

Abstract
PURPOSE
Primary intraocular lymphoma (PIOL) is a diffuse large B cell lymphoma that initially infiltrates the retina, vitreous, or optic nerve head, with or without central nervous system involvement. This study examined the expression of the bcl-2 t(14;18) translocation, the bcl-10 gene, and high expression of bcl-6 mRNA in PIOL cells.
METHODS
Microdissection and PCR analysis were used to examine vitreous specimens in patients with PIOL for the presence of bcl-2 t(14;18) translocations, the bcl-10 gene, and expression of bcl-6 mRNA. A medical record review was also conducted to determine whether the bcl-2 t(14;18) translocation correlated with prognosis.
RESULTS
Forty of 72 (55%) PIOL patients expressed the bcl-2 t(14;18) translocation at the major breakpoint region. Fifteen of 68 (22%) patients expressed the translocation at the minor cluster region. The bcl-10 gene was detected in 6 of 26 (23%) patients, whereas 4 of 4 (100%) PIOL patients expressed higher levels of bcl-6 mRNA compared with inflammatory lymphocytes. An analysis of clinical outcome in 23 PIOL patients revealed no significant association between bcl-2 t(14;18) translocations and survival or relapse. However, patients with the translocation were significantly younger.
CONCLUSIONS
PIOL has unique molecular patterns of bcl-2, bcl-10, and bcl-6 when compared with other systemic lympho-mas. This study lays the foundation for future studies aimed at exploring the genotypic classification of PIOL based on the quantitative molecular framework of gene expression profil-ing, with the goal of providing useful adjuncts to the pathologic diagnosis of this complex disease.
Primary intraocular lymphoma (PIOL) is a subset of central nervous system lymphoma (PCNSL) in which ma- lignant lymphoid cells invade the retina, vitreous, or optic nerve head.1,2 PIOL is usually a diffuse large B cell lymphoma (DLBCL) but occasionally presents as a T cell lymphoma.3,4 Sixty percent to 80% of patients with PIOL eventually have brain involvement, whereas 15% to 25% of PCNSL patients have ocular involvement.5–9 Because the clinical presentation often mimics uveitis, PIOL is considered a masquerade syndrome, and diagnosis requires pathologic confirmation, usually by vitrectomy.4,8–13
Although cancer prognosis has historically been based on clinical and laboratory findings, analysis of the expression of various gene translocations and proteins has burgeoned as a method for determining prognosis. This study examined the involvement of three genes—bcl-2, bcl-6, and bcl-10—in PIOL cells. Bcl-2 is an antiapoptotic molecule whose gene is located on chromosome 18.14 The immunoglobulin heavy chain (IgH) gene is located on chromosome 14. The bcl-2 t(14;18) translocation brings the bcl-2 gene under the control of the IgH enhancer, resulting in deregulated bcl-2 expression.15 Most (60%) translocations occur at the major breakpoint region (Mbr) located within exon 3, whereas 10% to 25% of translocations occur at the minor cluster region (mcr) located 20 kb downstream of the Mbr.16–18 On chromosome 14, the translocation occurs within the joining region of the IgH gene.16,19,20 Bcl-10 is a proapoptotic molecule with a caspase-recruitment domain. It is located at chromosome 1p22 and is involved in the t(1;14)(p22;q32) translocation typically associated with mucosa-associated lymphoid tissue (MALT) lymphoma.21 However, Bcl-10 is also seen in 24.6% to 49.2% of patients with DLBCL.22 Bcl-6, whose gene is located on chromosome 3q27, is a zinc finger transcriptional repressor and is involved in apoptosis and cell growth and differentiation.23
This study also examined the role of the bcl-2 t(14;18) translocation in PIOL survival and relapse. Because PIOL typically presents as a subtype of PCNSL, we hypothesized that PIOL cells express the bcl-2 t(14;18) translocation and the bcl-6 and bcl-10 genes in a pattern similar to that seen in DLBCL and PCNSL. However, we did not predict that the bcl-2 t(14;18) translocation correlates with PIOL prognosis, which is more likely related to age, CNS involvement, treatment selection, and genotypic subtypes.
MATERIALS AND METHODS
This study followed the tenets of the Declaration of Helsinki and was approved by the National Eye Institute Institutional Review Boards for human subjects. Informed consent was obtained from all patients.
Ocular Specimens
Vitrectomy specimens from 72 patients with diagnoses of PIOL were used for the microdissection and PCR analyses. Diagnosis was based on clinical findings and cytopathology identification of B lymphoma cells, as described previously.24 In addition, infiltrating lymphocytes from four uveitic eyes were collected.
Microdissection of Ocular Specimens
Microdissection was performed on the Giemsa-stained cytology slides of the vitreous specimens either manually or with the use of laser capture microscopy (PixCell II; Arcturus, Mountain View, CA), as described previously.25,26 For PCR analysis, at least 15 atypical cells were required. All captured PIOL cells were immediately placed in a single-step DNA extraction buffer containing 0.5 mg/mL proteinase K for 24 hours, which provides the starting point for PCR amplification.
Detection of the bcl-2 t(14;18) Translocation
To detect the bcl-2 t(14;18) translocation, the PCR-amplifiable mixture contained 1 μ L microdissected DNA; 4 pmol 32P-labeled sense primer for the Mbr (5′ -TTA GAG AGT TGC TTT ACG TGG CCT-3′) or for the mcr (5′-GAC TCC TTT ACG TGC TGG TAC C-3′); 4 pmol antisense primer CFW1 (5′-ACC TGA GGA GAC GGT GAC CAG GGT-3′); 4 nmol dNTP; 25 nmol MgCl2; and 0.5 U AmpliTaq Gold DNA polymerase (AmpliTaq Gold Enzyme; Applied Biosystems, Foster City, CA) in a final volume of 10 μL.27 The cycling parameter for Mbr was as follows: initial incubation at 94°C for 9 minutes; 40 cycles of 94°C for 45 seconds, 55°C for 2 minutes, and 72°C for 2 minutes; and a final incubation at 72°C for 7 minutes. The cycling parameter for mcr was as follows: initial incubation at 94°C for 9 minutes; 35 cycles of 94°C for 1 minute, 55°C for 2 minutes, and 72°C for 2 minutes; and a final incubation of 72°C for 7 minutes. PCR products for the bcl-2 Mbr and mcr analyses were separated on 3% agarose gels and visualized with autoradiography. Mbr was analyzed in 72 samples, and mcr was analyzed in 68 samples. Limited sample availability resulted in the difference in sample size for the mcr analysis.
