

Abstract
Objectives. We sought to identify prospective predictors of long-term abstinence versus relapse among individuals who quit smoking as young adults.
Methods. Participants from an ongoing longitudinal study of smoking who had quit for at least 1 year between the ages of 18 and 24 years (n=327) were divided into those who later reported not smoking for more than 5 years (long-term abstinence) or reported current smoking, defined as smoking at least monthly (relapse). Logistic regression was used to examine odds ratios (ORs) of prospective predictors of long-term abstinence versus relapse.
Results. Overall, 67% of participants maintained long-term abstinence and 33% relapsed. The strongest predictor of avoiding relapse was marrying a nonsmoker (adjusted OR [AOR]=0.07; 95% confidence interval [CI]=0.03, 0.21). Other predictors included making 1 lifetime quit attempt (AOR=0.13; 95% CI=0.04, 0.44), having as a young adult only 1 parent who smoked (AOR=0.23; 95% CI=0.06, 0.93), and working in a completely smoke-free building (AOR=0.13; 95% CI=0.03, 0.58).
Conclusions. The factors related to smoking in the social environment played the largest role in predicting long-term abstinence versus relapse.
The recent increase in smoking among young adults in the United States, especially during the 1990s, is a major public health concern.1 An estimated 11 million young adults in the United States smoke,2 and most want to quit.3–5 Thus, there is a need for a thorough understanding of the factors that promote successful smoking cessation for those aged 18 to 25 years (young adults). Previous studies have reported predictors of cessation among young adults,4–10 but there is a lack of consensus about what factors predict cessation in this age group. Moreover, there is no information in the published literature about what predicts long-term success of quitting as a young adult versus relapsing to smoking later in life.
We selected participants from an ongoing longitudinal study of the natural history of cigarette smoking who had quit smoking as young adults to identify prospective predictors of maintaining long-term abstinence versus relapsing. We examined demographic factors and predictor variables derived from standard cognitive social psychological models of behavior change (e.g., social cognitive theory,11 the theory of planned behavior,12 and the health belief model13) in 4 categories: smoking-related beliefs, smoking-related behaviors, acquisition of adult roles, and smoking in the social environment.
Smoking-related beliefs and behaviors may play a role in predicting successful cessation among young adults. Previous studies have identified perceived likelihood to continue smoking6,9 and valuing a healthy lifestyle6 as the factors associated with cessation. Smoking-related behaviors such as heavy smoking and nicotine dependence were observed in young adult smokers who were less likely to quit.6,7 Also, although 1 study identified age of onset of smoking as a significant predictor of cessation,7 another did not.6 Accordingly, our study examined personally relevant beliefs about psychological and health consequences of smoking and generalized beliefs about the negative health effects of smoking. For smoking-related behaviors, we assessed greatest number of cigarettes ever smoked, smoking onset, and age of quitting during young adulthood as predictors of maintaining long-term abstinence versus relapsing.
The acquisition of adult roles is another important factor that may influence cessation success. For example, young adults who get married are more likely to quit smoking.10,14 What may be even more important, however, is formal marriage to a nonsmoker, because studies have reported that marriage itself or cohabitating with a nonsmoker did not have an association with smoking cessation, but marrying a nonsmoker facilitated quitting.5,6,8 There is consensus in the literature that living with children is not associated with short-term cessation success.5,6,8,10 Two studies found that those who were employed were more successful at quitting,6,10 whereas another found no association with employment.8 We tested the influence of taking on adult roles on long-term cessation success by including marriage experience and having children as predictor variables.
Finally, the social environment has consistently been shown to correlate strongly with cessation during young adulthood. Smokers were less likely to quit if they perceived a higher prevalence of smoking6 and if they had greater exposure to peers who smoked.5,6,8,9 Restrictions on smoking in the workplace have also been associated with cessation,15,16 but no study has focused specifically on the effect of smoke-free workplace policies on quitting among young adult smokers. In addition, previous research has examined the effect of parental smoking, which could indicate genetic as well as environmental risk, on cessation. In 2 studies of cessation during young adulthood, parental smoking had no relation with cessation.6,8 However, other research has found that individuals whose parents smoked were less likely to quit smoking.10 We examined perceived prevalence of smoking; smoking among friends, parents, and spouses; and smoking in the workplace as predictors.
