fact that NEM's nonword reading was more impaired than his nonword spelling was also consistent with some impairment of visual processing of orthography. Although NEM attempted to use sublexical phonology to assemble spellings for words that he could not recall, his phonological abilities were not adequate to do so consistently. These behavioral findings were relatively consistent with NEM's lesion affecting nearly the full anterior–posterior extent of the left inferior temporo-occipital cortex, and extending dorsally into posterior perisylvian regions.
Response to treatment
A set of 40 words was identified for treatment for NEM that included many proper names of interest to him, such as names of musicians and local street names. The average word length was 7.35 letters, with a range of 2 to 12. Before treatment, NEM did not write any target words correctly, and orally named only 2 of the 40 targets on one of three baseline probes. Over the course of 10 weeks, he attended 17 of 17 sessions and completed 92% of his homework with 99% accuracy for written copying. NEM's spelling accuracy on the recall trials was 98%, and his self-assessment of accuracy for spoken production was 99% in CART + Repetition recall trials and 88% for the Repetition Only recall trials. He reported that the daily homework typically required approximately 30 minutes.
As shown in Figure 4, NEM demonstrated improvement for the three sets of treated words and maintained that improvement throughout the treatment phase. For Sets 1 and 2, NEM attained criterion simultaneously for oral naming and written naming in CART + Repetition. For Set 3, he only attained criterion for written naming. In response to CART + Repetition, NEM's performance yielded very large effect sizes for improvement in written (d = 9.49) and spoken naming (d = 17.41). For the items trained with Repetition Only, there was also a large effect size (d = 6.51) for spoken naming (see Table 3). It was noteworthy that during treatment probes for CART + Repetition, NEM wrote the target before naming it orally on 12% of trials, suggesting that he used orthography to guide retrieval of phonology in some instances. Even during the Repetition Only probes, NEM showed evidence of using residual orthography to help retrieve the phonology of a word. For example, he said, “It's a short one … four letters … starts with ‘u’ … Utah.”
Fig. 4.

NEM's performance on probes during baseline, treatment, maintenance, and follow-up for 4 sets of words (Sets 1–3 treated; Set 4 untreated). CART, Copy and Recall Treatment; Rep, Repetition.
Table 3.
Treatment effect sizes (d statistic) for each participant written and oral naming
| Participant |
|||
|---|---|---|---|
| Condition | Task | NEM | EMF |
| CART + Repetition | Written naming | 9.49 | 16.62 |
| Oral naming | 17.41 | 3.46 | |
| Repetition Only | Oral naming | 6.51 | 2.62 |
Note. The d statistic was calculated on the basis of baseline scores relative to posttreatment performance during the maintenance phase. CART = Copy and Recall Treatment.
On a follow-up probe conducted approximately 6 weeks after treatment, NEM correctly spelled 7 of 15 treated words in CART + Repetition, 5 words had minor spelling errors (e.g., Johnne Cash for Johnny Cash), 1 word had several letters omitted (Lefft Frizz for Lefty Frizzell ), and he could not recall 3 spellings from Set 3. He was able to orally name 12 of 15 treated words in CART + Repetition and 10 of 15 treated words from the Repetition Only treatment. NEM reported frequent use of friends' names and street names that were targeted in therapy.
Posttreatment assessment
As illustrated in Table 4, NEM demonstrated little change between pre- and posttreatment measures for untrained targets on all four tasks measured by the PALPA 53. This finding suggests that his response to treatment was specific to the trained items.
Table 4.
Participant performance on the PALPA 53 pre- and posttreatment (untrained items)
| Participant |
||
|---|---|---|
| Task | NEM | EMF |
| Writing to dictation | ||
| Pre | 15/40 | 3/40 |
| Post | 16/40 | 3/40 |
| Written naming | ||
| Pre | 9/40 | 3/40 |
| Post | 7/40 | 2/40 |
| Repetition | ||
| Pre | 37/40 | 40/40 |
| Post | 37/40 | 40/40 |
| Oral naming | ||
| Pre | 13/40 | 11/40 |
| Post | 14/40 | 14/40 |
Note. PALPA = Psycholinguistic Assessment of Language Processing in Aphasia.
