

Abstract
Background
Current theoretical models of nicotine dependence assume a close relationship between use and dependence; however, previous data suggest that many daily smokers fail to develop nicotine dependence.
Objectives
To determine what percentage of daily smokers fail to meet DSM-IV criteria for nicotine dependence within their lifetime, how non-dependence relates to duration and quantity of cigarette use, and whether other tobacco use and/or specific dependence criteria differentiate never-dependent and dependent smokers.
Methods
Cross-sectional data collected via personal interview from a nationally representative sample of 8213 past year daily smokers were analyzed.
Results
Approximately 39.4% of daily smokers never reached nicotine dependence. While the probability of remaining non-dependent decreased with smoking quantity and duration since the onset of daily smoking, a substantial portion of individuals (37.7%) who reported smoking ≥ 10 cigarettes per day and began smoking daily ≥ 10 years prior, remained never nicotine dependent.
Conclusions
The absence of nicotine dependence in heavy daily smokers may result from limitations in the measurement of dependence and/or nicotine exposure. Alternatively, some individuals may be relatively resistant to becoming nicotine dependent despite extensive use. The latter explanation would have important implications for understanding the nature of nicotine dependence.
1.0. Background
Current theories of nicotine dependence focus on the neurobiological effects of nicotine, stimuli paired with nicotine delivery and the repeated performance of nicotine-use behaviors as primary determinants of nicotine dependence (Balfour, 2004, Caggiula et al., 2002, Tiffany, 1990). An assumption of these theories is that dependence is closely related to the duration and quantity of use. While nicotine use is a necessary requirement for nicotine dependence and the rates of dependence increase with levels of use, a substantial number of smokers do not meet criteria for nicotine dependence (Breslau et al., 2001, Dierker et al., 2006, Kandel and Chen, 2000).
The purpose of the present study was to determine the proportion of daily smokers who fail to meet DSM-IV criteria for nicotine dependence, examine how this relates to both the duration and quantity of cigarette use, and describe any use and/or dependence characteristics that may differentiate dependent and non-dependent moderate-to-heavy daily smokers. The possibility that some individuals may be relatively resistant to developing DSM-IV nicotine dependence despite extensive use raises many important and interesting hypotheses, including that DSM-IV criteria are relative insensitive measures of dependence or conversely that nicotine use is necessary, but not sufficient, for dependence to occur.
2.0. Methods
2.1. Sample
A nationally representative sample of 43,093 non-institutionalized adults in the United States age 18 and older were personally interviewed from August 2001 to May 2002 as part of the National Epidemiologic Study on Alcohol and Related Conditions (NESARC), described in detail elsewhere (Grant et al., 2004b). Preliminary analyses focused on 18,013 individuals who reported smoking 100+ lifetime cigarettes confirmed previous reports (Breslau et al., 2001) indicating that the onset of daily smoking precedes or is concurrent with the onset of DSM nicotine dependence in the vast majority (95%) of cases. Given our interest in nicotine dependence, we focused the present analyses on past-year daily smokers (n=8213).
The sample was 46.7% female, 7.4% Hispanic, 10.8% African-American, 2.2% Asian, and 85.9% Caucasian. On average [mean (SEM)], participants were 41.4 (0.19) years of age, smoked 17.4 (0.14) cigarettes per day (cpd), initiated smoking 25.6 (0.19) years earlier, and initiated daily smoking 23.0 (0.19) years earlier. The distribution of current smoking quantity was as follows: 10.4% (1–5 cpd), 25.2% (6–10 cpd), 8.9% (11–15 cpd), 39.3% (16–20 cpd), 8.9% (21–30 cpd), 5.2% (31–40 cpd), and 2.1% (>40 cpd). The distribution of years since daily smoking onset was 3.9% (<1 yr), 10.0% (2–5 yrs), 11.8% (6–10 yrs), 10.5% (11–15 yrs), 11.5% (16–20 yrs), 23.2% (21–30 yrs), 16.0% (31–40 yrs), 8.9% (41–50 yrs), and 4.1% (>50 yrs).
