

Abstract
Objective
Early detection of hearing loss in infants and toddlers has created a need for age-appropriate tests of auditory perceptual capabilities. This article describes a progressive test battery we have developed to evaluate phonetic contrast perception, phoneme recognition, and word recognition in children 6 months to 5 years. This battery is part of a clinical research protocol designed to track auditory development in this population.
Methods
The progressive test battery originated from a model of auditory perceptual development to assess phonetic discrimination and word recognition. Phonetic discrimination is evaluated using the Battery of Auditory Speech Perception Tests for Infants and Toddlers (BATIT). The BATIT is composed of four measures (VRASPAC, PLAYSPAC, OLIMSPAC, and VIDSPAC) intended to assess the child’s ability to distinguish between phonologically significant contrasts using developmentally appropriate tasks. Designed for children aged 6 months and up, performance is represented either by percent correct or by the level of confidence that the child’s responses are not random. Phoneme and word recognition are assessed in children 4 years and older using lists of consonant-vowel-consonant (CVC) phonemes in words and lexically controlled words both in and out of sentence context (LEXSEN).
Results
Cross-sectional data show that children with normal hearing may be assessed by the age of 7 months on VRASPAC; by 3 years on PLAYSPAC and OLIMSPAC; and by 4 to 5 years on VIDSPAC, CVC phonemes in words, and LEXSEN words in isolation and in sentences. Data from infants with hearing loss showed that VRASPAC was sensitive to degree of hearing loss, but performance with normally hearing children on this test declined after 12 months of age.
Conclusion
Assessment of phonetic discrimination and word recognition is, for the most part, attainable in young children using a progressive test battery, but none of the tests used here was effective between 1 and 3 years of age. Continued development will be required to fill this gap and to separate auditory from non-auditory influences in performance.
1. Introduction
Successful implementation of Early Hearing Detection and Intervention programs in the United States has contributed to effective communication-skill development in young children identified with congenital hearing loss [1,2]. This breakthrough is possible because of innovative techniques in hearing assessment combined with advances in sensory device technology. Thus, it is possible to identify hearing loss at birth and fit state-of-the-art hearing aids and/or cochlear implants soon thereafter. After a child is identified with hearing loss, ear- and frequency-specific thresholds are obtained using physiological and behavioral audiological measures [3]. Prescriptions for fitting hearing aids take into account the unique amplification characteristics required for infants and toddlers [4]. Despite this progress, there remains a lack of age-appropriate assessment tools for which to substantiate auditory perceptual capabilities in children during the early stages of their intervention. This type of assessment is needed to help guide decisions about sensory device candidacy, track performance over a period of time, and establish individualized plans for habilitation. Thus, a major challenge confronting the field of pediatric audiology is to develop appropriate evaluation protocols that will ascertain auditory perceptual capability in the very young child with hearing loss.
From a theoretical standpoint, emergence of auditory perceptual milestones in young children would be expected to follow a trajectory of general perceptual development. One such model, proposed by Aslin and Smith [5], describes the following three stages of development: sensory primitives (Level I), which characterizes basic sensory perception; perceptual representations (Level II), which represents complex coding at higher neural levels; and higher order representations (Level III), which denotes cognitive/linguistic processing.
Carney [6] adopted the Aslin and Smith [5] model to describe three corresponding levels of auditory perceptual development in infants and toddlers. The three levels encompass sound awareness (Level I), phonetic discrimination (Level II), and word recognition (Level III). To elaborate, Level I represents awareness or attentiveness to sound, typically assessed through basic audiometric testing and parent report (e.g., Ling Developmental Schedules [7]; IT-MAIS [8]). Level II relates to complex encoding of stimuli at higher neural levels, which entails differentiation between speech sounds spanning broad phonetic categories. Level II activities have included visual reinforcement techniques for infants [9] and conditioned play activities for toddlers [10]. Both are well-established audiometric techniques for obtaining thresholds in this population, but have not been adopted clinically for measuring speech discrimination. These techniques, however, provide the foundation for two measures we will be describing as part of a progressive test battery.
Level III moves into the realm of word recognition. The ability to recognize words improves as the child matures. This improvement is mediated by a growing repertoire of phonemes, vocabulary, and motor speech skills, plus the ability to use contextual information (lexical, syntactic, semantic, social, and situational). Behavioral measures of word recognition are introduced when a child reaches 2 or 3 years of age. Tests for children of this age tend to rely on closed-set word- and sentence-identification tasks that require a forced choice—typically through a picture-pointing response. Clinical tests used in the United States include the Northwestern University-Children’s Perception of Speech (NU-CHIPS) [11], the Early Speech Perception (ESP) Test [12], and the Pediatric Speech Intelligibility (PSI) Test [13]. The Lexical Neighborhood Test (LNT) [14] is an open-set test of word recognition derived from the spoken vocabulary of young children between 3 and 5 years of age. Open-set tests, such as LNT, typically require the child to repeat the word. When children reach 5 or 6 years of age, more advanced word and sentence stimuli are introduced, such as the Phonetically Balanced-Kindergarten (PBK) Lists [15] and the Hearing In Noise Test-Children (HINT-C) [16].
As part of an ongoing clinical research protocol, we have devised a battery of software-driven tests to evaluate auditory perceptual development. The battery assesses phonetic discrimination, or what we are calling speech pattern contrast perception, (Level II) and word recognition (Level III). The target age range is 6 months to 5 years of age. A secondary aim is to provide software that is both user- and child-friendly in a clinical environment. Described below, the tests are divided into the broad categories of speech pattern contrast perception and phoneme/word recognition. This general description is followed by results obtained to date.