Although factors in these 4 conceptual categories have been shown in some studies to be important predictors of cessation for young adults, the previous research relied on relatively short follow-up periods to assess cessation success. We used a longitudinal data set to explore predictors of long-term success of quitting during young adulthood. A better understanding of the factors that are associated with relapse later in life provides much-needed guidance on how to prevent relapse among young adults who have quit smoking.
METHODS
Sample
Between 1980 and 1983, all consenting 6th to 12th graders in an Indiana county school system completed up to 4 annual surveys (a total sample of 8556 students were assessed at least once). Follow-up surveys were conducted in 1987 (n = 6234; retention rate = 73%), 1994 (n = 6223; retention rate = 73%), and 1999 (n = 6060; retention rate=71%). In this study, we focused on long-term abstinence from smoking versus smoking relapse among individuals who reported in 1987 or 1994 that they had quit smoking for at least 1 year during young adulthood (between the ages of 18 and 24 years) and who participated in 1999. Of the 509 participants who quit as young adults, 81 did not complete a survey in 1999. An additional 26 participants who completed a survey in 1999 were excluded because of missing data on time since last cigarette, and thus they could not be classified on the outcome variable. Another 75 participants who did not report current smoking were excluded because they had smoked within the past 5 years. Thus, the final sample size was 327 (Figure 1 ▶).
FIGURE 1—
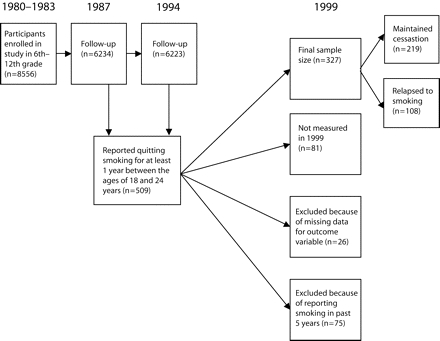
Schematic diagram of study illustrating enrollment, data collection points, loss to follow-up, and outcome.
We found no statistically significant differences in gender, educational attainment, age of last quit attempt during young adulthood, number of lifetime quit attempts, and number of friends who smoked during young adulthood between those who were included in this study and those who were not included. However, more people who were dropped from this study than were included worked at a workplace where they could smoke freely at their immediate workstations (21.5% vs 11.6%). Thus, the results may underestimate the amount of smoking relapse overall. However, given the lack of significant differences in other variables as well as the small magnitude of the difference in workplace smoking, the effect of this difference on the results is likely small.
Measures
The outcome variable for this study was created by dividing participants who reported quitting smoking for at least 1 year between the ages of 18 and 24 years into those who in 1999 reported not smoking for more than 5 years (n = 219) or reported current smoking, defined as smoking cigarettes at least monthly (n = 108).
Categories for predictor variables were created with 2 criteria. First, categories were created to maintain conceptual coherence (e.g., response options that reflected the period of young adulthood). Second, response options were collapsed when the number of cases was too small for the logistic regression analyses.
Demographic characteristics included age in 1999, gender, and educational attainment. For the analyses, 10 categories of educational attainment were collapsed into 3 levels: high school or less, some college, and 4-year college degree or higher.
A 6-item composite variable (α = .84) measured personally relevant beliefs about psychological consequences of smoking (e.g., “If I smoke cigarettes, I will be able to relax.”). A 5-item composite variable (α = .83) measured personally relevant beliefs about health consequences of smoking (e.g., “If I smoke cigarettes, I will get lung cancer.”). A 5-item composite variable (α = .89) measured generalized beliefs about the negative health effects of smoking (e.g., “Smoking cigarettes is OK as long as you don’t smoke too many.”).
Participants reported the greatest number of cigarettes ever smoked per day, subdivided for analyses into less than 1 cigarette a day, 1 to 20 cigarettes a day, and more than 21 cigarettes a day. The number of lifetime quit attempts was subdivided for analyses into 1, 2, or 3 or more. Two smoking-onset variables, the grade at which the first cigarette was tried and the grade at which regular smoking started, were both dichotomized for analyses into adolescent onset (12th grade or before) or postadolescent onset (after 12th grade). Participants reported the age at which they finally quit smoking. Response options that corresponded to young adulthood were 18 to 21 and 22 to 24.