Discussion
Before the initiation of treatment, NEM showed marked impairment of orthographic and phonological representations (or impaired access to such representations). Spelling and oral naming of targeted items clearly improved relative to the untrained items. While he responded well to both treatment approaches, NEM's improvement in spoken naming was strongest for items that were trained using CART + Repetition. In fact, after several weeks of treatment, NEM commented to the researchers that he was learning best with the CART + Repetition approach compared with the Repetition Only procedure. This finding was consistent with his self-assessment of spoken naming accuracy on the homework, which was higher in the CART + Repetition condition (98 vs. 88% correct). Whereas NEM's improvement during treatment was strong, his drop in performance on the follow-up probes conducted six weeks after treatment was disappointing. The fact that new learning was fragile without continued practice suggests that additional training or a maintenance program of homework should be considered to better ensure more durable effects.
Although the treatment did not focus on sublexical spelling procedures, it was evident that NEM used orthography to self-cue spoken naming of target words to some extent. He often sounded out the pronunciation of words after he had written them, but he did not rely on letter-sound correspondences to such an extent that regularization errors were made. It also remained evident that NEM's phonological skills were not intact and that he might benefit from a subsequent treatment phase directed toward strengthening letter–sound correspondences to further reinforce links between orthography and phonology.
Participant 2: EMF
EMF was a 72-year-old, right-handed female who suffered left frontal and brainstem aneurysms and a subarachnoid hemorrhage at age 67. After surgeries to repair an aneurysm of the anterior communicating artery, EMF exhibited significant expressive language deficits with dense right hemiplegia and right neglect. A computed tomography scan revealed left-hemisphere damage affecting inferior temporo-occipital regions, as well as the dorsolateral sensorimotor cortex (see Figure 3). She was a monolingual English speaker with 14 years of education who worked as a nurse and was retired at the time of the onset of language impairment. Before the initiation of this study, she had received speech-language treatment for two years.
At five years after onset, EMF's Aphasia Quotient was 64.2, and her spoken output was borderline fluent so that she appeared to have evolved from Broca's aphasia to anomic aphasia according to the WAB criteria. Her speech had reduced grammatical complexity and also contained frequent use of stereotyped utterances, such as “Jean” to indicate any person, “write the book” to indicate actions, or “B.W.” (the name of her cat) to indicate an object. When talking with EMF, her husband bore much of the burden of conversation, and many communication breakdowns went unrepaired.
Pretreatment assessment
As summarized in Table 2, EMF demonstrated impairments to several language components. Semantic processing was severely impaired as indicated by a score of 36/52 on the Pyramids and Palm Trees Test. Semantic impairment was also evident on the spoken word-to-picture matching task (PALPA 47); she correctly matched 29/40 items, with 9 close semantic errors and 2 visually similar errors. On the Raven's Coloured Progressive Matrices, EMF achieved a score of 12/36 (8%ile), indicating poor nonverbal visual problem-solving abilities. She achieved a score of 46/60 on the visual lexical decision task (PALPA 25) and was able to match only 28/40 written words to their pictures (PALPA 48). Although her repetition skills were excellent (40/40), EMF was able to correctly name only 11/40 stimuli on the PALPA 53, with primarily semantic errors. EMF had limited residual spelling ability; she correctly spelled 3/40 items on both the writing-to-dictation and written naming tasks (PALPA 53). Spelling errors bore little resemblance to the target (e.g., doam for swan), and only 13/37 error responses began with the correct first letter. Thus EMF showed marked degradation of orthographic knowledge and an inability to use phonology to retrieve orthography. With regard to peripheral writing skills, allographic conversion was impaired as demonstrated by her difficulty transcoding both upper and lowercase letters (15/26 and 13/26, respectively), but her direct copying skills were excellent (10/10).
To summarize, at five years after stroke, EMF had hesitant spoken language production with reduced fluency and marked anomia. She demonstrated degraded semantic knowledge that affected performance on spoken and written language tasks. In addition, she had visual/orthographic impairment affecting lexical decisions, and degraded memory for letter shapes. In comparison to NEM, her semantic impairment was of greater severity, and her poor performance on the Raven's Coloured Progressive Matrices suggested additional impairment of nonverbal problem solving. These differences in semantic processing are not readily explained by inspection of the lesions, in that NEM had more extensive temporal lobe damage than EMF. Her anomia and diminished orthographic knowledge were consistent with damage to left inferior temporo-occipital cortex. Additional damage to perisylvian cortex was not extensive, but lesions affecting the insula and rolandic regions may be associated with her limited sublexical phonological abilities. Her history of nonfluent language and reduced grammatical complexity were consistent with a disruption to frontal language regions.