Detection of the bcl-10 Gene
To detect the bcl-10 gene, the PCR-amplifiable mixture contained 1 μL microdissected DNA; 32P-labeled primers for the second exon of the bcl-10 gene (sense, 5′-AGA CTG CCA ACT AAT AGT CAC GT-3′; antisense, 5′-AAG TAG TCT AAC AAT TTT CCA GCC C-3′); 4 nmol dNTP; 25 nmol MgCl2; and 0.5 U AmpliTaq Gold Enzyme in a final volume of 10 μL. The cycling parameter was as follows: initial incubation at 94°C for 9 minutes; 35 cycles of 94°C for 30 seconds, 60°C for 45 seconds, and 72°C for 45 seconds; and a final incubation at 72°C for 7 minutes. The PCR product was separated on 15% polyacrylamide gels and visualized with phospho imaging. The bcl-10 analysis was performed on 26 samples.
Detection of bcl-6 mRNA Expression
RNA was extracted from microdissected PIOL and uveitis cells (Pico-Pure RNA isolation kit; Arcturus). PCR was performed on the cDNA complement (SuperScript RNase H- Reverse Transcriptase kit; Invitrogen, Carlsbad, CA). Primers were used for bcl-6 and 18S, a housekeeping gene. The PCR-amplifiable mixture contained cDNA, 4 pmol 32P-labeled bcl-6 primer pairs (sense, 5′-AGC AAG GCA TTG GTG AAG ACA-3′; antisense, 5′-ATG GCG GGT GAA CTG GAT AC-3′) or 4 pmol 32 P-labeled 18S primer pairs (sense, 5′-AGG AAT TGA CGG AAG GGC AC-3′; antisense, 5′-GGA CAT CTA AGG GCA TCA CA-3′), 4 nmol dNTP, 25 nmol MgCl2, and 0.5 U AmpliTaq Gold Enzyme in a final volume of 10 μL. The cycling parameter for bcl-6 was as follows: initial incubation at 94°C for 9 minutes; 40 cycles of 94°C for 1 minute, 60.5°C for 1 minute, and 72°C for 2 minutes; and a final incubation at 72°C for 7 minutes. The cycling parameter for 18S was as follows: initial incubation at 94°C for 9 minutes; 40 cycles of 94°C for 1 minute, 59°C for 1 minute, and 72°C for 2 minutes; and a final incubation at 72°C for 10 minutes. PCR products were separated on 15% polyacrylamide gels and semiquantitated with phospho imaging. Expression of bcl-6 was determined by taking the ratio of bcl-6:18S expression with 1.0 used as the cutoff for normal bcl-6 expression. Only four PIOL samples could be studied for RNA analysis.
Controls
To ensure the reliability of the PCR assays, we included a positive control (1 μL positive DNA) and a negative control (diethylpyrocarbonate-treated water) in all reactions.
Medical Record Collection and Chart Review
From 1991 to 2003, the National Eye Institute received ocular specimens from 72 patients with diagnoses of PIOL. Patients were from the United States and other countries. The following information was obtained: demographics (age, sex, race); clinical findings at initial presentation (visual acuity, anterior chamber cell and flare, vitreous cells and haze, retinal examination, and fluorescein angiogram); results of diagnostic tests (neuroimaging, cerebrospinal fluid analysis, bone marrow biopsy, and ocular tissue biopsy); date of diagnosis; basis of diagnosis (tissue specimen); initial treatment regimens (chemotherapy and radiation); length of remission, if any; time to recurrence, if any; therapeutic regimens used for recurrence; and date and cause of death. Complete clinical data were available for 23 patients.
Statistical Analysis of the bcl-2 t(14;18) Translocation and Disease Prognosis
To determine the relationship between detection of the bcl-2 t(14;18) translocation and PIOL prognosis, several statistical analyses were performed. Outcome variables of interest included duration of survival and relapse. Duration of survival was defined as the time interval from the date of diagnosis to the date of death. Censoring was used for patients still alive at the time this analysis was performed. Relapse was defined as the requirement of more than one course of treatment (chemotherapy, radiation therapy) for disease remission. First, univariate analysis was performed. Age was examined with a two-sided t test, and survival was examined with the log-rank test. Because of censoring in the survival data, which biases the results of univariate analysis, it was necessary to use Cox regression analysis. After adjusting for age, analysis of survival was made from two-sided Wald statistics from Cox regression with age as a covariate. Relapse was determined by two-sided Wald statistics from the logistic regression analysis with age as a covariate.
RESULTS
Lymphoma cells were identified in the vitreous specimens of all 72 patients with PIOL. PIOL cells (Fig. 1), characterized by scanty basophilic cytoplasm, large nuclei, and prominent nucleoli, were selectively microdissected from the slides of vitreous specimens. DNA was then extracted from these cells. PCR analysis was performed to detect the presence of the bcl-2 t(14;18) translocation and the bcl-10 gene. Seventy-two vitreous specimens were examined for expression of the bcl-2 t(14;18) translocation at the Mbr, and 68 specimens were examined for the bcl-2 t(14;18) translocation at the mcr. The Mbr translocation was detected in 40 of 72 (55%) specimens, and the mcr was detected in 15 of 68 (22%) specimens (Fig. 2). It should be noted that 14 of 15 of these specimens were also positive at the mbr region, indicating overlap of the breakpoint regions.
FIGURE 1. Typical cytology of a PIOL cell.

A characteristic PIOL cell (arrow) from the vitreous with basophilic cytoplasm and large prominent irregular nuclei.
FIGURE 2.
