

Abstract
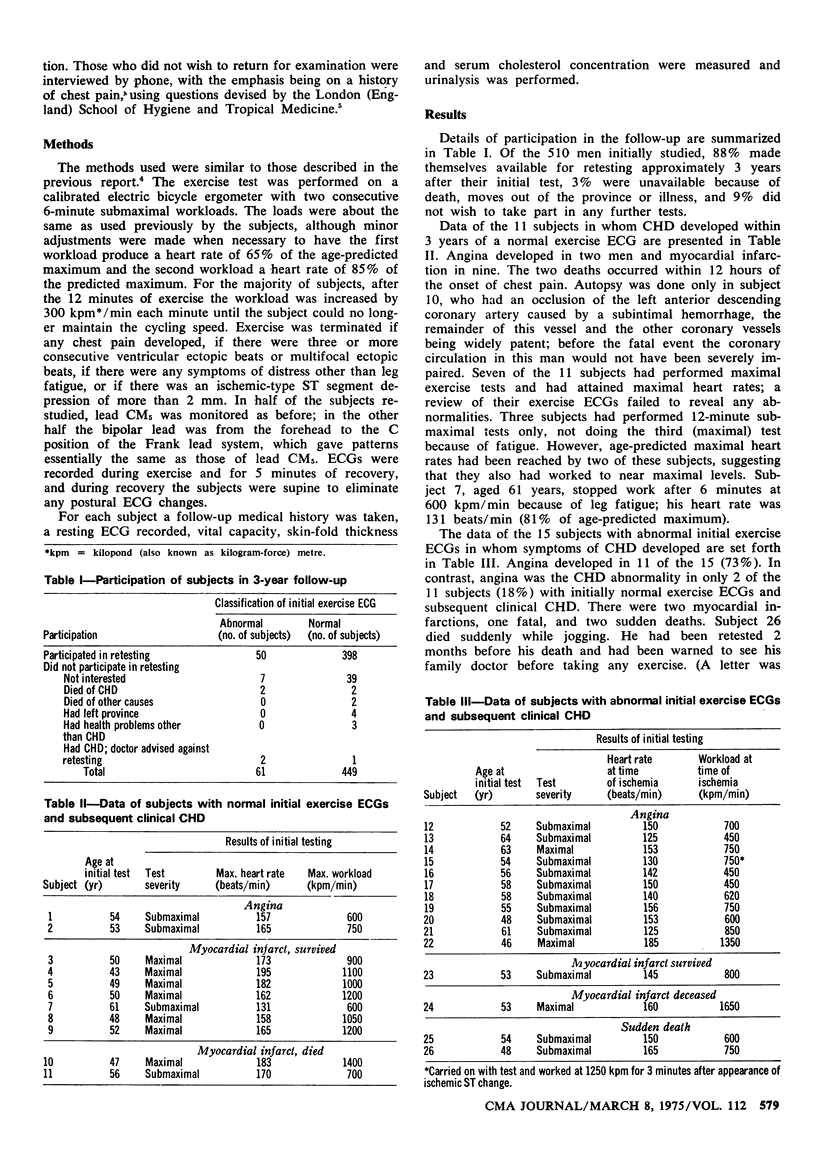
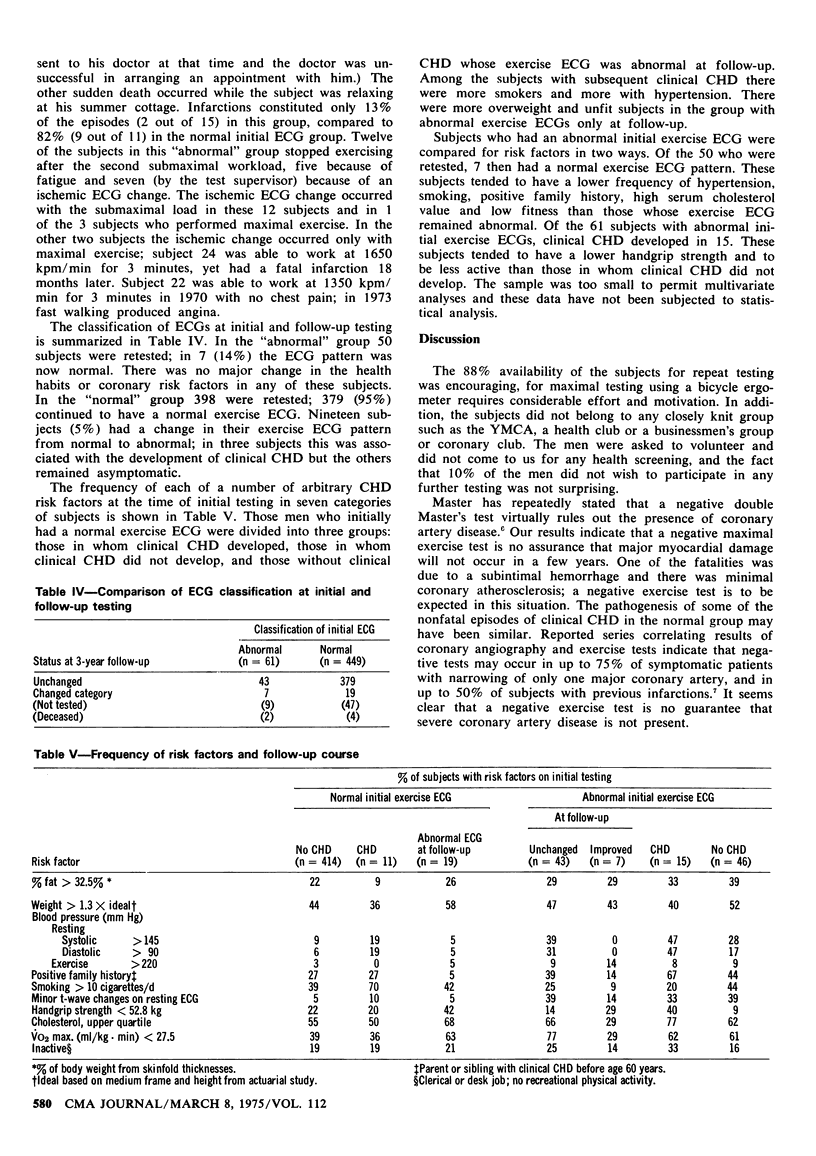
Electrocardiographic (ECG) changes during maximal bicycle exercise and risk factors for coronary heart disease (CHD) were studied in 510 male civic employees who were followed for 3 years. Clinical CHD developed in 15 (24.6 percent) of the 61 men with an ischemic exercise ECG on the initial examination and in 11 (2.4 percent) of the 449 subjects with a normal initial exercise ECG. A normal maximal exercise ECG is no guarantee that severe CHD does not exist and that a subject will not soon sustain major myocardial damage; and an ischemic exercise ECG does not necessarily indicate underlying CHD. In the former group angina was the most frequent clinical CHD episode; in the latter group, infarction. Among those with an abnormal initial exercise ECG, CHD was most likely to develop in association with a poor exercise capacity. Subjects with subsequent clinical CHD and those with abnormal ECGs after 3 years tended to have a higher frequency of risk factors; subjects whose abnormal ECGs reverted to normal after 3 years tended to have a lower frequency of risk factors.
Full text
PDF
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Anderson T. W. The changing pattern of ischemic heart disease. Can Med Assoc J. 1973 Jun 23;108(12):1500–1504. [PMC free article] [PubMed] [Google Scholar]