2. Methods
2.1. Tests of Speech Pattern Contrast Perception
The Battery of Auditory Speech Perception Tests for Infants and Toddlers (BATIT) consists of four computerized tests (VRASPAC, PLAYSPAC, OLIMSPAC, and VIDSPAC) that measure speech pattern contrast perception in children as they transition from infancy to preschool age. These tests evolved from the Speech Pattern Contrast Test (SPAC), originally developed by Boothroyd [17] for use with older children having reading skills. The tests comprising BATIT systematically lower the age limit to much younger children.
The stimulus set and perceptual task are held constant across the four tests of BATIT, but the response task changes according to the age, maturity and interest level of the child. The stimulus set consists of vowel-consonant-vowel (VCV) nonsense syllables recorded using a female talker. The perceptual task requires differentiation of vowel height, vowel place, consonant voicing, consonant manner, and consonant place in the bilabial-alveolar (front) and alveolar-palatal (rear) position. Examples of these contrasts are found in Table 1.
Table 1.
Examples of BATIT phonetic contrasts.
| Phonetic Contrasts | |
|---|---|
| Vowel Height | “oodoo” vs “aadaa” |
| Vowel Place | “oodoo” vs “eedee” |
| Consonant Voicing | “oodoo” vs “ootoo” |
| Consonant Manner | “oodoo” vs “oozoo” |
| Consonant Place (f)* | “oodoo” vs “ooboo” |
| Consonant Place (r)** | “oodoo” vs “oogoo” |
f = front (alveolar-bilabial)
r = rear (alveolar-palatal)
Performance on the individual tests of BATIT is determined not only by percent-correct scores but also by the level of confidence that the child’s responses are not random. The level of confidence is derived from probability theory, taking into account the number of deviant utterances, trials, responses occurring during the hypothetical response window, and false positives. Diagrams for each test are condensed into one graph for convenience (Figure 1), but all tests are carried out in one sound-attenuating booth.
Figure 1.
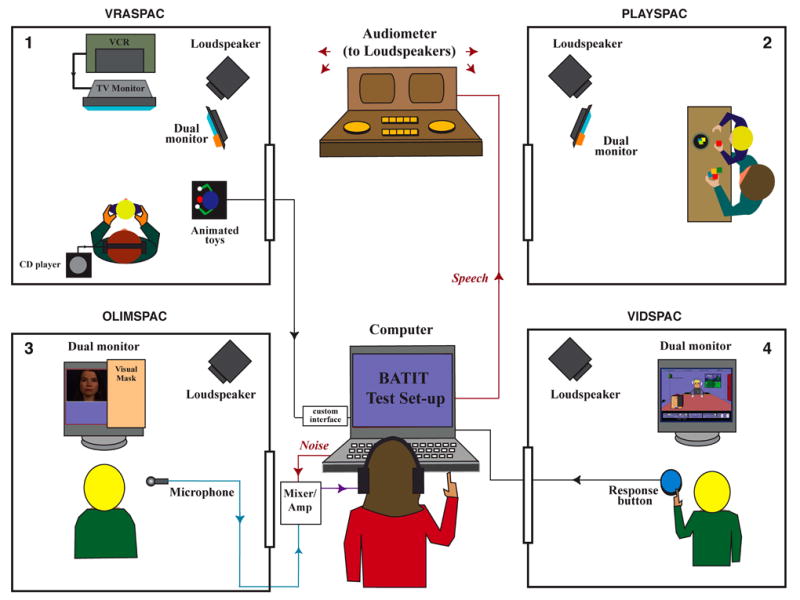
Diagrams of the four test set-ups for BATIT: (1) VRASPAC, (2) PLAYSPAC, (3) OLIMSPAC, and (4) VIDSPAC.
2.1.1. VRASPAC
VRASPAC, or Visual Reinforcement Assessment of the Perception of Speech Pattern Contrasts [18,19,20], is modeled after the Visual Reinforcement Infant Speech Discrimination (VRISD) Test [9]. VRASPAC has been designed for children as young as 6 months, the approximate age when infants are able to turn their head to look at a sound source. Displayed in the upper left hand corner in Figure 1 (1), the test set-up shows the child sitting in the lap of the caregiver, who listens to music during the test. The child either watches a video or attends to a test assistant. During test administration, a standard syllable is presented repeatedly in the sound field (e.g., “oodoo, oodoo, oodoo, oodoo, …”) until the child habituates to the standard. The contrast stimulus is then presented (e.g., vowel height, “aadaa, aadaa, aadaa”) and the child is conditioned (or trained) to turn toward the reinforcer (either an animated toy or a cartoon on a computer monitor). Test trials commence as soon as the child is conditioned. The test trial is terminated either by a preset stopping rule or manually by the tester, usually a result of the child losing interest in the task. The automatic stopping rule is determined by a confidence-level criterion, usually 90%. A stopping criterion increases efficiency, which is an important consideration when assessing infants.
2.1.2. PLAYSPAC
PLAYSPAC, or Play Assessment of Speech Pattern Contrasts [19], is displayed in the upper left hand corner of Figure 1 (2). Although we had hoped that PLAYSPAC would be appropriate for use with children at 24 to 30 months of age, our experiences to date suggest it is more applicable for children 36 months of age and older. Modeled after conditioned play audiometry and the Speech Feature Test [10], the child engages in a motor activity, such as putting a peg in a board or pushing a button, upon perceiving the phonetic change. The software is similar to that used for VRASPAC, including the use of an automatic stopping rule. In addition, there is an option to present a visual reward on the computer monitor for correct identification, such as a piece of a jigsaw puzzle that is revealed each time the child responds to the phonetic change. As with VRASPAC, conditioning trials precede testing.
2.1.3. OLIMSPAC
OLIMSPAC, or On-line Imitative Test of Speech Pattern Contrast Perception [18, 21,22,23,24], was developed for children 3 years of age and older, although the test has been administered to children as young as 2.5 years. Based on the notion that young children will naturally imitate speech, OLIMSPAC assesses perception of phonologically significant contrasts through repetition of each stimulus item. Thus, administration of the OLIMSPAC is incumbent upon the child having phonological knowledge and motor speech skills.