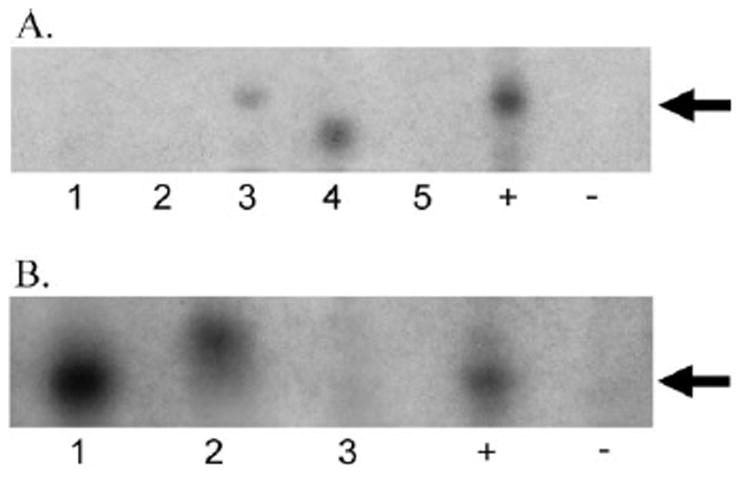
(A) Sample gel of PCR analysis for the bcl-2 t(14;18) translocation at the Mbr. PCR amplification of DNA from microdissected cells from vitreous specimens of PIOL patients using primers for the bcl-2 t(14;18) translocation at the Mbr. Lanes 1 to 5, PIOL samples; +, positive control; −, negative control. Seventy-two vitreous specimens were examined; 40 (55%) were positive. (B) Sample gel of PCR analysis for the bcl-2 t(14;18) translocation at the mcr. PCR amplification of DNA from microdissected cells from vitreous specimens of PIOL patients using primers for the bcl-2 t(14;18) translocation at the mcr. Lanes 1 to 3, PIOL samples; +, positive control; −, negative control. Sixty-eight vitreous specimens were examined; 15 (22%) were positive. In both (A) and (B), differences in migration through the gel were caused by variability where the translocation could occur in the JH region of the IgH gene, resulting in different sizes of amplified product.
Because of the quantity of material available of each sample, sufficient DNA was available in only 26 patients for further molecular evaluation. The bcl-10 gene was detected in 6 of 26 (23%) patients (Fig. 3). Four of these six patients were also positive for the bcl-2 t(14;18) translocation.
FIGURE 3. Sample gel of PCR analysis for the bcl-10 gene.
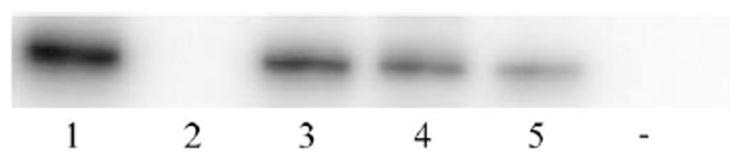
PCR amplification of DNA from microdissected cells from vitreous specimens of PIOL patients using primers for the bcl-10 gene. Lanes 1 to 5, PIOL samples; −, negative control. Twenty-six vitreous specimens were examined; 6 (23%) were positive.
To assess bcl-6 mRNA expression, PIOL and normal lymphocytes from ocular specimens of uveitic eyes were also microdissected. Only four patients had sufficient material for bcl-6 gene analysis. In all four patients with PIOL, higher expression of Bcl-6 mRNA was observed compared with mRNA samples isolated from the infiltrating lymphocytes of the four uveitic eyes or from mRNA isolated from the white blood cells of a healthy subject (Fig. 4). Three of these four patients also had the bcl-2 t(14;18) translocation at the Mbr site.
FIGURE 4.
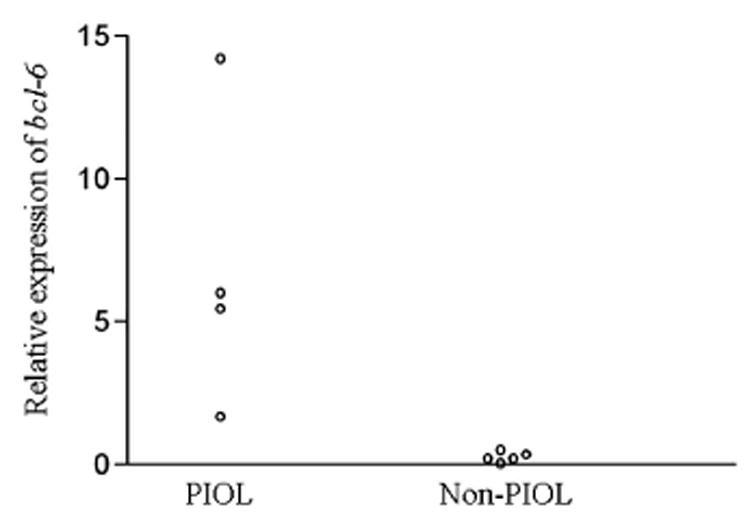
Analysis of expression of bcl-6 mRNA in PIOL cells compared with non-PIOL cells. Expression of bcl-6 was examined by PCR amplification of the cDNA complement of mRNA from four PIOL samples, four uveitis samples, and one healthy control sample. Autoradiography was used to compare relative amounts of bcl-6 and 18S mRNA. All four PIOL patients had higher expression of bcl-6, but none of the non-PIOL patients had high bcl-6 expression.
The detailed clinical course was available for 23 immunocompetent patients; mean follow-up was 29 months (Table 1). The countries of origin of the patients included the United States, France, Puerto Rico, Brazil, Japan, and Canada. Sixty-one percent expressed the bcl-2 t(14;18) translocation. Forty-eight percent of patients were older than 65. Sixty-one percent of patients had CNS involvement. Of the 14 patients who had CNS involvement, 12 had PCNSL at the time of diagnosis of PIOL, whereas in two patients CNS lesions developed during the course of the illness. The timing of the development of CNS disease was unclear from the final patient’s record. Sixty-three percent of patients received radiation therapy (10–60 Gy), and 48% received methotrexate-based therapy (including systemic high-dose, intravitreal, and intrathecal therapy). Other systemic chemotherapies included vincristine, thiotepa, procarbazine, dexamethasone, acepromazine, and cyclophosphamide, hydroxydaunomycin, Oncovin, prednisone (CHOP). Relapse occurred in 50% of patients. Therapeutic regimens after relapse included systemic bischloroethylnitrosourea (BCNU), temozolomide, cisplatin, thiotepa, cytarabine (Ara-C), methotrexate, and stem cell transplantation; intrathecal methotrexate, BCNU, Ara-C; intravitreal methotrexate; and radiation (Table 1). Too few patients received each therapy for adequate statistical analyses and conclusions about the specific therapeutic regimens. Survival ranged from 1 month to more than 84 months at the time of follow-up.