Response to treatment
The 40 words targeted for treatment for EMF included items such as caregivers' names, common objects, and local stores. Word length ranged from 2 to 15 letters with an average of 6.25 letters per word. Before the initiation of treatment, EMF was unable to write any of the target words and orally named 11/40 targets in one of three baseline probes. Over the course of 10 weeks of treatment, EMF attended 18 of 19 sessions. She reported that she spent approximately an hour on her daily homework and did not always complete it fully. The homework pages showed that EMF completed 76% of homework with 99% accuracy for the copy trials; she was 97% accurate on the recall trials for written production and scored herself as 97% accurate for spoken production in CART + Repetition recall trials, and 94% accurate for spoken production in the Repetition Only trials.
As shown in Figure 5, EMF reached criterion on the written naming task for the three treated word sets, but not for the spoken naming tasks. In response to CART + Repetition, EMF demonstrated a very large effect size for improvement in written naming (d = 16.62), and a small effect size for spoken naming (d = 3.46). The treatment effect for spoken naming in the Repetition Only treatment was also small (d = 2.62).
Fig. 5.

EMF's performance on probes during baseline, treatment, maintenance, and follow-up for 4 sets of words (Sets 1–3 treated; Set 4 untreated). CART, Copy and Recall Treatment; Rep, Repetition.
Of note, during treatment EMF often produced semantic errors when orally naming a target. For example, she said “Mary” (treated in Set 1) for Carolyn (Set 3). By contrast, she rarely made semantic errors in written naming. In fact, on occasion, she would correctly write Carolyn but say “Mary.” EMF showed no ability to use orthography to retrieve phonology, but she was highly responsive to spoken phonemic cues provided by the experimenter.
Similar to NEM, EMF showed a decrement in performance on a follow-up probe conducted approximately 6 weeks posttreatment. She was able to correctly write the names of 13/15 treated targets and orally name 5/15 targets in CART + Repetition, and 11/15 treated targets in the Repetition Only treatment.
Posttreatment assessment
As shown in Table 4, very little change took place between pre- and posttreatment measures on untreated items (PALPA 53), suggesting that EMF had an item-specific response to treatment for both spelling and oral naming of targets. However, changes in error types were noted for written naming following treatment. During pretreatment, EMF demonstrated predominantly nonwords as error responses, but following treatment her errors included visually similar real words, suggesting improved access to orthographic representations.
To better understand EMF's abilities, an additional oral reading task was administered. She was able to correctly read aloud 20/30 words that had been trained, but only 1/30 untrained words (matched to trained words for grammatical class and word length), and 0/10 nonwords (matched for word length). Thus she had improved access to the trained phonological representations, but was unable to use orthography to cue access to phonology at a lexical or sublexical level for untrained items.
Discussion
At the outset, EMF presented with marked anomia and severe impairment of written language. She made excellent progress relearning written spellings of treated words. Her improvements in spoken naming were apparent relative to untrained items but modest compared with improvements in written naming, and the improvements during treatment were similar for the two conditions. It was noteworthy that, during treatment, EMF frequently made semantic errors in spoken naming but rarely made such errors in writing. Thus it appeared that orthographic knowledge served to block semantic errors in writing, but she could not use orthography to access phonology to assist in spoken production. Given that her rate of improvement in spoken production was slower than written production (and less durable at follow-up), EMF might have benefited from extended treatment for each set of words until mastery was achieved for both modalities.
GENERAL DISCUSSION
This study was designed to (1) examine the therapeutic effect of treatment for single word spelling and spoken naming in two individuals with aphasia, and (2) determine whether treatment directed toward repeated, corrected practice of written words paired with verbal repetition (CART + Repetition) led to better oral naming than a verbal repetition task alone (Repetition Only). Over the course of 10 weeks of treatment, both participants were successful in improving written naming of target words, suggesting that specific orthographic representations were strengthened. In addition, NEM showed marked improvement in spoken naming for items trained using CART + Repetition, and this improvement was greater than that obtained from the Repetition Only treatment. The other participant, EMF, made modest improvements in spoken naming, irrespective of treatment condition.