To assess acquisition of adult roles, we created a marriage experience variable from 2 measures: current marital status (in which unmarried included divorced) and ever divorced. The marriage experience variable was then subdivided for analyses into never married, ever divorced or separated, and married and never divorced or separated. Participants also responded to a yes or no question of having children.
In 1987 (mean age of cohort = 20.8; SD = 2.4), to measure smoking in the social environment, participants were asked about their perceived prevalence of smoking (a composite variable of perceived smoking among adult men, adult women, adolescent boys, and adolescent girls), number of biological parents who currently smoked (0 to 2), and number of friends who smoked, dichotomized for analyses into 2 or fewer versus 3 or more. In the 1994 and 1999 data collection waves, participants reported a dichotomous measure of spouse smoking status and the extent of access to smoking at their workplace (“cannot smoke anywhere in the building,” “can smoke in designated areas but not at my own workstation,” and “can smoke freely at my immediate workstation”).
Statistical Analyses
Prior to selecting variables to be submitted to logistic regression analysis, we used the likelihood ratio χ2 test to examine bivariate associations of each variable with the outcome variable. For continuous variables, we centered each variable to reduce mathematically caused multicollinearity17 and checked the assumption of linearity between the logit and each continuous predictor using the Box–Tidwell approach (i.e., an interaction term between each predictor and its natural logarithm was added to the logistic regression model).18 None of the continuous predictors violated the linearity assumption.
After we fit a logistic regression model for each variable to obtain unadjusted odds ratios and 95% confidence intervals, we selected the variables with a bivariate P<0.25 as candidates for the multivariate model.18,19 To minimize the possibility of multicollinearity, we used backward likelihood ratio elimination with a threshold of P < .05 for retention in the model followed by a test for forward selection.18 We added each of the variables not selected for the original multivariate model back into the model 1 at a time and examined changes in the estimated logit coefficients for each of the other predictors in the model. When the change was more than 10%, the tested variable was reincluded.20 Evidence of multicollinearity was not detected among the variables included in the final model when we examined changes in the standard errors of the estimated logit coefficients between the single-variable model and the full model.
To test 2-way interactions among the variables in the final main effects model, we added the interaction terms between all pairs of variables, 1 at a time, to the model containing all the main effects. We were especially interested in the interaction of each predictor with potential moderators such as age and educational attainment. The model was not significantly improved with the addition of any interaction term as assessed by the significance of the change in the −2 log likelihood. We used SAS version 9.1 (SAS Institute Inc, Cary, NC) for the analyses.
RESULTS
Results of logistic regression predicting smoking relapse versus maintenance of abstinence among the longitudinal study cohort (n = 327) who reported that they quit smoking for at least a year between the ages of 18 and 24 years are presented in Table 1 ▶. Of the total cohort, 219 (67%) were long-term abstainers who reported in 1999 that they had not smoked a cigarette within the past 5 years, and 108 (33%) had relapsed and reported that they were currently smoking. In unadjusted logistic models, those who were older, had higher educational attainment, smoked fewer cigarettes per day at their peak of smoking quantity, made just 1 lifetime quit attempt, had 1 or no biological parent who smoked, and had fewer friends who smoked were less likely to relapse into smoking. The odds of relapse into smoking were also lower among those with a nonsmoking spouse, those who could not smoke anywhere in their workplace, and those who were married and who had never been divorced or separated.