2.2. Assessments
Tobacco use was assessed by the tobacco module of the Alcohol Use Disorder and Associated Disabilities Interview Schedule-IV (AUDADIS-IV) which contains detailed questions on tobacco use and DSM-IV nicotine dependence. It has demonstrated good to excellent test-retest reliability of lifetime nicotine dependence and tobacco use measures (Intraclass correlation coefficients=0.60–0.92; Grant et al., 2003). The AUDADIS-IV measure of nicotine dependence has been show to relate to pathological gambling (Petry et al., 2005), depression, and alcohol dependence (Dierker and Donny, under review), and similar measures of DSM-IV dependence (i.e., Composite International Diagnostic Interview) have been shown to predict future smoking behavior (Sledjeski et al., 2006)*. Notably, withdrawal criteria were defined liberally to include either four or more specific symptoms of withdrawal (Symptom 2a; Table 1) or one of the following (Symptom 2b; Table 1): using tobacco during the night, using tobacco just after awakening, using tobacco just after a situation where smoking was restricted, or using tobacco to avoid withdrawal symptoms (Grant et al., 2004a). Cigarette use questions examined in the present analyses included “About how old were you when you smoked your first full cigarette?,” “About how old were you when you first started smoking everyday?,” “About how often did you usually smoke in the past year?” and “On the days that you smoked in the last year, about how many cigarettes did you usually smoke?”
Table 1.
Weighted percent or mean (SEM) demographic characteristics, smoking history, and dependence symptoms in long-term (>10 years), daily (>10 cpd) smokers.
| Dependent (n=3292) | Never Dependent (n=1989) | P value | |
|---|---|---|---|
| Age | 45.09 (0.24) | 48.45 (0.34) | .0001 |
| % Male | 51.6 | 57.1 | .0012 |
| % Black | 15.2 | 18.2 | .0282 |
| % Hispanic | 3.9 | 6.2 | .0010 |
| Less than a high school degree | 20.0 | 21.1 | .957 |
| Age of smoking initiation | 15.15 (0.08) | 16.07 (0.11) | .0001 |
| Age of onset daily | 17.51 (0.09) | 18.26 (0.13) | .0001 |
| % using other tobacco (lifetime*) | 25.2 | 19.7 | .0003 |
| % using other tobacco (past year) | 9.8 | 8.1 | .0925 |
| Days since last cigarette | 5.77 (0.62) | 5.71 (0.84) | .9549 |
| Number of symptoms of nicotine dependence | 4.60 (0.03) | 2.03 (0.03) | <.0001 |
| % Symptom 1 (Tolerance) | 42.1 | 6.5 | <.0001 |
| % Symptom 2a (Withdrawal; Grant et al. 2004) | 98.2 | 68.2 | <.0001 |
| % Symptom 2b (Withdrawal; ≥ 4 DSM-IV symptoms) | 48.1 | 10.6 | <.0001 |
| % Symptom 2a OR 2b (Withdrawal) | 98.7 | 68.9 | <.0001 |
| % Symptom 3 (Larger amount/longer period) | 60.7 | 11.1 | <.0001 |
| % Symptom 4 (Difficulty cutting down) | 96.8 | 72.2 | <.0001 |
| % Symptom 5 (Activities to obtain, use, recover) | 53.6 | 14.5 | <.0001 |
| % Symptom 6 (Reduce other activities) | 21.2 | 3.6 | <.0001 |
| % Symptom 7 (Use despite problems) | 87.5 | 26.6 | <.0001 |
Smoked 50 cigars, a pipe 50 times, used snuff or chewing tobacco 20 times
2.3. Data analysis
Logistic regression analyses with third order polynomial contrasts were used to test the association between the absence of lifetime nicotine dependence and both quantity and years since onset of daily smoking among individuals who reported daily smoking within the past year. Smoking quantity and duration of daily smoking was grouped into categories as described above. The midpoint of each category was used in the logistic regression analyses. Age, gender, ethnicity and race were included as covariates in analyses based on previous findings (Kandel and Chen, 2000). Sample weights were used in each analysis to correct for differences in the probability of selection and to adjust for non-response. Adjustments for design effects were incorporated into the estimation process implemented by SAS survey procedures to generate accurate standard errors. Subsequent analyses contrasted dependent and non-dependent individuals who reporting smoking ≥ 10 cpd and daily smoking onset ≥ 10 years prior.