The original IMSPAC was developed for use as a research tool in which the child’s imitations were recorded and edited off line for a panel of judges to evaluate [25]. This new online version enables scoring as the test progresses. It is important to note that OLIMSPAC does not require an assessment of the quality or accuracy of the child’s imitation, but only its ability to provide the listener with phonemically contrastive information. OLIMSPAC differs from the other tests of BATIT in that it is multimodal; the test is administered first in the auditory-visual (AV) modality and then the auditory-only (AO) modality. AV scores are expected to be higher than AO scores, lending support to the assumption that speech production is not the limiting factor when testing in the AO modality.
A diagram of the OLIMSPAC set-up is shown in the lower left hand corner of Figure 1 (3), illustrating testing in the AV modality. The child is seated inside the test booth facing a secondary monitor. The target stimulus is presented in the sound field and the child repeats the stimulus into a microphone. The tester selects the stimulus that best approximates the child’s utterance from a choice of eight alternatives (three binary-choices). The tester is masked from hearing and seeing the target stimulus to ensure objectivity.
A complete run per modality (AV or AO) involves 16 trials. The first eight trials simultaneously assess vowel height, consonant voicing, and front consonant place. The second eight trials simultaneously assess vowel place, consonant manner, and rear consonant place. To explain, let’s say that the stimulus item presented is “oochoo” and the child repeats “oochoo”. In this case, the child receives credit for three contrasts—vowel height, consonant manner, and rear consonant place. However, should the child utter “ootoo” instead of “oochoo”, credit is given for vowel height and consonant manner, but not for rear consonant place.
2.1.4. VIDSPAC
VIDSPAC, or Video Speech Pattern Contrast Test [18, 26,27], assesses speech pattern contrast perception using a video-game format. VIDSPAC has been administered to children 5 years of age and older [28,29], although we have observed children as young as 4 years able to perform the task. VIDSPAC is similar to VRASPAC and PLAYSPAC in that the perceptual task requires the child to indicate when a phonetic change is detected during a series of repeated nonsense syllables. The child responds by pushing a button that interfaces with the computer, as shown in the lower right hand corner of Figure 1 (4). Alternate methods of response can be incorporated, such as hitting a key on the computer keyboard or use of the mouse. VIDSPAC is the only test of BATIT in which feedback is provided. To keep the child motivated throughout the test, a brief cartoon can be viewed following the completion of each contrast. Two auditory-visual practice conditions, contrasting vowel height and place, precede testing in the auditory-only modality. There are four trials per contrast.
2.1.5. Graphic analysis for BATIT
The four tests of BATIT are under computer control to facilitate standardization and automatic computation of performance and data-logging. Upon completion of a test, a summary of the data is retrieved in graphic format which may be printed and kept as a record in the child’s chart. Inasmuch as VRASPAC, PLAYSPAC, and VIDSPAC are similar in software and graphic output, an example of results is shown only for VRASPAC. Audiometric and VRASPAC results are displayed in Figure 2 for a 12-month-old boy wearing hearing aids. This child was identified with hearing loss at birth and fitted with hearing aids at 6 weeks. The top part of the figure shows his unaided audiogram, indicating a bilateral, moderately severe hearing loss. Below is the profile of performance scores for individuals contrasts, vowels combined, consonants combined, and the composite score averaged across all contrasts. Testing for this child was completed in three sessions. The results indicated above-chance performance for vowel height and consonant continuance (or manner). The composite score averaged across features was 65%. Below the graph is a numeric summary of the data, including confidence levels that the responses were not random. The confidence level was 92% both for vowel height and consonant continuance.
Figure 2.
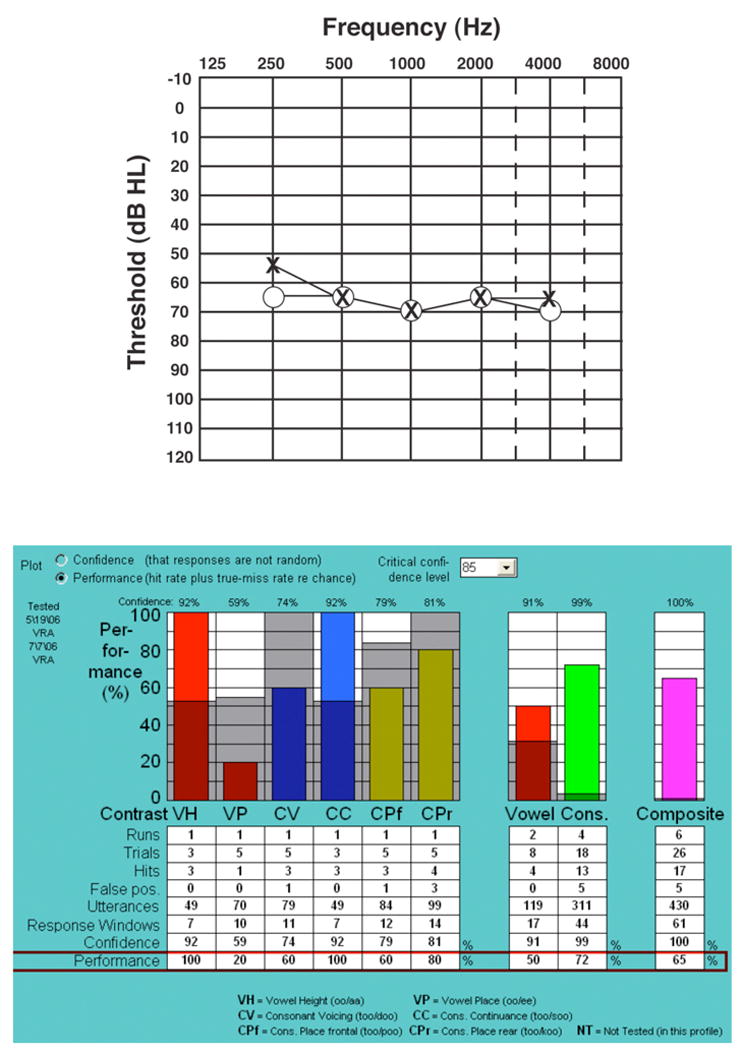
Audiogram and performance profile for a 12-month-old hearing aid user assessed on VRASPAC.