TABLE 1—
Predictors of Relapse Into Smoking Among Those Who Quit Smoking During Young Adulthood (Ages 18–24 Years): United States, 1987–1999
| Predictor | Quit During Young Adulthood and Relapsed, % (No./Total) | Bivariate OR (95% CI) | Multivariate Adjusted OR (95% CI) |
| Demographic characteristics | |||
| Agea | . . . | 0.88 (0.80, 0.98)* | 1.03 (0.80, 1.31) |
| Gender | |||
| Women | 31.1 (60/193) | 0.81 (0.51, 1.29) | . . . |
| Men (reference) | 35.8 (48/134) | 1.00 | . . . |
| Educational attainment | |||
| High school diploma or less (reference) | 38.5 (37/96) | 1.00 | 1.00 |
| Some college | 36.0 (40/111) | 0.90 (0.51, 1.58) | 0.70 (0.22, 2.18) |
| Four-year college degree or more | 26.1 (31/119) | 0.56 (0.31, 1.00)* | 0.71 (0.22, 2.31) |
| Smoking-related beliefs | |||
| Personally relevant beliefs about psychological consequences of smoking, measured in 1987a | . . . | 1.16 (0.85, 1.59) | . . . |
| Personally relevant beliefs about health consequences of smoking, measured in 1987a | . . . | 1.17 (0.80, 1.70) | . . . |
| Generalized beliefs about the negative health consequences of smoking, measured in 1987a | . . . | 0.86 (0.62, 1.20) | . . . |
| Smoking-related behaviors | |||
| Greatest no. of cigarettes ever smoked | |||
| < 1 cigarette per day | 10.0 (10/100) | 0.07 (0.03, 0.18)*** | 0.33 (0.05, 2.31) |
| 1–20 cigarettes per day | 38.4 (68/177) | 0.42 (0.22, 0.79)** | 0.73 (0.25, 2.16) |
| ≥ 21 cigarettes per day (reference) | 60.0 (30/50) | 1.00 | 1.00 |
| No. lifetime quit attempts | |||
| 1 | 18.9 (27/143) | 0.18 (0.09, 0.34)*** | 0.13 (0.04, 0.44)*** |
| 2 | 53.6 (30/56) | 0.87 (0.41, 1.82) | 0.50 (0.14, 1.79) |
| ≥ 3 (reference) | 57.1 (32/56) | 1.00 | 1.00 |
| Grade first tried a cigarette | |||
| ≤ 12th (reference) | 35.5 (88/248) | 1.00 | . . . |
| > 12th | 19.4 (6/31) | 0.44 (0.17, 1.10) | . . . |
| Grade first started smoking regularly | |||
| ≤ 12th (reference) | 39.1 (63/161) | 1.00 | . . . |
| > 12th | 25.4 (16/63) | 0.53 (0.28, 1.01) | . . . |
| Age of last quit attempt during young adulthood, y | |||
| 18–21 | 28.3 (43/152) | 0.67 (0.42, 1.07) | 0.68 (0.25, 1.87) |
| 22–24 (reference) | 37.1 (65/175) | 1.00 | 1.00 |
| Acquisition of adult roles | |||
| Marriage experience | |||
| Never married (reference) | 50.0 (27/54) | 1.00 | 1.00 |
| Ever divorced or separated | 41.8 (38/91) | 0.72 (0.36, 1.41) | 0.52 (0.11, 2.38) |
| Married and never divorced or separated | 22.6 (38/168) | 0.29 (0.15, 0.56)*** | 0.38 (0.10, 1.51) |
| Have kids | |||
| Yes | 31.2 (69/221) | 0.78 (0.48, 1.27) | . . . |
| No (reference) | 36.8 (39/106) | 1.00 | . . . |
| Smoking in the social environment | |||
| Perceived prevalence of smoking measured in 1987a | . . . | 1.01 (0.99, 1.02) | . . . |
| No. biological parents who smoked in 1987 | |||
| 0 | 33.1 (55/166) | 0.42 (0.20, 0.87)* | 0.72 (0.20, 2.55) |
| 1 | 22.9 (22/96) | 0.25 (0.11, 0.56)*** | 0.23 (0.06, 0.93)* |
| 2 (reference) | 54.1 (20/37) | 1.00 | 1.00 |
| No. friends who smoked in 1987 | |||
| ≤2 (reference) | 26.0 (45/173) | 1.00 | 1.00 |
| ≥3 | 41.5 (51/123) | 2.02 (1.23, 3.30)** | 1.15 (0.46, 2.90) |
| Spouse smoking status | |||
| Smoking (reference) | 64.9 (48/74) | 1.00 | 1.00 |
| Nonsmoking | 17.6 (32/182) | 0.12 (0.06, 0.21)*** | 0.07 (0.03, 0.21)*** |
| Extent of access to smoking at workplace | |||
| Cannot smoke anywhere in building | 23.9 (42/176) | 0.33 (0.16, 0.70)** | 0.13 (0.03, 0.58)** |
| Can smoke in designated areas | 45.1 (41/91) | 0.87 (0.40, 1.90) | 0.23 (0.05, 1.17) |
| Can smoke freely at own immediate workstation (reference) | 48.6 (17/35) | 1.00 | 1.00 |
Note. OR = odds ratio; CI = confidence interval. Frequencies within categories varied because missing data resulted in deletion of the entire case.
