

BACKGROUND
In 1952, Professor Bryan Brooke described his technique for everting an ileostomy in order to minimise skin excoriation, which continues to be used today.1 The classical method of colostomy formation involves suturing the cut end of the bowel directly to the skin resulting in a flush stoma.2 We propose the eversion-technique be used for the end colostomy in order to spout the colostomy in a similar fashion to the Brooke ileostomy. This allows easier and more effective application of a stoma appliance.
TECHNIQUE
The end of the bowel wall is sutured to the skin by means of a 3/0 absorbable suture. The suture first passes through the skin, followed by a seromuscular bite taken 1.5 cm proximal to the end of the bowel; the suture is then passed through the full thickness of the end of the bowel wall. Four of these sutures are placed at quarterly intervals and then secured. Additional sutures are placed as required between these points passing solely between skin and the end of the bowel (Fig. 1).
Figure 1.
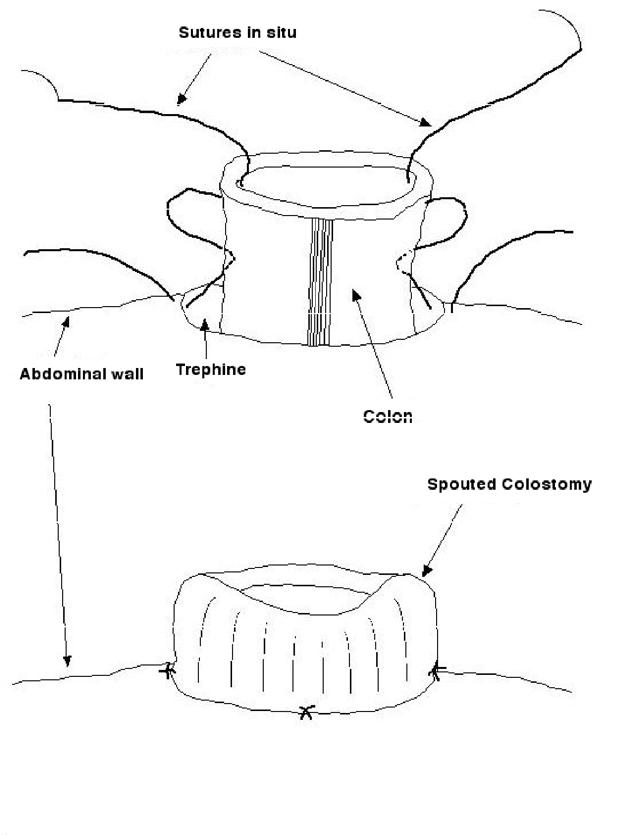
Diagramatical representation of the proposed technique.
DISCUSSION
Not only does the Brooke ileostomy help prevent skin excoriation, it also facilitates the application of a closely approximated appliance to the base of the stoma, thereby minimising ingress of fluid under the free edge of the stoma appliance which may subsequently lead to leakage. This benefit can also be achieved with the formation of a spouted colostomy, allowing easier fitting of a stoma appliance and minimising the risk of leakage associated with any liquid effluent. This technique has received favourable feedback from stoma therapists locally.
References
- 1.Brooke BN. The management of an ileostomy, including its complications. Lancet. 1952;2:102–4. doi: 10.1016/s0140-6736(52)92149-1. [DOI] [PubMed] [Google Scholar]
- 2.Kirk RM. Basic Surgical Techniques. 5th edn. Edinburgh: Churchill Livingstone; 2002. [Google Scholar]