The graphic output of OLIMSPAC differs from the other three tests because it is the only test that is multimodal, i.e., administered in AV and AO modalities. A test profile for OLIMSPAC is shown in Figure 3 for a 4.5-year-old male child. The audiogram indicates a bilateral profound loss, which was identified when the child was 16 months. Following unsuccessful trials with hearing aids, the child received a cochlear implant at 25 months. With the implant activated, AV scores on OLIMSPAC were above-chance for all contrasts except rear consonant place. AO scores were above chance for all contrasts except consonant voicing and rear consonant place. The composite scores were 79% (AV) and 67% (AO).
Figure 3.
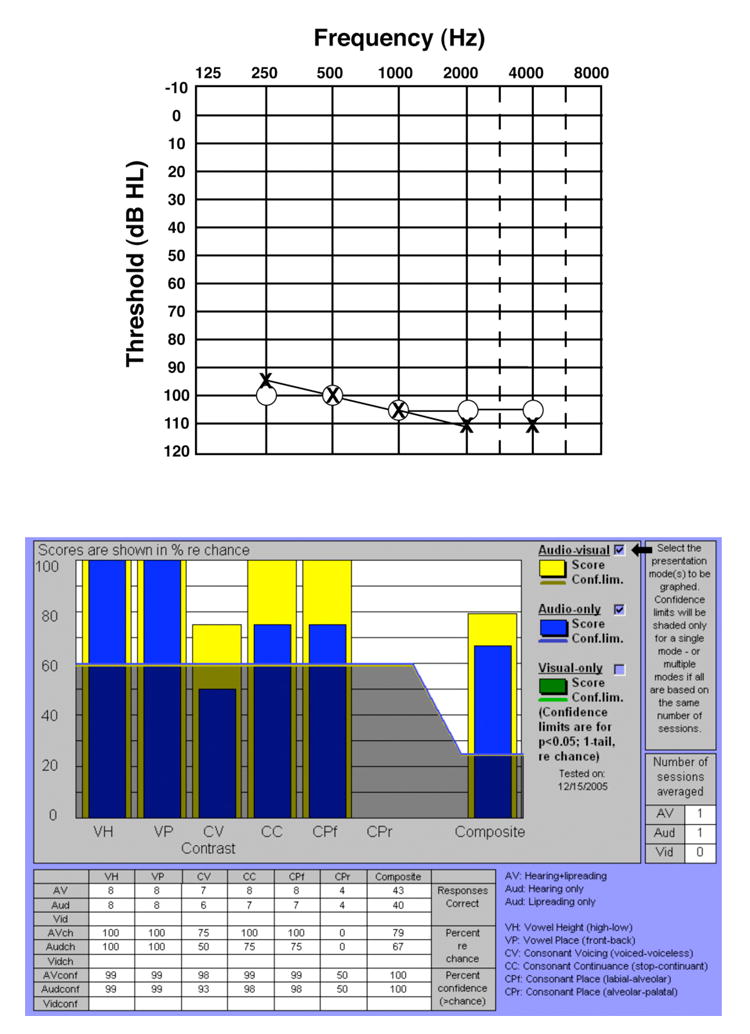
Audiogram and performance profile for a 4.5-year-old cochlear implant user assessed on OLIMSPAC.
2.2. Tests of Phoneme and Word Recognition
2.2.1. Phonemes in Words
In progressing from phonetic contrast perception (Level II) to word recognition (Level III), we transition via phoneme recognition of consonant-vowel-consonant (CVC) words using the AB Isophonemic Word Lists [30]. A software program called Computer-Assisted Speech Perception Assessment (CASPA) [32,33] has been produced for ease of delivery, scoring, and analysis.
CASPA delivers 20 sets of 10 CVC words. Within each set there is one instance each of 10 vowels and 20 consonants. The lists are constructed without reference to consonant position (pre- or post-vocalic), frequency of word occurrence, or lexical neighborhood size. They are, however, intended to be scored phonemically (i.e., one point for each phoneme correctly recognized). This approach to scoring minimizes the contributions of linguistic factors and reduces confidence limits relative to the more traditional whole-word scoring [30,31].
2.2.2. Words in Isolation and in Sentences
LEXSEN is a test composed of lexically controlled sentences [34] that evolved from the Lexical Neighborhood Test (LNT) [14]. The LNT is an open-set test of word recognition that classifies words according to frequency of occurrence and acoustic-phonetic similarity. LEXSEN extended this concept by presenting lexically controlled words in sentence context. The words selected for LEXSEN were generated from the spoken vocabulary of normal-hearing children between the ages of 3 and 5 years (CHILDES database) [35],
Two lists of 20 sentences were created, with each sentence containing 3 lexically controlled key words. One sentence list was composed of 60 lexically “easy” words high in frequency of occurrence with low neighborhood density (i.e., phonemically dissimilar to other words). The other sentence list was composed of 60 lexically “hard” words low in frequency of occurrence with high neighborhood density (i.e., phonemically confusable with other words). For ease of administration, a software program was produced for delivery of digitized stimulus files, scoring, and subsequent analysis [36].