3.0. Results
In a large, nationally representative sample of past-year daily smokers, 39.4% failed to meet criteria for nicotine dependence within their lifetime. Univariate logistic regression revealed that the probability of remaining never nicotine dependent decreased linearly with increasing past year smoking quantity (β=−0.077, OR: .926, p<.0001) and years since the onset of daily smoking (β= −0.036, OR: .965, p<.05) (Figure 1). Quadratic and cubic effects failed to reach significance and were not included in the multivariate model. Multivariate analyses revealed that the linear relationship between both usual quantity (β= −0.029, OR: .971, p<.0001) and duration of daily smoking (β= −0.028, OR: .972, p<.0001) persisted when simultaneously included in the model and when controlling for demographic variables.
Figure 1.
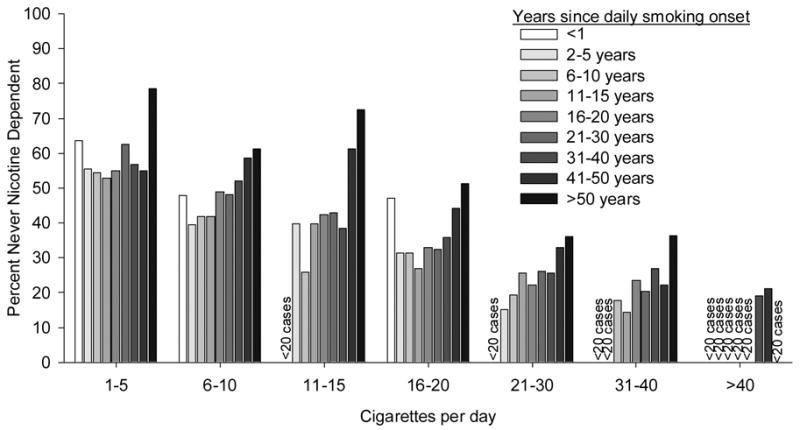
Probability of remaining never DSM-IV nicotine dependent as a function of both years since daily smoking onset and quantity of smoking. Points with fewer than 20 cases have been omitted.
Among individuals who were moderate-to-heavy (i.e., ≥ 10 cpd) smokers and had initiated daily smoking ≥ 10 years prior (n=5281), 37.7% were never nicotine dependent (Table 1). The non-dependent group was disproportionately older, male, African-American and Hispanic. Non-dependent smokers initiated smoking and daily smoking at a later age and were less likely to have ever used other forms of tobacco. The most prevalent dependence criteria met by non-dependent individuals were difficulty cutting down (72.2%) and withdrawal (68.9%); no other criteria exceeded 27% prevalence. These results were largely unchanged when the sample was narrowed to individuals smoking in the past 7 days. 36.5% of past-week daily smokers failed to reach criteria for nicotine dependence.
4.0. Discussion
Conceptualization and measurement of nicotine dependence has been extensively discussed. Numerous measures have been put forward that differ in their theoretical underpinnings, whether they are dichotomous or continuous, and whether they are single or multi-dimensional (Piper et al., 2006). Here, non-dependent cases could have resulted from insensitivity (i.e., false negatives) of the AUDADIS-IV assessment of DSM-IV dependence, due to its dichotomous structure, operationalization of DSM-IV dependence symptoms, method of assessment (e.g., personal interviewing may lead some to under-report symptoms), or retrospective recall bias. Symptom level analyses revealed that the differences between dependent and non-dependent individuals were observed for all seven criteria, but that approximately 70% of individuals experienced two or more symptoms during their lifetime. These data suggest that the differences in dependence may be quantitative not qualitative; that is, the absence of DSM-IV dependence in daily smokers is unlikely to be indicative of absolute resilience to nicotine dependence, but instead a relative resistance. Future research should assess whether individuals failing to meet criteria for DSM-IV nicotine dependence also differ along continuous and/or multi-dimensional measures of dependence.