TABLE 1.
Clinical Outcomes of PIOL Patients
| Initial Therapy
|
||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Patient | Age (y) | Country | CNS Involvement | Radiation | MTX | Other Chemotherapy |
Relapse | Subsequent Treatment |
Survival (mo) | bcl-2 t(14; 18) Translocation |
| 1 | 76 | France | + | − | + (systemic) | − | − | N/A | 1 | + |
| 2 | 63 | United States | − | − | + (intravitreal) | − | + | Intrathecal: MTX | 56+ | + |
| 3 | 60 | Puerto Rico | + | + | − | − | − | Intravitreal: MTX N/A | 6 | + |
| 4 | 69 | Japan | + | + (30 Gy) | − | + Systemic: CHOP | + | Radiation: 40 Gy | 19 | + |
| 5 | 46 | Brazil | + | + (10 Gy) | − | − | − | N/A | 64+ | + |
| 6 | 51 | United States | + | − | + (intrathecal) | + Systemic: dexamethasone; Intrathecal: Ara-C | + | Systemic: BCNU, cisplatin, temozolomide, Ara-C Intrathecal: MTX, BCNU Intravitreal: MTX | 67+ | + |
| 7 | 77 | Japan | − | + (30 Gy) | − | − | − | N/A | 11+ | − |
| 8 | 63 | Japan | − | + (26 Gy) | − | − | − | N/A | 19+ | − |
| 9 | 80 | Japan | − | + (35 Gy) | − | − | − | N/A | 23+ | + |
| 10 | 48 | United States | + | + (54 Gy) | + (intrathecal) | + Systemic: Promace/ Cytabom Intrathecal: Ara-C | + | None | 9 | + |
| 11 | 73 | Japan | − | + (30 Gy) | − | + Systemic: CHOP | − | N/A | 34+ | − |
| 12 | 80 | Japan | − | + (39 Gy) | − | − | − | N/A | 48+ | + |
| 13 | 40 | Israel | + | U | U | U | U | U | 20+ | + |
| 14 | 38 | United States | + | + (40 Gy) | + (systemic high dose; intravitreal) | + | + | Systemic: MTX, stem cell transplantation; Radiation: dose unknown; Intravitreal: MTX | 29+ | + |
| 15 | 67 | United States | − | − | + (systemic high dose) | − | − | N/A | 12+ | + |
| 16 | 57 | United States | − | − | + (systemic high dose; intrathecal) | + Systemic: vincristine, procarbazine | + | Radiation: dose unknown Intravitreal: MTX | 33+ | + |
| 17 | 78 | United States | + | + (45 Gy) | U | U | U | U | 5+ | − |
| 18 | 58 | United States | + | − | + (systemic high dose) | + Systemic: thiotepa, vincristine Intrathecal: Ara-C) | + | Systemic: MTX Intrathecal: MTX, Ara-C Radiation × 2: 30 and 49 Gy | 84+ | + |
| 19 | 79 | United States | + | + (60 Gy) | − | − | + | None | 33+ | − |
| 20 | 47 | India | + | + (45 Gy) | + (systemic high dose) | + Systemic vincristine, thiotepa, dexamethasone, Intrathecal: Ara-C | + | Systemic: thiotepa, vincristine, MTX, dexamethasone, bone marrow transplantation Intrathecal: MTX and Ara-C | 67+ | + |
| 21 | 74 | United States | + | + (unknown dose) | − | − | + | none | 12+ | − |
| 22 | 73 | United States | − | − | − | − | − | N/A | 8 | − |
| 23 | 57 | Canada | + | − | + (systemic high dose) | − | − | N/A | 6+ | + |
U, information unavailable; MTX, methotrexate; N/A, not applicable.
Patients who were positive for the bcl-2 t(14;18) translocation were significantly younger (mean age, 58.9 years) than those who lacked the translocation (mean age, 73.9 years) (P = 0.001). After adjusting for age, no statistically significant difference was found in survival (hazard ratio, 2.33; P = 0.478) or relapse (odds ratio, 1.28; P = 0.840) between patients who did or did not have the bcl-2 t(14;18) translocation.
DISCUSSION
This study used microdissection and PCR techniques to examine the expression of bcl-2 t(14;18) translocation and the bcl-10 and bcl-6 genes. The bcl-2 t(14;18) translocation occurs in 57% to 90% of patients with follicular lymphoma (FL) and in 9% to 30% of patients with DLBCL; 55% to 60% of translocations occur at the Mbr, whereas 10% to 20% occur at the mcr.16,28–35 There is no known correlation between the bcl-2 t(14;18) translocation and bcl-2 expression.28,29 We found that 55% of samples expressed the translocation at the Mbr and that 22% of samples expressed the translocation at the mcr. Fourteen of 15 (93%) of the samples that were positive for the mcr translocation were also positive for the Mbr translocation. This finding is expected given the proximity of these two regions, which leads to overlap among the primer pairs.