3.0. Results
Results obtained to date are first presented for a sample of normally hearing children. Normally hearing children are assessed under the assumption that they have normal auditory capacity, and any deviation from perfect performance would be considered an index of non-auditory, developmental, or task-related factors. If, for example, a group of 3-year-old normally hearing children attains a mean score of 80% on a given test, we would not expect a child with hearing loss to do any better. Inasmuch as variability is expected even with normally hearing young children, estimates of performance will require testing on a much larger sample than we present here. The data on normally hearing children are then followed by VRASPAC data on infants and toddlers with hearing loss.
3.1. Children with normal hearing
Cross sectional data from a small sample of normally hearing children are displayed in Figure 4 as a function of age on the four tests of BATIT, CASPA phonemes in words, and LEXSEN words in isolation and in sentences (collapsed across easy and hard lists). Vowel scores only are shown for VRASPAC because these contrasts represent the most data collected at this time. OLIMSPAC scores represent testing in the auditory-only modality. The curves are least-squares fits of a cubed-exponential growth function to the data. The functions suggest the lowest age range for administering each test. Data for VRASPAC vowels showed the lowest age to be 7 months, although younger infants have not been tested to date. A dip in scores was seen at 18 months with recovery at 30 months. This dip suggests an age at which children may be too old for VRASPAC but too young for the other tests. Near ceiling scores were reached by 3 years on PLAYSPAC and OLIMSPAC, by 4 years on VIDSPAC, and by 4.5 to 5 years on CASPA and LEXSEN.
Figure 4.

Performance scores of children with normal hearing assessed on VRASPAC (vowels only), PLAYSPAC, OLIMSPAC (auditory only), VIDSPAC, CASPA CVC phonemes, and LEXSEN words in isolation and in sentences.
Whereas Figure 4 displays vowel data only for the VRASPAC, Figure 5 presents data on all contrasts as a function of age in months for infants with normal hearing. Variability is shown for individual subjects and the trend shows a decrease in performance as children mature beyond 12 months, particularly for consonants (as shown in the Figure 5 inset). Assuming that children with normal hearing have full auditory capacity, the observed decline in performance beyond 12 months of age points to a task-related factor. In other words, the visual-reinforcement paradigm is no longer compatible with the child’s developmental status, needs, or interests.
Figure 5.
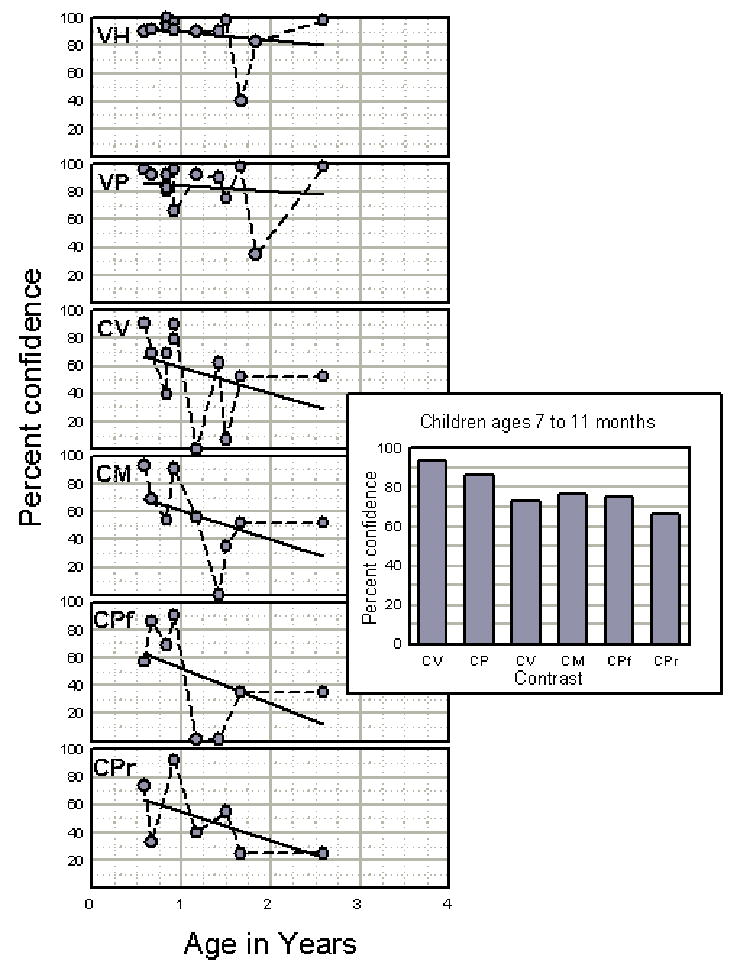
Confidence level scores of normally hearing children assessed on the six contrasts of VRASPAC as functions of age. VH= vowel height; VP=vowel place; CV=consonant voicing; CM=consonant manner; CPf=consonant place (front); CPr=consonant place (rear). The inset is a contrast profile showing the mean confidence scores of normally hearing children aged 7 through 11 months.
3.2. VRASPAC results on children with hearing loss
A small sample of infants and toddlers using hearing aids has been evaluated on VRASPAC. Degree of hearing loss ranges from mild to profound hearing loss, which is shown in Figure 6 (y-axis) as the better-ear three-frequency average unaided threshold. Age at time of testing (in months) is shown on the x-axis. Performance scores for vowel and consonant contrasts, displayed as the circles in the graph, are represented as percent confidence that the head-turn responses were not random. The results indicate that 1) the aided children were able to perform the task; 2) vowel contrasts were perceived quite well regardless of degree of hearing loss; and 3) consonant contrasts were perceived less well than vowels, particularly in children with greater degrees of hearing loss.
Figure 6.