Unmeasured use/exposure characteristics could further differentiate dependent and non-dependent smokers. Non-dependent, daily smokers may inhale less deeply, absorb less nicotine per cigarette, metabolize nicotine at a different rate, have a greater history of abstinence or systematically overestimate their use. These limitations will be difficult to overcome in cross-sectional epidemiological studies, but can be addressed within the context of longitudinal studies that more intensely assesses smoking trajectories and/or laboratory studies that objectively measure nicotine use/exposure with greater precision.
The interpretation that some smokers may be relatively resistant to developing dependence despite extensive cigarette use is consistent with studies suggesting the relationship between use and dependence is weaker than might be expected and that a substantial proportion of smokers fail to meet dependence criteria (Breslau et al., 2001, Dierker et al., 2006, Kandel and Chen, 2000). Similar animal research has been reported for rats self-administering cocaine; only a portion of rats self-administering cocaine develop signs of “addiction” despite comparable levels of cocaine use (Deroche-Gamonet et al., 2004). Resistance to dependence in established, moderate-to-heavy, daily smokers would suggest that other factor(s) besides extensive nicotine use may be necessary for dependence to occur. An example of a potential co-factor is depression; a history of major depression increases risk of nicotine dependence across all levels of smoking and leads to approximately 100% nicotine dependence amongst the heaviest users (Dierker and Donny, under review). Whether other co-factors can also explain the presence versus absence of dependence despite extensive use requires further study.
Nearly 20 years ago, Shiffman and colleagues (Shiffman, 1989) demonstrated that a small (~5%) subgroup of smokers maintained relatively low levels of use (≥5 cpd) and did not develop nicotine dependence. The current observation suggests that a relatively large portion of individuals who smoke much more intensely may also fail to develop DSM-IV nicotine dependence. It is important to note that from a public health perspective, both dependent and non-dependent daily smokers are an important target for clinical intervention as both engage in a behavior with grave health consequences. The existence of a relatively large population of non-dependent, heavy, long-term, daily smokers presents a challenge for comprehensive theories of nicotine dependence which must account for both risk for and resistance to dependence.
Supplementary Material
Acknowledgments
The National Epidemiologic Survey of Alcohol and Related Conditions (NESARC) was designed and conducted by the National Institute on Alcoholism and Alcohol Abuse (NIAAA). Data analysis was supported by grant K01 DA15454 from the National Institute of Drug Abuse (Dierker) and an Investigator Award from the Patrick & Catherine Weldon Donaghue Medical Research Foundation (Dierker).