Both participants were motivated to participate in the treatment and were consistent in their attendance, but NEM completed a larger percentage of the assigned homework compared with EMF (92 vs. 76%), and it was apparently accomplished in a shorter period of time. It may be relevant that NEM was 12 years younger than EMF and was certainly the more energetic of the two. He led a more active and independent lifestyle and may have brought more effort to the treatment enterprise than EMF. However, the differences in their response to treatment appear to be better explained from a cognitive perspective.
In the case of NEM, we postulate that strengthened orthographic representations provided additional support to access phonology, which was the intended effect of treatment. The CART + Repetition protocol was lexical in the sense that whole word orthography and phonology were stimulated, but NEM also appeared to derive some benefit from sublexical phonology. Although EMF was responsive to the writing treatment, in that she relearned the targeted spellings, orthography did not appear to provide additional input to phonology. Despite the fact that she was responsive to phonemic cues provided by the experimenter, EMF was unable to derive phonology for self-cueing. The pretreatment assessment revealed these differences between the two participants to some extent. NEM performed better on writing to dictation than on written picture naming, and his error responses included phonologically plausible errors and frequent knowledge of the correct first letter. In contrast, EMF performed equally poorly on written picture naming and writing to dictation, and her spelling attempts bore little resemblance to the target. In other words, from the outset, NEM provided some evidence of taking advantage of links between phonology and orthography, whereas EMF did not. These findings suggest that pretreatment assessment can provide prognostic clues regarding the potential benefit of CART + Repetition as a means to improve both written and spoken naming.
The pretreatment assessment also showed that EMF had marked semantic impairment that was evident on comprehension and spoken naming tasks. Although she mastered written naming of targeted items with no evidence of semantic errors, such errors persisted in spoken naming. It may have been the case that strengthened orthography served to block semantic errors in writing, but access to phonology remained weak. EMF improved her spoken naming with both treatment approaches, albeit at a slower rate than observed for writing, so continued treatment might have proven successful. EMF's impaired semantic processing may have been an important limiting factor in her response to treatment, so that treatment directed more specifically toward semantic knowledge might have been necessary to remediate spoken naming impairments. With regard to the more peripheral aspects of writing, both participants showed some degradation of letter shape knowledge, as indicated by their performance on the case conversion tasks, but the repeated copying of CART proved adequate to strengthen specific orthographic word forms.
A comparison of lesion location and extent does not fully explain differences in levels of performance between the two participants, nor would it necessarily lead one to predict that NEM would be more responsive to treatment than EMF. NEM's lesion was the more extensive, affecting most of the inferior temporo-occipital cortex and extending into posterior perisylvian regions. EMF's lesion was less extensive, but more diffuse than NEM's, and included damage to frontal and insular cortices, which may have contributed to her more limited ability to derive phonology from orthography. We are reluctant to over-interpret the lesion information from two subjects, given individual variability and the fact that the functional integrity of residual cortex was unknown. However, these cases may serve as a basis of comparison for participants examined in future studies. Of particular interest will be the integrity of left anterior perisylvian regions, which seem to play a particularly important role in phonological processing (Henry et al., 2006; Omura et al., 2004; Rapcsak & Beeson, 2002).
In summary, this study demonstrated the potential benefit of the CART + Repetition protocol as a lexical treatment to improve written naming of a corpus of personally relevant words. The effect on spoken naming was stronger when there was some residual phonological ability so that links between orthography and phonology were enhanced, as observed in NEM.
For both participants, the treatment effects were specific to the trained items, with little generalization to untrained words. While generalization of treatment effects is a desirable outcome, the value of regaining the ability to communicate specific personally relevant information has considerable functional significance regardless. Such benefit was explicitly expressed by NEM as he regained the ability to write and say names of friends, musicians, and the like (see also Beeson, 1999; Clausen & Beeson, 2003). The decrements in performance at the 6-week follow-up suggest that this relatively short course of treatment should be lengthened, of increased intensity, or followed by continued homework to maximize benefit and stabilize performance. Future research should explore adjustments in the treatment schedule and criteria for mastery of individual items; it should also explore the value of complementary treatment to strengthen sublexical phonology to assist in written and spoken naming.