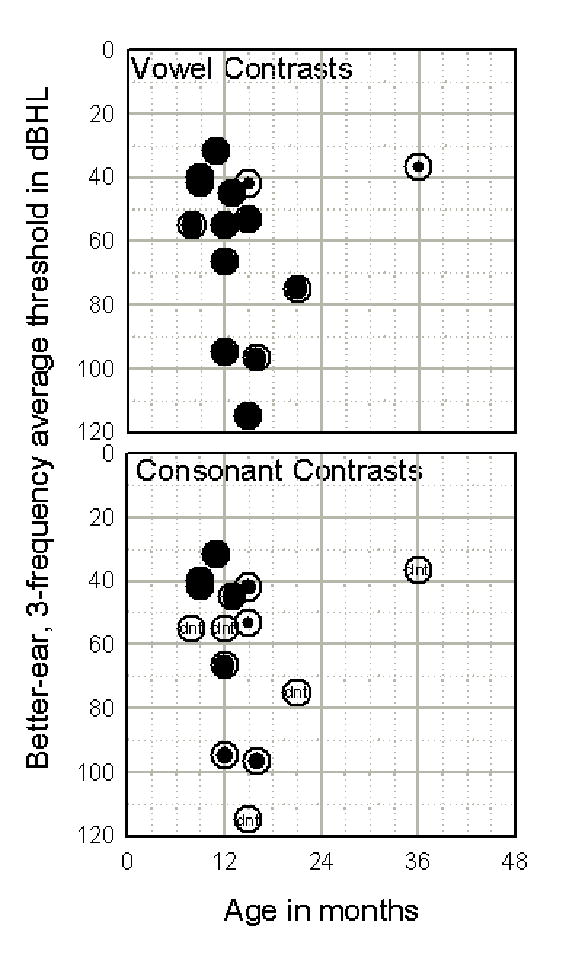
Performance of aided children on VRASPAC vowel and consonant contrasts as a function of hearing loss and age at time of testing. Confidence is represented by the radius of the filled circle relative to the open circle.
4.0. Discussion
The major challenge in developing tests that assess auditory capacity in infants and toddlers is to eliminate, or account for, non-auditory and task-related variables. Underlying this concept is the acknowledgment that children’s abilities as well as levels of interest and attentiveness will vary due to maturity, experience, current state, knowledge, processing skills and motor skills. Although these variables can not be completely controlled, their confounding influences may be diminished through careful test construction and the skill of the person administering the test.
In assessing auditory capacity, the child needs to be engaged in tasks that tap into his or her current abilities, needs, and interests. From 6 to 12 months, a child has the ability to turn his or her head and look at a sound source. After 12 months, the child becomes much more interested in developing the motor skills that will enable active exploration of the environment. To the extent that performance on VRASPAC decreases after 12 months and that there is an age range in which none of the other tests is appropriate, we have not been successful in achieving our goal of eliminating task-related effects across the targeted age range. As a result of these findings, continued test development is warranted for children between 1 and 3 years of age. More creative ways are being considered through use of less formal testing techniques. For example, children of this age are very responsive to social interaction, particularly with their caregivers. Integrating auditory testing into a type of scripted interaction between child and caregiver may prove to be a more successful transition for children too old for VRASPAC and too young for PLAYSPAC or OLIMSPAC.
There were a number of young children, hearing and hearing-impaired, for whom no usable data were obtained. These children either were not able to be trained on the task or were too inattentive to complete testing. An alternate direction may be to reduce reliance on behavioral measures in favor of electrophysiological cortical measures, such as the Acoustic Change Complex [37,38,39].
Software development has been labor-intensive for the four tests that measure speech pattern contrast perception. There have been many upgrades over the past several years while we’ve gained experience testing children of different ages and degrees of hearing loss. For instance, we originally used CV stimuli with the early test prototypes [20,23]. Because of technical difficulties with the AV files for OLIMSPAC, we re-recorded the stimuli using VCVs. One advantage of VCV stimuli is that transitions between vowels and consonants are present in both initial and final vowel positions. The change from CV to VCV was shown to improve OLIMSPAC scores [40]. Future studies are needed to determine whether the use of VCV stimuli scores also yield superior scores for VRASPAC, PLAYSPAC, and VIDSPAC relative to CV stimuli.
In another example, no-change trials were incorporated in the first prototype of VRASPAC [20] to reduce tester effects and biases. We found that those trials substantially extended the duration of testing for each contrast, reducing the child’s attention to the task. By discontinuing the no-change trials, test efficiency was markedly improved but at the expense of an increased risk of tester bias. Further development of VRASPAC is needed to determine how best to code an overt or subtle response to a phonetic change that is not a head turn, such as eye widening. One solution in the short term is to enlist the aid of a test assistant who can observe responses not easily seen by the tester. However, this solution reduces the objectivity of the test. Future development may consider an observer-based psychophysical procedure [41], in which the masked observer documents possible child responses to the contrast. We also are interested in upgrading the VRASPAC software to interface with more up-to-date video reinforcers, which may improve attentiveness for infants over the age of 12 months.
One difficulty encountered during this early phase of data collection has been the need for return visits. More than one test session is often required to complete a test, particularly for VRASPAC and PLAYSPAC. Parents of children with normal hearing sometimes prefer not to schedule additional research appointments. As a result, the greatest amount of VRASPAC data on normally hearing children comes from vowel height and place, which are the first contrasts assessed.
Despite the fact that additional test development is needed, the current tests that comprise BATIT offer much flexibility for assessing young children. If we are unable to test a child on one task, we often try a different one. It may be the case that we first attempt PLAYSPAC with a 2- to 3-year-old child. If the child is not cooperative in performing the task, we might then attempt OLIMSPAC. Conversely, some children may be very shy or nonverbal and won’t repeat the syllables during OLIMSPAC. In such cases we might attempt PLAYSPAC or even VIDSPAC if the child is a little older. We also have been successful in administering VRASPAC to older toddlers who are developmentally delayed.