Studies have reported conflicting roles for the bcl-2 t(14;18) translocation in patients with FL.33,36–40 However, a recent report of 131I-tositumomab therapy (an anti-CD20 antibody) for advanced stages of FL found that though there was no difference in outcome between patients with or without the translocation at baseline, this therapy resulted in the conversion of translocation status from positive to negative in 34 of 36 patients. Furthermore, negative translocation status correlated with clinical remission and predicted a durable complete remission.41 The only study involving PCNSL examined bcl-2 expression as opposed to the translocation and found no effect on prognosis.42
Conflicting reports have also been published on the role of the bcl-2 t(14;18) translocation in DLBCL prognosis. The recent development of DNA microarray technology has led to a genomewide approach to the study of DLBCL and has resulted in three distinct molecular subtypes of DLBCL indicative of different functional stages of B cell differentiation.43–46 The first type expresses genes characteristic of germinal center B cells (GCB-DLBCLs), whereas the second type expresses genes normally seen during in vitro activation of peripheral blood B cells (ABC-DLBCLs). The third type, primary mediastinal B cell lymphoma (PMBL), is more heterogeneous and not well defined. The GCB group has a significantly better survival than the ABC and PMBL groups. In two recent articles, expression of bcl-2 translocation and bcl-2 protein was reported to be associated with a significantly worse outcome in the non-GCB groups but not in the GCB group.47,48 However, another report demonstrated overall survival was significantly worse for bcl-2–positive patients in the GCB group but not in the non-GCB groups.49 Our study did not distinguish the genotypic classification or expression of the bcl-2 protein of the PIOL samples.
Although there are known prognostic factors in PCNSL, such as age, immune status, initial performance status, and CSF protein levels, there are no known prognostic factors for PIOL. Our study did not find a role for the bcl-2 t(14;18) translocation in determining length of survival or likelihood of disease relapse, though it is interesting to note that patients with the bcl-2 t(14;18) translocation were significantly younger, a finding similar to that observed by Gascoyne et al28 in patients with DLBCL. This may suggest a role for the translocation in accelerating disease presentation. In addition, this may suggest a need for aggressive therapy for younger patients with the translocation.
It is not surprising that there was no significant effect of the translocation on survival or occurrence of relapse. Because of the small number of patients affected by this disease, the numbers available for analysis are also small and may be inadequate. In addition, some of these patients received diagnoses in the early 1990s, when radiotherapy was considered the treatment of choice for PIOL and PCNSL.7,50 However, since that time, the benefits of systemic, intrathecal, and intravitreal chemotherapy and high-dose methotrexate have become more evident. These treatments have led to improved prognosis and survival of patients with PIOL. Furthermore, it is likely that the length of time to diagnosis and the extent of CNS involvement may play a more significant role in determining prognosis for patients with PIOL. Early systemic treatment of PIOL, before the onset of CNS involvement, results in better disease control and longer survival (39 months for isolated PIOL versus 24 months for PCNSL with ocular involvement).11
Bcl-10 is a molecule that regulates apoptosis.21 Mutations resulting in truncated proteins (that have subsequently lost their apoptosis-inducting function) have been detected at low frequencies in patients with DLBCL.51,52 With the use of immunohistochemistry studies, Ohshima et al.22 detected bcl-10 in 24% to 50% of patients with DLBCL. They did not detect any significant effect of bcl-10 expression on DLBCL prognosis. No reports have been published of bcl-10 expression in patients with FL or PCNSL. Our study detected the bcl-10 gene in 23% of PIOL samples. The relatively low expression could be related to the observation that bcl-10 is most closely related to mucosa-associated lymphoid tissue (MALT) lymphoma, a low-growth fraction lymphoma usually related to chronic inflammation.53 On the other hand, PCNSL and DLBCL each follow a more aggressive clinical course.23 Thus, it is not surprising that bcl-10 was detected at a low frequency in PIOL, a subset of PCNSL.
Although the International Prognostic Index is usually used to stratify DLBCL patients by level of risk, a number of cellular factors have been found to have prognostic significance in DLBCL. A phenotype similar to that seen in germinal center cells has been linked to a more favorable outcome. Lymphomas that are thought to have a germinal center origin express bcl-6 along with CD10.43,54
Bcl-6 is required for the formation of normal germinal center B cells and T cell–dependent antigen responses.23 It is also considered a proto-oncogene because of its involvement in translocations repeatedly found in DLBCL. Bcl-6 rearrangements are found in 23% to 37% of patients with DLBCL.29,55–57 Lossos et al.58 examined bcl-6 expression and found that over-expression was linked to better overall survival in patients with DLBCL. In DNA microarray analysis, the overexpression of bcl-6 correlates with GCB-DLBCL, which is associated with better prognosis.43–45 Similar findings were also found in PC-NSL.59 However, Chang et al.42 found that bcl-6–positive patients had poorer overall survival. In one PIOL study,60 immunohistochemistry found that PIOL cells were positive for Bcl-6. Our analysis looked at mRNA and found higher expression of bcl-6 mRNA in the PIOL cells of four selected patients who had sufficient samples for analysis compared with control and uveitis patients. This may support that PIOL cells have a germinal center origin, as also suggested by other studies.61
The current study provides important information about the expression pattern of several different apoptotic and cell differentiation genes in PIOL. In addition, it lays the foundation for the examination of p53, c-Myc, and other oncogenes in PIOL. However, it is important to recognize one important barrier that impeded this study. Working with vitreous specimens from PIOL patients provided a limited sample size (as few as 15 lymphoma cells per sample), which made microarray analysis and other techniques such as quantitative PCR extremely difficult. Indeed, as evidenced by the few samples analyzed for bcl-6 expression, mRNA from these lymphoma cells was extremely difficult to isolate. On the other hand, in studies of systemic and CNS lymphomas, larger amounts of tissue from biopsy specimens had been used. Thus, while great advances have been made in gene expression profiling for DLBCL, it is less likely that such a technique will be readily available for PIOL in the near future.
In summary, PIOL has unique molecular patterns of bcl-2, bcl-6, and bcl-10 compared with other types of lymphomas, such as follicular lymphoma, DLBCL, or PCNSL. Gene expression seems more closely related to GCB-DLBCL. The bcl-2 t(14;18) translocation is found significantly more often in younger patients with PIOL.
Acknowledgments
Supported by the Intramural Program of the National Eye Institute, National Institutes of Health, and by the National Institutes of Health Clinical Research Training Program.