ACKNOWLEDGMENTS
The authors thank Dr. Steven Rapcsak for the referral of NEM to our research project. We also express our gratitude to the Mayer-Johnson Company for providing the augmentative devices used to implement homework with the participants in this study. This work was funded in part by RO1DC007646 from the National Institute on Deafness and Other Communication Disorders. The information in this manuscript is new and original and has never been published electronically or in print. The authors have no conflicts of interest to declare.
Footnotes
These values are notably larger than the effect sizes typically obtained from group research designs, wherein Cohen (1988) suggested that benchmarks of .20, .50, and .80 are considered to reflect small, medium, and large effect sizes. Because benchmarks have not been established for single subject research in aphasia, we cite the effect sizes from the meta-analysis of single-subject research in aphasia by Robey et al. (1999) as an appropriate metric for the interpretation of the results of this research. See also Beeson et al. (2005) for a similar use of these benchmarks. We anticipate that these benchmarks should continue to be refined as treatment research advances.
REFERENCES
- Alexander MP, Friedman RB, Loverso F, Fischer RS. Lesion localization in phonological agraphia. Brain and Language. 1992;43:83–95. doi: 10.1016/0093-934x(92)90022-7. [DOI] [PubMed] [Google Scholar]
- Aliminosa D, McCloskey M, Goodman-Schulman R, Sokol S. Remediation of acquired dysgraphia as a technique for testing interpretations of deficits. Aphasiology. 1993;7:55–69. [Google Scholar]
- Bartholow K. Examining the validity of the Arizona Semantic Test. University of Arizona; 2005. Unpublished Master's thesis. [Google Scholar]
- Bastiaanse R, Bosje M, Franssen M. Deficit-oriented treatment of word-finding problems: Another replication. Aphasiology. 1996;10:363–383. [Google Scholar]
- Beeson PM. Treating acquired writing impairment: Strengthening graphemic representations. Aphasiology. 1999;13:367–386. [Google Scholar]
- Beeson P, Hirsch F, Rewega M. Successful single-word writing treatment: Experimental analysis of four cases. Aphasiology. 2002;16:473–492. [Google Scholar]
- Beeson PM, Magloire J, Robey RR. Letter-by-letter reading: Natural recovery and response to treatment. Behavioural Neurology. 2005;16:191–202. doi: 10.1155/2005/413962. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Beeson PM, Rapcsak SZ, Plante E, Chargualaf J, Chung A, Johnson SC, Trouard T. The neural substrates of writing: A functional magnetic resonance imaging study. Aphasiology. 2003b;17:647–665. [Google Scholar]
- Beeson P, Rising K, Volk J. Writing treatment for severe aphasia: Who benefits? Journal of Speech, Language, and Hearing Research. 2003a;46:1038–1060. doi: 10.1044/1092-4388(2003/083). [DOI] [PubMed] [Google Scholar]
- Best W, Nickels L. From theory to therapy in aphasia: Where are we now and where to next? Neuropsychological Rehabilitation. 2000;10:231–247. [Google Scholar]
- Binder J, Price CJ. Functional neuroimaging of language. In: Cabeza R, Kingstone A, editors. Handbook of functional neuroimaging of cognition. MIT Press; Cambridge, MA: 2001. pp. 187–251. [Google Scholar]
- Boyle M. Semantic feature analysis treatment for anomia in two fluent aphasia syndromes. American Journal of Speech-Language Pathology. 2004;13:236–249. doi: 10.1044/1058-0360(2004/025). [DOI] [PubMed] [Google Scholar]
- Bruce C, Howard D. Computer generated phonemic cues: An effective aid for naming in aphasia. British Journal of Disorders of Communication. 1987;22:191–201. doi: 10.3109/13682828709019862. [DOI] [PubMed] [Google Scholar]