Footnotes
Supplementary material relevant to the methods used in the study described here can be found by accessing the online version of this paper at http://dx.doi.org by entering doi: 10.1016/j.drugalcdep.2006.11.019
Specific nicotine dependence questions used in the NESARC are provided as supplementary material on the online version of this paper at http://dx.doi.org by entering doi: 10.1016/j.drugalcdep.2006.11.019
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
References
- Balfour DJ. The neurobiology of tobacco dependence: a preclinical perspective on the role of the dopamine projections to the nucleus accumbens [corrected] Nicotine Tob Res. 2004;6:899–912. doi: 10.1080/14622200412331324965. [DOI] [PubMed] [Google Scholar]
- Breslau N, Johnson EO, Hiripi E, Kessler R. Nicotine dependence in the United States: prevalence, trends, and smoking persistence. Arch Gen Psychiatry. 2001;58:810–6. doi: 10.1001/archpsyc.58.9.810. [DOI] [PubMed] [Google Scholar]
- Caggiula AR, Donny EC, Chaudhri N, Perkins KA, Evans-Martin FF, Sved AF. Importance of nonpharmacological factors in nicotine self-administration. Physiol Behav. 2002;77:683–7. doi: 10.1016/s0031-9384(02)00918-6. [DOI] [PubMed] [Google Scholar]
- Deroche-Gamonet V, Belin D, Piazza PV. Evidence for addiction-like behavior in the rat. Science. 2004;305:1014–7. doi: 10.1126/science.1099020. [DOI] [PubMed] [Google Scholar]
- Dierker LC, Donny E, Tiffany S, Colby SM, Perrine N, Clayton RR. The association between cigarette smoking and DSM-IV nicotine dependence among first year college students. Drug & Alcohol Dependence. 2006 doi: 10.1016/j.drugalcdep.2006.05.025. [DOI] [PubMed] [Google Scholar]
- Grant BF, Dawson DA, Stinson FS, Chou PS, Kay W, Pickering R. The Alcohol Use Disorder and Associated Disabilities Interview Schedule-IV (AUDADIS-IV): reliability of alcohol consumption, tobacco use, family history of depression and psychiatric diagnostic modules in a general population sample. Drug & Alcohol Dependence. 2003;71:7–16. doi: 10.1016/s0376-8716(03)00070-x. [DOI] [PubMed] [Google Scholar]
- Grant BF, Hasin DS, Chou SP, Stinson FS, Dawson DA. Nicotine dependence and psychiatric disorders in the United States: results from the national epidemiologic survey on alcohol and related conditions. Arch Gen Psychiatry. 2004a;61:1107–15. doi: 10.1001/archpsyc.61.11.1107. [DOI] [PubMed] [Google Scholar]
- Grant BF, Stinson FS, Dawson DA, Chou SP, Ruan WJ, Pickering RP. Co-occurrence of 12-month alcohol and drug use disorders and personality disorders in the United States: results from the National Epidemiologic Survey on Alcohol and Related Conditions. Arch Gen Psychiatry. 2004b;61:361–8. doi: 10.1001/archpsyc.61.4.361. [DOI] [PubMed] [Google Scholar]
- Kandel DB, Chen K. Extent of smoking and nicotine dependence in the United States: 1991–1993. Nicotine Tob Res. 2000;2:263–74. doi: 10.1080/14622200050147538. [DOI] [PubMed] [Google Scholar]
- Petry NM, Stinson FS, Grant BF. Comorbidity of DSM-IV pathological gambling and other psychiatric disorders: results from the National Epidemiologic Survey on Alcohol and Related Conditions. J Clin Psychiatry. 2005;66(5):564–74. doi: 10.4088/jcp.v66n0504. [DOI] [PubMed] [Google Scholar]
- Piper ME, McCarthy DE, Baker TB. Assessing tobacco dependence: a guide to measure evaluation and selection. Nicotine Tob Res. 2006;8:339–51. doi: 10.1080/14622200600672765. [DOI] [PubMed] [Google Scholar]
- Sledjeski EM, Dierker LC, Costello D, Shiffman S, Donny E, Flay BR Tobacco Etiology Research Network. Predictive validity of four nicotine dependence measures in a college sample. Drug & Alcohol Dependence. 2006 doi: 10.1016/j.drugalcdep.2006.07.005. [DOI] [PubMed] [Google Scholar]
- Shiffman S. Tobacco “chippers”--individual differences in tobacco dependence. Psychopharmacology. 1989;97:539–47. doi: 10.1007/BF00439561. [DOI] [PubMed] [Google Scholar]
- Tiffany ST. A cognitive model of drug urges and drug-use behavior: role of automatic and nonautomatic processes. Psychol Rev. 1990;97:147–68. doi: 10.1037/0033-295x.97.2.147. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.