Footnotes
Disclosure: D.J. Wallace, None; D.F. Shen, None; G.F. Reed, None; M. Miyanaga, None; M. Mochizuki, None; H.N. Sen, None; S.S. Dahr, None; R.R. Buggage, None; R.B. Nussenblatt, None; C.-C. Chan, None
References
- 1.Chan CC, Buggage RR, Nussenblatt RB. Intraocular lymphoma. Curr Opin Ophthalmol. 2002;13:411–418. doi: 10.1097/00055735-200212000-00012. [DOI] [PubMed] [Google Scholar]
- 2.Hormigo A, DeAngelis LM. Primary ocular lymphoma: clinical features, diagnosis, and treatment. Clin Lymphoma. 2003;4:22–29. doi: 10.3816/clm.2003.n.010. [DOI] [PubMed] [Google Scholar]
- 3.Paulus W. Classification, pathogenesis, and molecular pathology of primary CNS lymphomas. J Neurooncol. 1999;43:203–208. doi: 10.1023/a:1006242116122. [DOI] [PubMed] [Google Scholar]
- 4.Hoffman PM, McKelvie P, Hall AJ, Stawell RJ, Santamaria JD. Intraocular lymphoma: a series of 14 patients with clinicopathological features and treatment outcomes. Eye. 2003;17:513–521. doi: 10.1038/sj.eye.6700378. [DOI] [PubMed] [Google Scholar]
- 5.Hochberg FH, Miller DC. Primary central nervous system lymphoma. J Neurosurg. 1988;68:835–853. doi: 10.3171/jns.1988.68.6.0835. [DOI] [PubMed] [Google Scholar]
- 6.DeAngelis LM. Brain tumors. N Engl J Med. 2001;344:114–123. doi: 10.1056/NEJM200101113440207. [DOI] [PubMed] [Google Scholar]
- 7.Freeman LN, Schachat AP, Knox DL, Michels RG, Green WR. Clinical features, laboratory investigations, and survival in ocular reticulum cell sarcoma. Ophthalmology. 1987;94:1631–1639. doi: 10.1016/s0161-6420(87)33256-7. [DOI] [PubMed] [Google Scholar]
- 8.Whitcup SM, de Smet MD, Rubin BI, et al. Intraocular lymphoma: clinical and histopathologic diagnosis. Ophthalmology. 1993;100:1399–1406. doi: 10.1016/s0161-6420(93)31469-7. [DOI] [PubMed] [Google Scholar]
- 9.Akpek EK, Ahmed I, Hochberg FH, et al. Intraocular-central nervous system lymphoma: clinical features, diagnosis, and outcomes. Ophthalmology. 1999;106:1805–1810. doi: 10.1016/S0161-6420(99)90341-X. [DOI] [PubMed] [Google Scholar]
- 10.Rothova A, Ooijman F, Kerkhoff F, Van Der Lelij A, Lokhorst HM. Uveitis masquerade syndromes. Ophthalmology. 2001;108:386–399. doi: 10.1016/s0161-6420(00)00499-1. [DOI] [PubMed] [Google Scholar]
- 11.Hormigo A, Abrey LE, Heinemann MH, DeAngelis LM. Ocular presentation of primary central nervous system lymphoma: diagnosis and treatment. Br J Haematol. 2004;126:202–208. doi: 10.1111/j.1365-2141.2004.05028.x. [DOI] [PubMed] [Google Scholar]
- 12.Peterson K, Gordon KB, Heinemann MH, DeAngelis LM. The clinical spectrum of ocular lymphoma. Cancer. 1993;72:843–849. doi: 10.1002/1097-0142(19930801)72:3<843::aid-cncr2820720333>3.0.co;2-#. [DOI] [PubMed] [Google Scholar]
- 13.Levy-Clarke GA, Chan CC, Nussenblatt RB. Diagnosis and management of primary intraocular lymphoma. Hematol Oncol Clin North Am. 2005;19:739–749. doi: 10.1016/j.hoc.2005.05.011. [DOI] [PubMed] [Google Scholar]
- 14.Hockenbery D, Nunez G, Milliman C, Schreiber RD, Korsmeyer SJ. Bcl-2 is an inner mitochondrial membrane protein that blocks programmed cell death. Nature. 1990;348:334–336. doi: 10.1038/348334a0. [DOI] [PubMed] [Google Scholar]
- 15.Ngan BY, Chen-Levy Z, Weiss LM, Warnke RA, Cleary ML. Expression in non-Hodgkin’s lymphoma of the bcl-2 protein associated with the t(14;18) chromosomal translocation. N Engl J Med. 1988;318:1638–1644. doi: 10.1056/NEJM198806233182502. [DOI] [PubMed] [Google Scholar]
- 16.Cleary ML, Galili N, Sklar J. Detection of a second t(14;18) breakpoint cluster region in human follicular lymphomas. J Exp Med. 1986;164:315–320. doi: 10.1084/jem.164.1.315. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Cotter F, Price C, Zucca E, Young BD. Direct sequence analysis of the 14q+ and 18q- chromosome junctions in follicular lymphoma. Blood. 1990;76:131–135. [PubMed] [Google Scholar]
- 18.Weiss LM, Warnke RA, Sklar J, Cleary ML. Molecular analysis of the t(14;18) chromosomal translocation in malignant lymphomas. N Engl J Med. 1987;317:1185–1189. doi: 10.1056/NEJM198711053171904. [DOI] [PubMed] [Google Scholar]
- 19.Bakhshi A, Jensen JP, Goldman P, et al. Cloning the chromosome breakpoint of t(14;18) human lymphomas: clustering around Jh on chromosome 14 and near a transcriptional unit on 18. Cell. 1985;41:899–906. doi: 10.1016/s0092-8674(85)80070-2. [DOI] [PubMed] [Google Scholar]
- 20.Tsujimoto Y, Cossman J, Jaffe E, et al. Involvement of the Bcl-2 gene in human follicular lymphomas. Science. 1985;228:1440–1443. doi: 10.1126/science.3874430. [DOI] [PubMed] [Google Scholar]
- 21.Zhang Q, Siebert R, Yan M, et al. Inactivating mutations and overexpression of Bcl10, a caspase recruitment domain-containing gene in MALT lymphoma with t(1;14)(P22;Q32) Nat Genet. 1999;22:63–68. doi: 10.1038/8767. [DOI] [PubMed] [Google Scholar]