- Busk PL, Serlin RC. Meta-analysis for single-case research. In: Kratochwill TR, Levin JR, editors. Single-case research design and analysis: New directions for psychology and education. Lawrence Erlbaum Associates; Hillsdale, NJ: 1992. pp. 187–212. [Google Scholar]
- Clausen NS, Beeson PM. Conversational use of writing in severe aphasia: A group treatment approach. Aphasiology. 2003;17:625–644. [Google Scholar]
- Cohen J. Statistical power analysis for the behavioral sciences. 2nd ed. Lawrence Erlbaum Associates; Hillsdale, NJ: 1988. [Google Scholar]
- Cohen L, Dehaene S. Specialization within the ventral stream: The case for the visual word form area. Neuroimage. 2004;22:466–476. doi: 10.1016/j.neuroimage.2003.12.049. [DOI] [PubMed] [Google Scholar]
- DeDe G, Parris D, Waters G. Teaching self-cues: A treatment approach for verbal naming. Aphasiology. 2003;17:465–480. [Google Scholar]
- Drew RL, Thompson CK. Model-based semantic treatment for naming deficits in aphasia. Journal of Speech, Language, and Hearing Research. 1999;42:972–989. doi: 10.1044/jslhr.4204.972. [DOI] [PubMed] [Google Scholar]
- Ellis AW. Reading, writing and dyslexia: A cognitive analysis. 2nd ed. Lawrence Erlbaum Associates; Hillsdale, NJ: 1993. [Google Scholar]
- Fiez J. Phonology, semantics, and the role of the left inferior prefrontal cortex. Human Brain Mapping. 1997;5:79–83. [PubMed] [Google Scholar]
- Franklin S, Buerk F, Howard D. Generalised improvement in speech production for a subject with reproduction conduction aphasia. Aphasiology. 2002;16:1087–1114. [Google Scholar]
- Henry ML, Beeson PM, Stark AL, Rapcsak SZ. The role of left perisylvian cortical regions in spelling. Brain and Language. 2006;99 doi: 10.1016/j.bandl.2006.06.011. in press. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hillis AE. Efficacy and generalization for aphasic naming errors. Archives of Physical Medicine and Rehabilitation. 1989;70:632–636. [PubMed] [Google Scholar]
- Hillis AE, Caramazza A. Theories of lexical processing and rehabilitation of lexical deficits. In: Riddoch MJ, Humphreys GW, editors. Cognitive neuropsychology and cognitive rehabilitation. Lawrence Erlbaum Associates; London: 1994. pp. 449–484. [Google Scholar]
- Holland A. A strategy for improving oral naming in an individual with a phonological access impairment. In: Helm-Estabrooks N, Holland AL, editors. Approaches to the treatment of aphasia. Singular; San Diego, CA: 1998. pp. 39–67. [Google Scholar]
- Howard D, Patterson K. Pyramids and palm trees: A test of semantic access from pictures and words. Thames Valley Test Company; Bury St. Edmunds, UK: 1992. [Google Scholar]
- Kay J, Lesser R, Coltheart M. Psycholinguistic assessment of language processing in aphasia (PALPA) Thames Valley Test Company; Bury St. Edmunds, UK: 1992. [Google Scholar]
- Kertesz A. Western aphasia battery. Grune & Stratton; New York: 1982. [Google Scholar]
- Kiran S, Thompson CK. The role of semantic complexity in treatment of naming deficits: Training semantic categories in fluent aphasia by controlling exemplar typicality. Journal of Speech, Language, and Hearing Research. 2003;46:773–787. doi: 10.1044/1092-4388(2003/061). [DOI] [PMC free article] [PubMed] [Google Scholar]
- Margolin DI. The neuropsychology of writing and spelling: Semantic, phonological, motor and perceptual processes. Quarterly Journal of Experimental Psychology. 1984;36A:459–489. doi: 10.1080/14640748408402172. [DOI] [PubMed] [Google Scholar]
- Marshall J, Pound C, White-Thomson M, Pring T. The use of picture/word matching tasks to assist word retrieval in aphasic patients. Aphasiology. 1990;4:167–184. [Google Scholar]