aCentered continuous variable (obtained by subtracting the mean).
* P ≤ .05; **P ≤.01; ***P ≤.001.
Among the 18 demographic variables and predictor variables from the 4 conceptual categories that were measured, 10 were retained in the final multivariate model, as shown in Table 1 ▶. The Hosmer-Lemeshow goodness-of-fit statistic for the multivariate model was 3.199 (df = 8; P = .921), indicating a good fit of the model. The results of the multivariate analysis indicated that, among the 4 groups of predictor variables (smoking-related beliefs, smoking-related behaviors, acquisition of adult roles, and smoking in the social environment), the factors in the social environment were the best predictors of smoking relapse versus long-term abstinence. The number of biological parents who smoked, spouse smoking status, extent of access to smoking at a workplace, and number of lifetime quit attempts were independent predictors of smoking relapse versus long-term abstinence, after adjusting for all the other variables in the model.
DISCUSSION
Previous studies of prospective predictors of cessation among young adults used relatively short follow-up times and therefore short periods of abstinence, usually 6 months or 1 year, to define smoking cessation. By contrast, our study defined successful smoking cessation as abstinence from smoking for at least 5 years, enabling us to examine long-term success of quitting during young adulthood. The first finding of note was that young adults who successfully quit smoking for at least 1 year had a good chance of remaining abstinent in the long term. That is, two thirds of these young adult exsmokers were able to maintain long-term abstinence from smoking 5 or more years later. This illustrates the usefulness of promoting smoking cessation in young adulthood.
We identified several variables that contributed to this long-term abstinence. The variables having to do with smoking in the social environment seemed to play the largest role in predicting whether individuals in this study would relapse into smoking or stay abstinent. Other researchers have also emphasized the importance of background conditions or situational factors rather than individual traits in predicting smoking relapse.21 In the unadjusted model, those who, as young adults, had 1 or no parent who smoked were less likely to relapse into smoking than were those who had 2 parents who smoked. Parental smoking has previously been linked with persistence of offspring smoking and is likely to index both genetic and environmental influences.22
Another significant predictor from the social environment was the extent of access to smoking in the workplace. It is important to note that only those who worked in completely smoke-free buildings were less likely to relapse into smoking. The finding that working where smoking was allowed in designated areas failed to predict long-term abstinence versus smoking relapse in both the unadjusted and adjusted models suggests that smoke-free workplace policies should be comprehensive in nature and prohibit smoking throughout the workplace to help young adults maintain long-term smoking cessation. Another policy-based intervention that may have a similar effect and therefore warrants future study is the implementation of smoke-free policies on college campuses. In addition to promoting smoking cessation, these smoke-free policy interventions may reduce cigarette consumption; prevent some light and intermittent smokers from becoming regular, heavy smokers; and prevent some young adults from initiating smoking.
Social role influences, such as getting married, are associated with decreases in other forms of substance use during young adulthood.14 However, the picture is less clear for smoking. In the current data, stable marriage (never being divorced) was associated with long-term abstinence in the unadjusted model but did not exert a unique effect in the multivariate adjusted model. Weaker marriage effects on smoking than on other forms of substance use might be attributable to the fact that cigarettes are legal for this age group and do not produce intoxication, so there is less conflict between smoking and the demands of marriage. Marriage alone may not be sufficient to promote long-term success in quitting smoking during young adulthood. However, the strongest independent predictor of maintaining long-term abstinence in the current data was being married to a non-smoker. This is consistent with at least 1 other study’s findings.8 Thus, there appear to be 2 factors related to marriage that are important for long-term abstinence after quitting. First, the stability that accompanies formal, lasting marriages appears to aid in quitting smoking and staying abstinent. Second, marrying a nonsmoker may aid in cessation and long-term abstinence for reasons that include the introduction of a nonsmoking role model into the former smoker’s life, encouragement from the nonsmoking spouse to not smoke, and the desire to protect family members from environmental tobacco smoke exposure.
