

Abstract
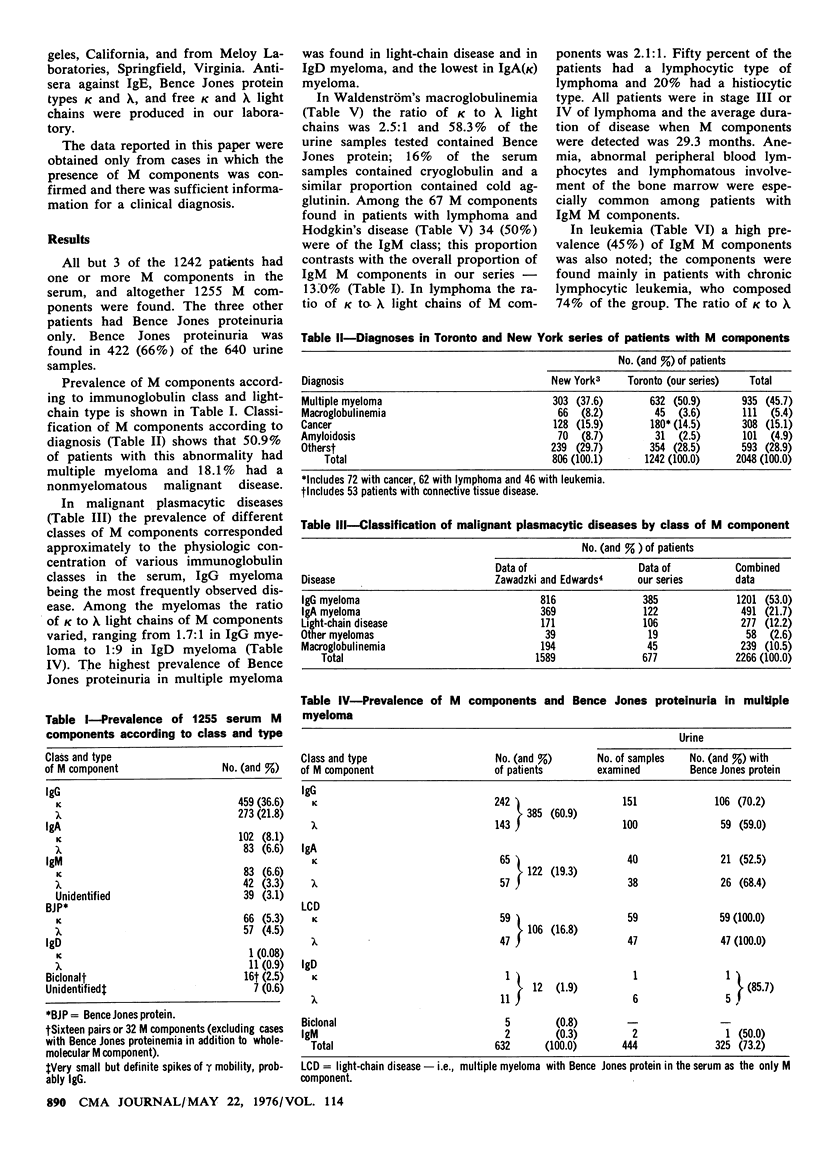
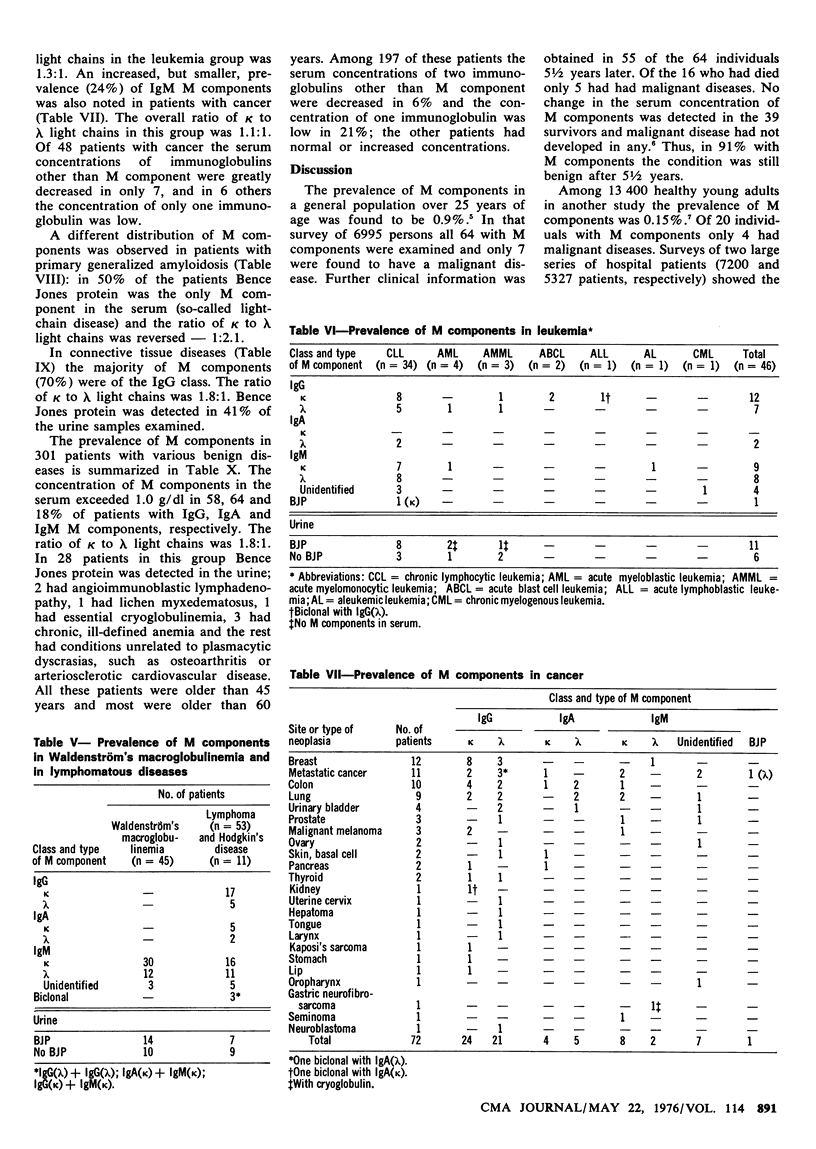
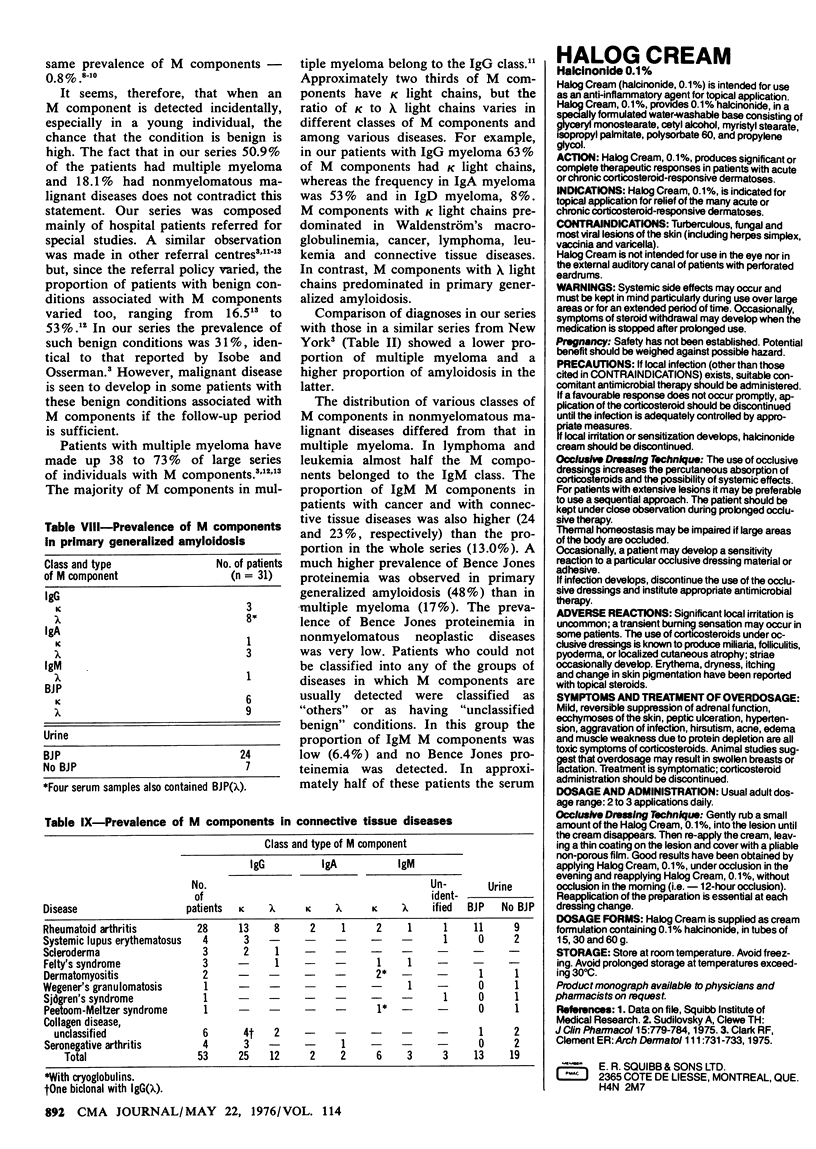
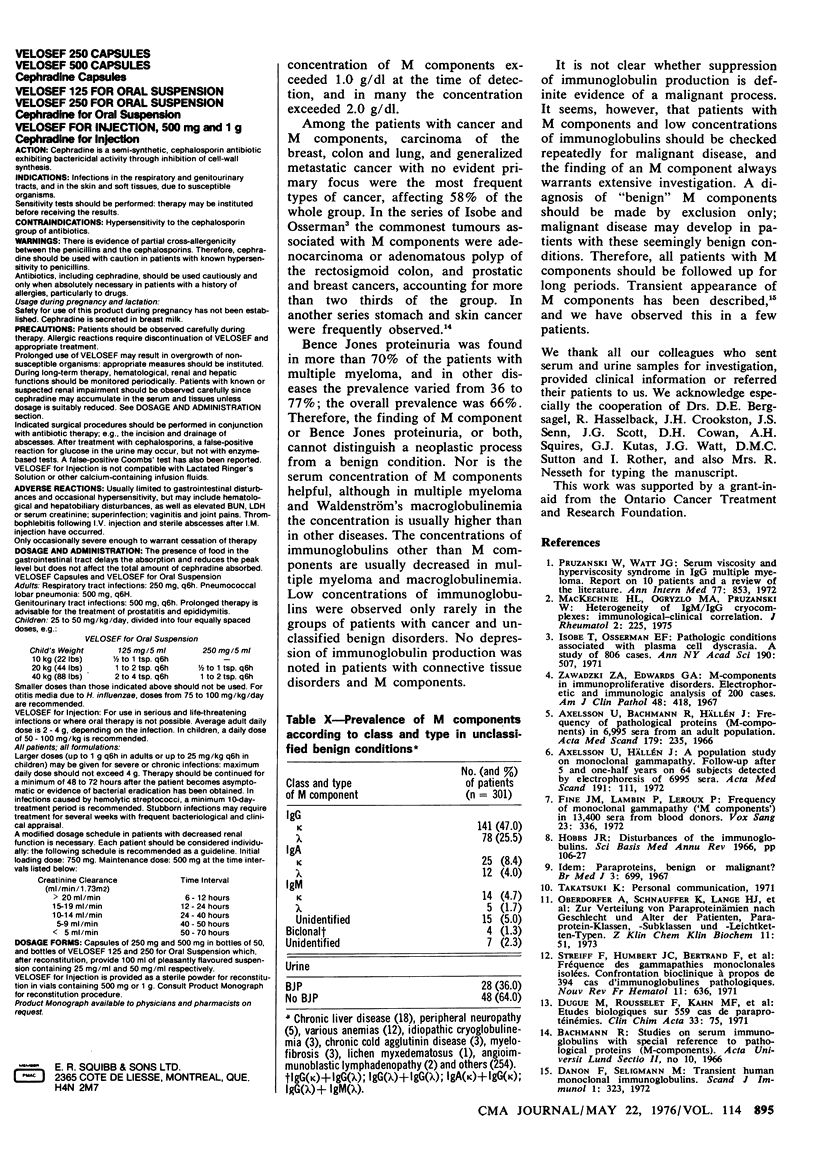
Among 1242 patients referred for immunologic investigation 1255 M components were detected in the serum. Of these patients 50.9% had multiple myeloma, 18.1% had nonmyelomatous malignant diseases such as macroglobulinemia, lymphoma, leukemia or cancer, 4.3% had connective tissue diseases, 2.5% had primary generalized amyloidosis (PGA) and the rest had various "benign" conditions. Whereas IgG was the commonest M component in multiple myeloma, connective tissue diseases and the other benign conditions, IgM was the commonest M component in lymphoma and leukemia; Bence Jones proteinemia was most frequently