OLIMSPAC differs from the other tests of BATIT in that a verbal response is required. When comparing performance between OLIMSPAC and PLAYSPAC or VIDSPAC within the same child, we sometimes observe lower scores for OLIMSPAC even though the perceptual task is the same. One explanation for this discrepancy is that OLIMSPAC is constrained by the child’s articulation. Thus, a child who misarticulates many consonants will have a depressed score. Although OLIMSPAC may not capture auditory perceptual capability exclusively, it yields data that are much more reflective of the child’s communication skills. Further, we are not assessing what the child says but, rather, which of the nonsense syllables the child is trying to imitate. This task, therefore, may bring us closest to an estimate of the child’s auditory capacity.
5.0. Summary
With the implementation of newborn hearing screening and early identification of hearing loss, there is a pressing need for development of assessment tools to measure auditory perceptual capabilities in infants and toddlers. We have developed a progressive test battery to respond to this clinical need, but also to address specific research questions about auditory capacity and performance in young children with hearing loss. We’ve taken an approach in accordance with auditory perceptual development, specifically phonetic discrimination (Level II) and word recognition (Level III). The greatest effort has entailed development of Level II tasks for infants and toddlers. Although much progress has been made during the past several years, additional test development remains.
As has always been the position in audiological assessment, a battery approach represents the standard. The tests described in this review are not meant to replace other existing measures or parent rating scales. Rather, these new tests in combination with other existing measures should provide a more complete profile on the young child with hearing loss.
Acknowledgments
This work is funded by the National Institute on Deafness and Other Communication Disorders of the National Institutes of Health grant R01DC006238 (House Ear Institute). Initial development of OLIMSPAC was funded under grant R01 DC004433 (UCLA). We recognize the important contributions of Jean L. DesJardin, Karen C. Johnson, Leslie Visser-Dumont, Danielle Dzubak, Sophie Ambrose, Donna Thal, and Carren Stika to this research.
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
References
- 1.Yoshinaga-Itano C, Sedey AL, Coutler DK, Mehl AL. Language of early- and later-identified children with hearing loss. Pediatr. 1998;5:1161–1171. doi: 10.1542/peds.102.5.1161. [DOI] [PubMed] [Google Scholar]
- 2.Moeller MP. Early intervention and language development in children who are deaf and hard of hearing. Pediatr. 2000;106:1–9. doi: 10.1542/peds.106.3.e43. [DOI] [PubMed] [Google Scholar]
- 3.Johnson KC, Winter ME. Audiologic assessment of infants and toddlers. Volta Rev. 2003;103:221–251. [Google Scholar]
- 4.Seewald RC, Cornelisse LE, Ramji KV, Sinclair ST, Moodie KS, Jamieson DG. DSL v4.1 for Windows: A software implementation of the desired sensation level (DSL[i/o] method for fitting linear gain and wide-dynamic-range compression hearing instruments. Hearing Health Care Research Unit, The University of Western Ontario; London Ontario, Canada: 1997. [Google Scholar]
- 5.Aslin RN, Smith LB. Perceptual development. Ann Rev Psychol. 1988;39:435–473. doi: 10.1146/annurev.ps.39.020188.002251. [DOI] [PubMed] [Google Scholar]
- 6.Carney AE. Audition and the development of oral communication competency. In: Bess FH, Gravel JS, Tharpe AM, editors. Amplification for Children with Auditory Deficits. Bill Wilkerson Center Press; Nashville: 1996. pp. 29–54. [Google Scholar]
- 7.Ling AH. Schedules of development in audition speech language communication for hearing-impaired infants and their parents. Washington, D.C.: The Alexander Graham Bell Association for the Deaf, Inc.; 1977. [Google Scholar]
- 8.Zimmerman-Phillips S, Robbins AM, Osberger MJ. Assessing cochlear implant benefit in very young children. Ann Otol Rhinol Laryngol. 2000;109(Suppl 185):42–43. doi: 10.1177/0003489400109s1217. [DOI] [PubMed] [Google Scholar]
- 9.Eilers RE, Wilson WR, Moore JM. Developmental changes in speech discrimination in infants. J Speech Hear Res. 1977;20:766–780. doi: 10.1044/jshr.2004.766. [DOI] [PubMed] [Google Scholar]
- 10.Dawson PW, Nott PE, Clark GM, Cowan RSC. A modification of play audiometry to assess speech discrimination ability in severe-profoundly deaf 2-to-4 year old children. Ear Hear. 1998;19:371–384. doi: 10.1097/00003446-199810000-00004. [DOI] [PubMed] [Google Scholar]
- 11.Elliott LL, Katz D. Development of a new children’s test of speech discrimination (Technical Manual) Auditec; St. Louis: 1980. [Google Scholar]
- 12.Moog JS, Geers AE. Early Speech Perception Test for profoundly hearing-impaired children. Central Institute for the Deaf; St. Louis: 1990. [Google Scholar]
- 13.Jerger S, Jerger J. Pediatric Speech Intelligibility Test. Auditec; St. Louis: 1984. [Google Scholar]