Although previous studies have reported that those living with children are less successful at quitting smoking,5,6,8 we found that living with children was not significant in either direction for long-term smoking cessation. Even though having children does not seem to lead to smoking cessation, it does present an opportunity for young adult parents to receive public health education about the negative health consequences of environmental tobacco smoke exposure. If young adult parents are educated about environmental tobacco smoke, they may be more likely to quit smoking to avoid exposing their young children.23
Of the smoking-related behaviors examined in this study, only number of lifetime quit attempts was an independent predictor of relapse. Individuals who quit smoking the first time they tried to quit smoking were significantly less likely to relapse into smoking than were those who made 3 or more quit attempts. These individuals who quit smoking the first time they attempted to quit may be smokers who were less addicted to nicotine or who were particularly committed to maintaining smoking cessation. There was no difference between those who made 2 quit attempts and those who made 3 or more quit attempts. For individuals who require multiple cessation attempts, it is important that cessation interventions support their motivation to continue trying despite failing to quit in the past. Because these individuals may label themselves as failures after 1 failed quit attempt, they may require extra encouragement to continue trying.
Although other studies have reported that young adults were less likely to quit when exposed to smoking peers,5,8,9 we did not find in this study that the number of friends who smoked was an independent predictor of relapse into smoking later in life. Similarly, none of the smoking-related belief measures predicted smoking relapse. However, having few friends who smoked and having negative beliefs about smoking may have been motivating influences to quit smoking as a young adult. Then, later in adulthood, other factors, such as adult roles and environmental influences, may have played a relatively more important role in maintaining, as opposed to initiating, smoking abstinence.
The findings of this study are subject to limitations. First, the community from which this representative sample was drawn is predominantly White and well educated, so some caution is warranted in generalization. Second, potentially important predictor variables not included in this study are employment status and assistance with cessation, because of lack of variability in the sample, and nicotine addiction, because of lack of data. Third, variables that were significant in the unadjusted model but not in the multivariate adjusted model may have been mediated by other factors in the multivariate model, but formal mediational analyses are beyond the scope of this paper. Fourth, the relatively small sample size might have limited the statistical power of our analyses.
Despite these limitations, this study provides additional information about the factors affecting cessation during young adulthood and contributes further to the literature by assessing long-term abstinence versus smoking relapse, the outcome that ultimately holds the most interest for public health practitioners and policymakers. To help young adults stop smoking permanently, it is important to understand the key behaviors of young adults that can be influenced and the conditions in the social environment that can be changed and to use these as targets for public health intervention. The current data suggest that long-term maintenance of abstinence is promoted most by antismoking influences in the social environment such as a nonsmoking spouse and comprehensive smoke-free work-place policies.
Acknowledgments
This research was supported by the National Institute on Drug Abuse (grant DA13555).
Human Participant Protection This study was approved by Indiana University’s human subjects committee.
Peer Reviewed
Contributors: J. T. Macy originated the study and led the writing. D.-C. Seo conducted the statistical analyses. All authors helped to conceptualize ideas, interpret findings, and write and review drafts of the article.
References
- 1.Johnston LD, O’Malley PM, Bachman JG. Monitoring the Future National Survey Results on Drug Use, 1975–2000. Volume II: College Students and Adults Ages 19–40. Bethesda, Md: National Institute on Drug Abuse; 2001. NIH Publication 01–4925.
- 2.Summary of Findings from the 2000 National Household Survey on Drug Abuse. Rockville, Md: Office of Applied Studies, Substance Abuse and Mental Health Services Administration; September 2001. SMA 01–3549.