- Bruce R. A., McDonough J. R. Stress testing in screening for cardiovascular disease. Bull N Y Acad Med. 1969 Dec;45(12):1288–1305. [PMC free article] [PubMed] [Google Scholar]
- Cumming G. R., Borysyk L., Dufresne C. The maximal exercise ECG in asymptomatic men. Can Med Assoc J. 1972 Mar 18;106(6):649–653. [PMC free article] [PubMed] [Google Scholar]
- Froelicher V. F., Jr, Yanowitz F. G., Thompson A. J., Lancaster M. C. The correlation of coronary angiography and the electrocardiographic response to maximal treadmill testing in 76 asymptomatic men. Circulation. 1973 Sep;48(3):597–604. doi: 10.1161/01.cir.48.3.597. [DOI] [PubMed] [Google Scholar]
- Kattus A. A., Jorgensen C. R., Worden R. E., Alvaro A. B. S-T-segment depression with near-maximal exercise in detection of preclinical coronary heart disease. Circulation. 1971 Oct;44(4):585–595. doi: 10.1161/01.cir.44.4.585. [DOI] [PubMed] [Google Scholar]
- Mason R. E., Likar I., Biern R. O., Ross R. S. Multiple-lead exercise electrocardiography. Experience in 107 normal subjects and 67 patients with angina pectoris, and comparison with coronary cinearteriography in 84 patients. Circulation. 1967 Oct;36(4):517–525. doi: 10.1161/01.cir.36.4.517. [DOI] [PubMed] [Google Scholar]
- Master A. M. Exercise testing for evaluation of cardiac performance. Am J Cardiol. 1972 Nov;30(7):718–721. doi: 10.1016/0002-9149(72)90144-0. [DOI] [PubMed] [Google Scholar]