observed in PGA. The ratio of kappa to lambda light chains varied from 1.7:1 in IgG myeloma to 1:9 in IgD myeloma, and was 1:2.1 in PGA. Bence Jones protein was detected in 422 (66%) of 640 urine samples tested, the prevalence ranging from more than 70% in multiple myeloma and PGA to as low as 36% in various benign conditions. It is evident that the class and type of M components and the presence of Bence Jones proteinuria have no definite significance with regard to the diagnosis. Therefore, thorough investigation and follow-up at regular intervals are required when M components are detected.
Full text
PDF
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Axelsson U., Bachmann R., Hällén J. Frequency of pathological proteins (M-components) om 6,995 sera from an adult population. Acta Med Scand. 1966 Feb;179(2):235–247. doi: 10.1111/j.0954-6820.1966.tb05453.x. [DOI] [PubMed] [Google Scholar]
- Danon F., Seligmann M. Transient human monoclonal immunoglobulins. Scand J Immunol. 1972;1(4):323–328. doi: 10.1111/j.1365-3083.1972.tb03297.x. [DOI] [PubMed] [Google Scholar]
- Fine J. M., Lambin P., Leroux P. Frequency of monoclonal gammapathy ('M components') in 13,400 sera from blood donors. Vox Sang. 1972;23(4):336–343. doi: 10.1111/j.1423-0410.1972.tb03468.x. [DOI] [PubMed] [Google Scholar]
- Hobbs J. R. Disturbances of the immunoglobulins. Sci Basis Med Annu Rev. 1966:106–127. [PubMed] [Google Scholar]
- Isobe T., Osserman E. F. Pathologic conditions associated with plasma cell dyscrasias: a study of 806 cases. Ann N Y Acad Sci. 1971 Dec 31;190:507–518. doi: 10.1111/j.1749-6632.1971.tb13560.x. [DOI] [PubMed] [Google Scholar]
- MacKechnie H. L., Ogryzlo M. A., Pruzanski W. Heterogeneity of IgM/IgG cryocomplexes: immunological-clinical correlation. J Rheumatol. 1975 Jun;2(2):225–240. [PubMed] [Google Scholar]
- Oberdorfer A., Schnauffer K., Lange H. J., Neiss A. Zur Verteilung von Paraproteinämien nach Geschlecht und Alter der Patienten, Paraprotein-Klassen, -Subklassen und -Leichtketten-Typen. Z Klin Chem Klin Biochem. 1973 Feb;11(2):51–64. [PubMed] [Google Scholar]
- Zawadzki Z. A., Edwards G. A. M-components in immunoproliferative disorders. Electrophoretic and immunologic analysis of 200 cases. Am J Clin Pathol. 1967 Oct;48(4):418–430. doi: 10.1093/ajcp/48.4.418. [DOI] [PubMed] [Google Scholar]