- 3.Everett SA, Husten CG, Kann LK, Warren CW, Sharp D, Crossett L. Smoking initiation and smoking patterns among US college students. J Am Coll Health. 1999;48:55–60. [DOI] [PubMed] [Google Scholar]
- 4.Pirie PL, Murray DM, Luepker RV. Gender differences in cigarette smoking and quitting in a cohort of young adults. Am J Public Health. 1991;81:324–327. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Tucker JS, Ellickson PL, Orlando M, Klein DJ. Predictors of attempted quitting and cessation among young adult smokers. Prev Med. 2005;41:554–561. [DOI] [PubMed] [Google Scholar]
- 6.Rose JS, Chassin L, Presson CC, Sherman SJ. Prospective predictors of quit attempts and smoking cessation in young adults. Health Psychol. 1996;15: 261–268. [DOI] [PubMed] [Google Scholar]
- 7.Breslau N, Peterson EL. Smoking cessation in young adults: age at initiation of cigarette smoking and other suspected influences. Am J Public Health. 1996; 86:214–220. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Chen P-H, White HR, Pandina RJ. Predictors of smoking cessation from adolescence into young adulthood. Addict Behav. 2001;26:517–529. [DOI] [PubMed] [Google Scholar]
- 9.Tucker JS, Ellickson PL, Klein DJ. Smoking cessation during the transition from adolescence to young adulthood. Nicotine Tob Res. 2002;4:321–332. [DOI] [PubMed] [Google Scholar]
- 10.Chassin L, Presson CC, Rose JS, Sherman SJ. The natural history of cigarette smoking from adolescence to adulthood: demographic predictors of continuity and change. Health Psychol. 1996;15:478–484. [DOI] [PubMed] [Google Scholar]
- 11.Bandura A. Social cognitive theory: an agentic perspective. Psychol Rev. 2001;52:1–26. [DOI] [PubMed] [Google Scholar]
- 12.Ajzen I. The theory of planned behavior. Organ Behav Hum Decis Process. 1991;50:179–211. [Google Scholar]
- 13.Janz NK, Becker MH. The health belief model: a decade later. Health Educ Q. 1984;11:1–47. [DOI] [PubMed] [Google Scholar]
- 14.Bachman J, Wadsworth K, O’Malley P, Johnston L, Shulenberg J. Smoking, Drinking, and Drug Use in Young Adulthood: The Impacts of New Freedoms and New Responsibilities. Hillsdale, NJ: Erlbaum; 1997.
- 15.Bauer JE, Hyland A, Li Q, Steger C, Cummings MK. A longitudinal assessment of the impact of smoke-free worksite policies on tobacco use. Am J Public Health. 2005;95:1024–1029. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Fichtenberg CM, Glantz SA. Effect of smoke-free workplaces on smoking behaviour: systematic review. BMJ. 2002;325:188–194. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Tabachnick BG, Fidell LS. Using Multivariate Statistics. 5th ed. Boston, Mass: Pearson Education; 2007.
- 18.Hosmer DW, Lemeshow S. Applied Logistic Regression. 2nd ed. New York, NY: John Wiley & Sons; 2000.
- 19.Mickey J, Greenland S. A study of the impact of confounder–selection criteria on effect estimation. Am J Epidemiol. 1989;129:125–137. [DOI] [PubMed] [Google Scholar]
- 20.Tindle HA, Rigotti NA, Davis RB, Barbeau EM, Kawachi I, Shiffman S. Cessation among smokers of light cigarettes: results from the 2000 National Health Interview Survey. Am J Public Health. 2006;96: 1498–1504. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Shiffman S. Dynamic influences on smoking relapse process. J Pers. 2005;73:1715–1748. [DOI] [PubMed] [Google Scholar]
- 22.White VM, Hopper JL, Wearing AJ, Hill DJ. The role of genes in tobacco smoking during adolescence and young adulthood: a multivariate behaviour genetic investigation. Addiction. 2003;98:1087–1100. [DOI] [PubMed] [Google Scholar]
- 23.Ling PM, Glantz SA. Why and how the tobacco industry sells cigarettes to young adults: evidence from industry documents. Am J Public Health. 2002;92: 908–916. [DOI] [PMC free article] [PubMed] [Google Scholar]