- 22.Ohshima K, Kawaskaki C, Muta H. CD10 and Bcl10 expression in diffuse large B-cell lymphoma: CD10 is a marker of improved prognosis. Histopathology. 2001;39:156–162. doi: 10.1046/j.1365-2559.2001.01196.x. [DOI] [PubMed] [Google Scholar]
- 23.Sanchez-Beato M, Sanchez-Aguilera A, Piris MA. Cell cycle deregulation in B-cell lymphomas. Blood. 2003;101:1220–1235. doi: 10.1182/blood-2002-07-2009. [DOI] [PubMed] [Google Scholar]
- 24.Levy-Clarke GA, Byrnes GA, Buggage RR, et al. Primary intraocular lymphoma diagnosed by fine needle aspiration biopsy of a subretinal lesion. Retina. 2001;21:281–284. doi: 10.1097/00006982-200106000-00023. [DOI] [PubMed] [Google Scholar]
- 25.Shen DF, Zhuang Z, LeHoang P, et al. Utility of microdissection and polymerase chain reaction for the detection of immunoglobulin gene rearrangement and translocation in primary intraocular lymphoma. Ophthalmology. 1998;105:1664–1669. doi: 10.1016/S0161-6420(98)99036-4. [DOI] [PubMed] [Google Scholar]
- 26.Chan CC. Molecular pathology of primary intraocular lymphomas. Trans Am Ophthalmol Soc. 2003;101:43–60. [PMC free article] [PubMed] [Google Scholar]
- 27.Segal GH, Jorgensen T, Scott M, Braylan RC. Optimal primer selection for clonality assessment by polymerase chain reaction analysis, II: follicular lymphomas. Hum Pathol. 1994;25:1276–1282. doi: 10.1016/0046-8177(94)90085-x. [DOI] [PubMed] [Google Scholar]
- 28.Gascoyne RD, Adomat SA, Krajewski S. Prognostic significance of bcl-2 protein expression and bcl-2 gene rearrangement in diffuse aggressive non-Hodgkin’s lymphoma. Blood. 1997;90:244–251. [PubMed] [Google Scholar]
- 29.Kramer MH, Hermans J, Wijburg E, et al. Clinical relevance of BCL2, BCL6, and MYC rearrangements in diffuse large B-cell lymphoma. Blood. 1998;92:3152–3162. [PubMed] [Google Scholar]
- 30.Corbally N, Grogan L, Dervan PA, Carney DN. The detection of specific gene rearrangements in non-Hodgkin’s lymphoma using the polymerase chain reaction. Br J Cancer. 1992;66:805–809. doi: 10.1038/bjc.1992.364. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Tang SC, Visser L, Hepperle B, Hanson J, Poppema S. Clinical significance of Bcl-2-MBR gene rearrangement and protein expression in diffuse large-cell non-Hodgkin’s lymphoma: an analysis of 83 cases. J Clin Oncol. 1994;12:149–154. doi: 10.1200/JCO.1994.12.1.149. [DOI] [PubMed] [Google Scholar]
- 32.Jacobson JO, Wilkes BM, Kwaiatkowski DJ, Medeiros LJ, Aisenberg AC, Harris NL. Bcl-2 rearrangements in de novo diffuse large cell lymphoma: association with distinctive clinical features. Cancer. 1993;72:231–236. doi: 10.1002/1097-0142(19930701)72:1<231::aid-cncr2820720141>3.0.co;2-5. [DOI] [PubMed] [Google Scholar]
- 33.Yunis JJ, Mayer MG, Arnesen MA, Aeppli DP, Oken MM, Frizzera G. Bcl-2 and other genomic alterations in the prognosis of large-cell lymphoma. N Engl J Med. 1989;320:1047–1054. doi: 10.1056/NEJM198904203201605. [DOI] [PubMed] [Google Scholar]
- 34.Hill ME, MacLennan KA, Cunningham DC, et al. Prognostic significance of BCL-2 expression and bcl-2 major breakpoint region rearrangement in diffuse large cell non-Hodgkin’s lymphoma: a British national lymphoma investigation study. Blood. 1996;88:1046–1051. [PubMed] [Google Scholar]
- 35.Offit K, Koduru PR, Hollis R, et al. 18q21 rearrangement in diffuse large cell lymphoma: incidence and clinical significance. Br J Haematol. 1989;72:178–183. doi: 10.1111/j.1365-2141.1989.tb07680.x. [DOI] [PubMed] [Google Scholar]
- 36.Johnson A, Brun A, Dictor M, Rambech E, Akerman M, Anderson H. Incidence and prognostic significance of t(14;18) translocation in follicle center cell lymphoma of low and high grade: a report from southern Sweden. Ann Oncol. 1995;6:789–794. doi: 10.1093/oxfordjournals.annonc.a059317. [DOI] [PubMed] [Google Scholar]
- 37.Levine EG, Arthur DC, Frizzera G, Peterson BA, Hurd DD, Bloomfield CD. Cytogenetic abnormalities predict clinical outcome in non-Hodgkin lymphoma. Ann Intern Med. 1988;108:14–20. doi: 10.7326/0003-4819-108-1-14. [DOI] [PubMed] [Google Scholar]
- 38.Pezzella F, Jones M, Ralfkiaer E, Ersboll J, Gatter KC, Mason DY. Evaluation of Bcl-2 protein expression and 14;18 translocation as prognostic markers in follicular lymphoma. Br J Cancer. 1992;65:87–89. doi: 10.1038/bjc.1992.16. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Tilly H, Rossi A, Stamatoullas A, et al. Prognostic value of chromosomal abnormalities in follicular lymphoma. Blood. 1994;84:1043–1049. [PubMed] [Google Scholar]
- 40.Lopez-Guillermo A, Cabanillas F, McDonnell TI, et al. Correlation of Bcl-2 rearrangement with clinical characteristics and outcome in indolent follicular lymphoma. Blood. 1999;93:3081–3087. [PubMed] [Google Scholar]
- 41.Kaminski MS, Tuck M, Estes J, et al. 131I-tositumomab therapy as initial treatment for follicular lymphoma. N Engl J Med. 2005;352:441–449. doi: 10.1056/NEJMoa041511. [DOI] [PubMed] [Google Scholar]