- 14.Kirk KI, Pisoni DB, Osberger MJ. MJ Lexical effects of spoken word recognition by pediatric cochlear implant users. Ear Hear. 1995;16:470–481. doi: 10.1097/00003446-199510000-00004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Haskins H. Unpublished Master’s thesis. Northwestern University; 1949. A phonetically balanced test of speech discrimination for children. [Google Scholar]
- 16.Gelnett D, Sumida A, Nilsson M, Soli SD. Development of the Hearing In Noise Test for Children (HINT-C) American Academy of Audiology; Dallas: 1995. [Google Scholar]
- 17.Boothroyd A. Auditory perception of speech contrasts by subjects with sensorineural hearing loss. J Speech Hear Res. 1984;27:134–144. doi: 10.1044/jshr.2701.134. [DOI] [PubMed] [Google Scholar]
- 18.Boothroyd A. Measuring auditory speech-perception capacity in young children. In: Seewald RC, Bamford JM, editors. A Sound Foundation through Early Amplification: Proceedings of the 3rd International Conference; Phonak AG. 2005. pp. 129–140. [Google Scholar]
- 19.Boothroyd A, Eisenberg L, Martinez A. VIPSPAC, Version 4.3. House Ear Institute; Los Angeles: 2006. [Google Scholar]
- 20.Eisenberg LS, Martinez AS, Boothroyd A. Perception of phonetic contrasts in infants: Development of the VRASPAC. In: Miyamoto RT, editor. Cochlear Implants; International Congress Series 1273; Elsevier, Amsterdam. 2004. pp. 364–367. [Google Scholar]
- 21.Boothroyd A. Evaluation of speech production in the hearing-impaired: Some benefits of forced-choice testing. J Speech Hear Res. 1985;28:185–196. doi: 10.1044/jshr.2802.185. [DOI] [PubMed] [Google Scholar]
- 22.Boothroyd A, Eisenberg L, Martinez A. OLIMSPAC, Version 3.1d. House Ear Institute; Los Angeles: 2005. [Google Scholar]
- 23.Eisenberg LS, Martinez AS, Boothroyd A. Auditory-visual and auditory-only perception of phonetic contrasts in children. Volta Rev. 2003;103:327–346. [Google Scholar]
- 24.Kosky C, Boothroyd A. Validation of an on-line implementation of the Imitative Test of Speech Pattern Contrast Perception (IMSPAC) J Amer Acad Audiol. 2003;14:72–83. doi: 10.3766/jaaa.14.2.3. [DOI] [PubMed] [Google Scholar]
- 25.Boothroyd A, Hanin L, Eran O. Speech perception and production in children with hearing impairment. In: Bess FH, Gravel JS, Tharpe AM, editors. Amplification for Children with Auditory Deficits. Bill Wilkerson Center Press; Nashville: 1996. pp. 55–74. [Google Scholar]
- 26.Boothroyd A. Speech perception measures and their role in the evaluation of hearing aid performance in a pediatric population. In: Feigin JA, Stelmachowicz PG, editors. Pediatric Amplification: Proceedings of the 1991 National Conference, Boys Town National Research Hospital; Omaha. 1991. pp. 77–99. [Google Scholar]
- 27.Boothroyd A. VIDSPAC, Version 4.0. Graduate Center, City University of New York; New York: 2006. [Google Scholar]
- 28.Eisenberg LS, Shannon RV, Martinez AS, Wygonski J, Boothroyd A. Speech recognition with reduced spectral cues as a function of age. J Acoust Soc Amer. 2000;107:2704–2710. doi: 10.1121/1.428656. [DOI] [PubMed] [Google Scholar]
- 29.Pisoni DB, Geers AE. Working memory in deaf children with cochlear implants: Correlations between digit span and measures of spoken language processing. Ann Otol Rhinol Laryngol. 2000;109185(Suppl):92–93. doi: 10.1177/0003489400109s1240. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Boothroyd A. Developments in speech audiometry. Brit J Audiol (formerly Sound) 1968;2:3–10. [Google Scholar]
- 31.Boothroyd A. The discrimination of partially hearing children of frequency distorted speech. Int Audiol. 1967;6:136–145. [Google Scholar]
- 32.Boothroyd A. CASPA, Version 3.3a. San Diego: 2004. [Google Scholar]
- 33.MacKersie CL, Boothroyd A, Minnear D. Evaluation of the Computer-Assisted Speech Perception Test (CASPA) J Amer Acad Audiol. 2001;12:390–396. [PubMed] [Google Scholar]
- 34.Eisenberg LS, Martinez AS, Holowecky SR, Pogorelsky S. Recognition of lexically controlled words and sentences by children with normal hearing and children with cochlear implants. Ear Hear. 2002;23:450–462. doi: 10.1097/00003446-200210000-00007. [DOI] [PubMed] [Google Scholar]
- 35.MacWhinney B, Snow C. The child language data exchange system. J Child Lang. 1985;12:271–296. doi: 10.1017/s0305000900006449. [DOI] [PubMed] [Google Scholar]
- 36.Boothroyd A. LEXSEN. House Ear Institute; Los Angeles: 2005. [Google Scholar]
- 37.Martin BA, Boothroyd A. Cortical, auditory, event-related potentials in response to periodic and aperiodic stimuli with the same spectral envelope. Ear Hear. 1999;20:33–44. doi: 10.1097/00003446-199902000-00004. [DOI] [PubMed] [Google Scholar]
- 38.Martin BA, Boothroyd A. Cortical, auditory, evoked potentials in response to changes of spectrum and amplitude. J Acoust Soc Amer. 2000;107:2155–2161. doi: 10.1121/1.428556. [DOI] [PubMed] [Google Scholar]
- 39.Ostroff JM, Martin BA, Boothroyd A. Cortical evoked response to acoustic change within a syllable. Ear Hear. 1998;19:290–297. doi: 10.1097/00003446-199808000-00004. [DOI] [PubMed] [Google Scholar]
- 40.Martinez AS, Eisenberg LS, Boothroyd A, Johnson KC. Auditory-visual and auditory-only perception of CV and VCV stimuli in young children. 10th Symposium on Cochlear Implants in Children; Dallas. 2005. [Google Scholar]
- 41.Olsho LW, Koch EG, Halpin CF, Carter EA. An observer-based psychoacoustic procedure for use with young infants. Dev Psychol. 1987;23:627–240. [Google Scholar]