- Miceli G, Amitrano A, Capasso R, Caramazza A. The treatment of anomia resulting from output lexical damage: Analysis of two cases. Brain and Language. 1996;52:150–174. doi: 10.1006/brln.1996.0008. [DOI] [PubMed] [Google Scholar]
- Mummery CJ, Patterson K, Price CJ, Ashburner J, Frackowiak RSJ, Hodges JR. A voxel-based morphometry study of semantic dementia: Relationship between temporal lobe atrophy and semantic memory. Annals of Neurology. 2000;47:36–45. [PubMed] [Google Scholar]
- Nakamura K, Honda M, Hirano S, Oga T, Sawamoto N, Hanakawa T, Inoue H, Ito J, Matsuda T, Fukuyama H, Shibasaki H. Modulation of the visual word retrieval system in writing: A functional MRI study on the Japanese orthographies. Journal of Cognitive Neuroscience. 2002;14:104–115. doi: 10.1162/089892902317205366. [DOI] [PubMed] [Google Scholar]
- Nickels L. The autocue? Self-generated phonemic cues in the treatment of a disorder of reading and naming. Cognitive Neuropsychology. 1992;9:155–182. [Google Scholar]
- Nickels L, Best W. Therapy for naming deficits (part II): Specifics, surprises, and suggestions. Aphasiology. 1996;10:109–136. [Google Scholar]
- Omura K, Tsukamoto T, Kotani Y, Ohgami Y, Yoshikawa K. Neural correlates of phoneme-to-grapheme conversion. Neuroreport. 2004;15:949–953. doi: 10.1097/00001756-200404290-00004. [DOI] [PubMed] [Google Scholar]
- Rapcsak SZ, Beeson PM. Neuroanatomical correlates of spelling and writing. In: Hillis AE, editor. Handbook of adult language disorders: Integrating cognitive neuropsychology, neurology, and rehabilitation. Psychology Press; Philadelphia: 2002. pp. 71–99. [Google Scholar]
- Rapcsak SZ, Beeson PM. The role of left posterior inferior temporal cortex in spelling. Neurology. 2004;62:2221–2229. doi: 10.1212/01.wnl.0000130169.60752.c5. [DOI] [PubMed] [Google Scholar]
- Rapp B, Benzig L, Caramazza A. The autonomy of lexical orthography. Cognitive neuropsychology. 1997;14:71–104. [Google Scholar]
- Raven JC. Coloured progressive matrices. H.K. Lewis; London: 1976. [Google Scholar]
- Robey RR, Schultz MC. A model for conducting clinical-outcome research: An adaptation for use in aphasiology. Aphasiology. 1998;12:787–810. [Google Scholar]
- Robey RR, Schultz MC, Crawford AB. Single-subject clinical outcome research: Designs, data, effect sizes, and analysis. Aphasiology. 1999;13:445–473. [Google Scholar]
- Robson J, Marshall J, Chiat S, Pring T. Enhancing communication in jargon aphasia: A small group study of writing therapy. International Journal of Language and Communication Disorders. 2001;36:471–488. doi: 10.1080/13682820110089371. [DOI] [PubMed] [Google Scholar]
- Roeltgen DP, Sevush S, Heilman KM. Phonological agraphia: Writing by the lexical-semantic route. Neurology. 1983;33:755–765. doi: 10.1212/wnl.33.6.755. [DOI] [PubMed] [Google Scholar]
- Rorden C, Brett M. Stereotaxic display of brain lesions. Behavioural Neurology. 2000;12:191–200. doi: 10.1155/2000/421719. [DOI] [PubMed] [Google Scholar]
- Sugishita M, Seki K, Kabe S, Yunoki K. A material-control single-case study of the efficacy of treatment for written and oral naming difficulties. Neuropsychologia. 1993;31:559–569. doi: 10.1016/0028-3932(93)90052-2. [DOI] [PubMed] [Google Scholar]
- Tainturier M-J, Rapp B. The spelling process. In: Rapp B, editor. The handbook of cognitive neuropsychology: What deficits reveal about the human mind. Psychology Press; Philadelphia: 2001. pp. 263–289. [Google Scholar]
- Vandenberghe R, Price C, Wise R, Josephs O, Frackowiak RSJ. Functional anatomy of a common semantic system for words and pictures. Nature. 1996;383:254–256. doi: 10.1038/383254a0. [DOI] [PubMed] [Google Scholar]