- 42.Chang CC, Kampalath B, Schultz C, et al. Expression of P53, c-Myc, or Bcl-6 suggests a poor prognosis in primary central nervous system diffuse large B-cell lymphoma among immunocompetent individuals. Arch Pathol Lab Med. 2003;127:208–212. doi: 10.5858/2003-127-208-EOPMOB. [DOI] [PubMed] [Google Scholar]
- 43.Alizadeh AA, Eisen MB, Davis RE, et al. Distinct types of diffuse large B-cell lymphoma identified by gene expression profiling. Nature. 2000;403:503–511. doi: 10.1038/35000501. [DOI] [PubMed] [Google Scholar]
- 44.Rosenwald A, Wright G, Chan WC, et al. The use of molecular profiling to predict survival after chemotherapy for diffuse large-B-cell lymphoma. N Engl J Med. 2002;346:1937–1947. doi: 10.1056/NEJMoa012914. [DOI] [PubMed] [Google Scholar]
- 45.Wright G, Tan B, Rosenwald A, Hurt EH, Wiestner A, Staudt LM. A gene expression-based method to diagnose clinically distinct subgroups of diffuse large B cell lymphoma. Proc Natl Acad Sci USA. 2003;100:9991–9996. doi: 10.1073/pnas.1732008100. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Staudt LM, Dave S. The biology of human lymphoid malignancies revealed by gene expression profiling. Adv Immunol. 2005;87:163–208. doi: 10.1016/S0065-2776(05)87005-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Hans CP, Weisenburger DD, Greiner TC, et al. Confirmation of the molecular classification of diffuse large B-cell lymphoma by immunohistochemistry using a tissue microarray. Blood. 2004;103:275–282. doi: 10.1182/blood-2003-05-1545. [DOI] [PubMed] [Google Scholar]
- 48.Iqbal J, Sanger WG, Horsman DE, et al. BCL2 translocation defines a unique tumor subset within the germinal center B-cell-like diffuse large B-cell lymphoma. Am J Pathol. 2004;165:159–166. doi: 10.1016/s0002-9440(10)63284-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Berglund M, Thunberg U, Amini RM, et al. Evaluation of immunophenotype in diffuse large B-cell lymphoma and its impact on prognosis. Mod Pathol. 2005;18:1113–1120. doi: 10.1038/modpathol.3800396. [DOI] [PubMed] [Google Scholar]
- 50.Khan RB, Shi W, Thaler HT, DeAngelis LM, Abrey LE. Is intrathecal methotrexate necessary in the treatment of primary CNS lymphoma? J Neurooncol. 2002;58:175–178. doi: 10.1023/a:1016077907952. [DOI] [PubMed] [Google Scholar]
- 51.Tadokoro J, Nakamura Y, Furusawa S, et al. Low frequency of Bcl10 gene mutations in B-cell non-Hodgkin’s lymphoma. Int J Hematol. 2001;73:222–225. doi: 10.1007/BF02981941. [DOI] [PubMed] [Google Scholar]
- 52.Takahashi H, Hosokawa Y, Suzuki R. Infrequent bcl10 mutations in B-cell non-Hodgkin’s lymphomas. Jpn J Cancer Res. 1999;90:1316–1320. doi: 10.1111/j.1349-7006.1999.tb00714.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Capello D, Gaidano G. Molecular pathophysiology of indolent lymphoma. Haematologica. 2000;85:195–201. [PubMed] [Google Scholar]
- 54.Barrans SL, Carter I, Owen RG, et al. Germinal center phenotype and bcl-2 expression combined with the International Prognostic Index improves patient risk stratification in diffuse large B-cell lymphoma. Blood. 2002;99:1136–1143. doi: 10.1182/blood.v99.4.1136. [DOI] [PubMed] [Google Scholar]
- 55.Lo Coco F, Ye BH, Lista F, et al. Rearrangements of the BCL6 gene in diffuse large cell non-Hodgkin’s lymphoma. Blood. 1994;83:1757–1759. [PubMed] [Google Scholar]
- 56.Bastard C, Deweindt C, Kerckaert JP, et al. LAZ3 rearrangements in non-Hodgkin’s lymphoma: correlation with histology, immunophenotype, karyotype, and clinical outcome in 217 Patients. Blood. 1994;83:2423–2427. [PubMed] [Google Scholar]
- 57.Offit K, Lo Coco F, Louie DC, et al. Rearrangement of the bcl-6 gene as a prognostic marker in diffuse large-cell lymphoma. N Engl J Med. 1994;331:74–80. doi: 10.1056/NEJM199407143310202. [DOI] [PubMed] [Google Scholar]
- 58.Lossos IS, Jones CD, Warnke R, et al. Expression of a single gene, Bcl-6, strongly predicts survival in patients with diffuse large B cell lymphoma. Blood. 2001;98:945–951. doi: 10.1182/blood.v98.4.945. [DOI] [PubMed] [Google Scholar]
- 59.Braaten KM, Ketensky RA, de Leval L, et al. Bcl-6 expression predicts improved survival in patients with primary central nervous system lymphoma. Clin Cancer Res. 2003;9:1063–1069. [PubMed] [Google Scholar]
- 60.Coupland SE, Bechrakis NE, Anastassiou G, et al. Evaluation of vitrectomy specimens and chorioretinal biopsies in the diagnosis of primary intraocular lymphoma in patients with masquerade syndrome. Graefes Arch Clin Exp Ophthalmol. 2003:860 –870. doi: 10.1007/s00417-003-0749-y. [DOI] [PubMed] [Google Scholar]
- 61.Coupland SE, Loddenkemper C, Smith JR, et al. Expression of immunoglobulin transcription factors in primary intraocular lymphoma and primary central nervous system lymphoma. Invest Ophthalmol Vis Sci. 2004:3957–3964. doi: 10.1167/iovs.05-0318. [DOI] [PubMed] [Google Scholar]